Prehospital Cardiopulmonary Resuscitation in Patients with Suspected Severe Traumatic Brain Injury: A BRAIN PROTECT Sub-Analysis
Floor J. Mansvelder, Elise Beijer, Anthony R. Absalom, Frank W. Bloemers, Dennis Den Hartog, Nico Hoogerwerf, Esther M. M. Van Lieshout, Stephan A. Loer, Joukje van der Naalt, Lothar A. Schwarte, Sebastiaan M. Bossers, Patrick Schober

TL;DR
This study examines outcomes of patients with severe traumatic brain injury who received prehospital CPR, finding that some survivors achieved good neurological recovery.
Contribution
The study provides new insights into the prognosis and characteristics of TBI patients requiring prehospital CPR, a group often excluded from research.
Findings
30-day mortality was 79.9%, but 45.7% of survivors achieved moderate disability or good recovery at discharge.
Outcomes did not differ between isolated and non-isolated TBI patients.
Shockable initial rhythm and lack of anisocoria were characteristics associated with better survival.
Abstract
Background/Objectives: Severe traumatic brain injury (TBI) carries high mortality, and outcomes are particularly poor when prehospital cardiopulmonary resuscitation (CPR) is required. Because these patients are often excluded from research, epidemiological data and prognostic insights are limited. This study aimed to describe characteristics and outcomes of patients with suspected severe TBI who received prehospital CPR. Methods: We performed a sub-analysis of the prospectively collected multicenter BRAIN-PROTECT registry, including all patients with suspected severe TBI who underwent prehospital CPR and were transported to a participating trauma center. Results: A total of 256 patients with suspected severe TBI who received prehospital CPR were included. Early mortality was high, with 22.6% declared dead in the emergency department and an additional 28.9% within 24 h, resulting in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
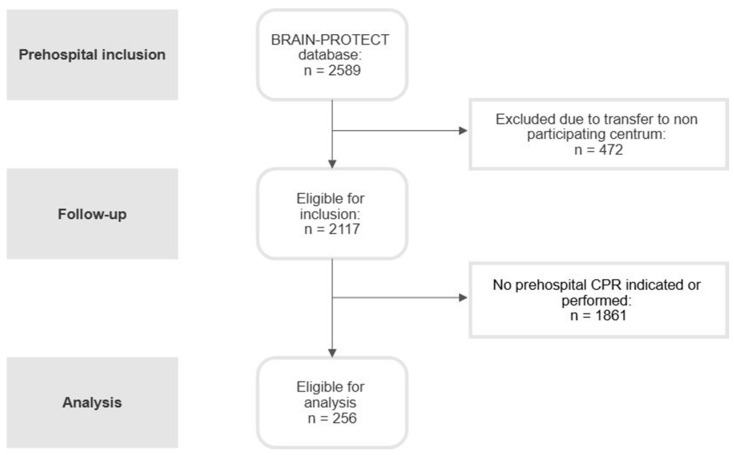 Figure 1
Figure 1- —Hersenstichting
- —Stichting Achmea Gezondheidszorg
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrest and Resuscitation · Traumatic Brain Injury and Neurovascular Disturbances · Trauma and Emergency Care Studies
1. Introduction
Severe traumatic brain injury (TBI) is a major global health problem, associated with high mortality and poor functional outcomes [1,2,3,4,5]. After the first hit of traumatic injury, preventing secondary brain injury becomes the primary focus of early care, starting in the prehospital setting [6,7,8]. Key priorities include preventing hypoxia, avoiding hypotension, maintaining normocapnia, and addressing other major injuries and issues such as major hemorrhage [9,10,11,12]. Failure to achieve these physiological targets is strongly associated with worse outcomes.
Prehospital cardiopulmonary resuscitation (CPR) in patients with severe TBI represents an even more critical challenge. From a pathophysiological perspective, the need for CPR, which involves an additional period of low-flow or no-flow cerebral perfusion on top of the primary brain injury, substantially increases the risk of secondary brain injury [13].
Despite their clinical relevance, patients who receive prehospital CPR are frequently excluded from TBI research because including this subgroup, with its overwhelmingly high mortality rate, introduces significant heterogeneity that can confound analyses aimed at evaluating standard TBI care [14,15]. Conversely, studies on CPR often exclude trauma patients altogether, and research on traumatic cardiac arrest typically does not distinguish between TBI and non-TBI causes [16,17,18]. Consequently, TBI patients requiring CPR remain only sparsely described in the literature. In clinical practice, however, these cases do occur, and clinicians are often faced with uncertainty regarding prognosis and appropriate management strategies.
Against this background, current trauma and neurotrauma guidelines offer no specific recommendations for the management of this specific group of patients with suspected severe TBI who undergo prehospital CPR [19,20]. As a result, epidemiological data and patient outcome estimates are lacking, and it is unclear to what extent historically poor results are truly generalizable. Moreover, possible differences in outcomes between isolated TBI CPR cases and patients with TBI and additional extracranial injuries, and the implications for survival and neurological recovery, are underreported.
To address this knowledge gap, this study aims to describe the prehospital characteristics and in-hospital outcomes of patients with suspected severe TBI who receive prehospital CPR. The overarching aim was to explore whether survival and recovery are uniformly poor, suggesting that continuation of aggressive treatment may be futile, or whether specific patient subgroups demonstrate sufficient potential for meaningful recovery to warrant ongoing care.
2. Materials and Methods
2.1. Study Design, Setting, Participants
This study is a sub-analysis of prospectively collected data from the BRAIN-PROTECT (Brain Injury; Prehospital Registry of Outcomes, Treatments and Epidemiology of Cerebral Trauma) study, a multicenter observational cohort study aimed at understanding the prehospital management of patients with severe TBI in the Netherlands [21]. Data were collected between February 2012 and December 2017. Inclusion took place when a patient with suspected severe TBI was treated by a Helicopter Emergency Medical Services (HEMS) team. In The Netherlands, suspected severe traumatic brain injury is a primary dispatch criterion for HEMS activation [22]. This suspicion is based on a Glasgow Coma Scale (GCS) score of 8 or lower in combination with a trauma mechanism or clinical findings suggestive of TBI. The study protocol was reviewed by the Medical Research Ethics Committees of Amsterdam University Medical Center (location Vrije Universiteit Medical Center) and Erasmus Medical Center in Rotterdam. These committees determined that the research did not fall under the Dutch Medical Research Involving Human Subjects Act and the requirement for obtaining informed consent was waived [23]. Reporting of the study followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines [24].
2.2. Data Collection and Outcome Measures
For this study, we included and analyzed all patients with suspected severe TBI who underwent prehospital CPR and were transported to a participating trauma center. Patients who were declared dead on the scene were not included. Collected data included demographic characteristics, medication use, American Society of Anesthesiologists (ASA) classification, distance to hospital, duration of CPR, presence of shockable or non-shockable rhythms, prehospital Glasgow Coma Scale (GCS) score, and Injury Severity Score (ISS). Furthermore, data were collected on dispatch category, defined as primary dispatch when Helicopter Emergency Medical Services (HEMS) were activated directly at the time of the emergency call, and secondary dispatch when HEMS was requested by the ambulance team on scene due to clinical deterioration or reassessment of injury severity. The primary outcome of the study was 30-day mortality. Secondary outcomes included mortality in the emergency department, 24 h mortality, neurological status at discharge assessed by the Glasgow Outcome Scale (GOS), length of hospital stay, and length of ICU stay.
2.3. Statistical Analyses
Data were analyzed using Stata 18 (StataCorp, College Station, TX, USA). The previously published BRAIN-PROTECT study protocol [23] includes a detailed statistical analysis plan and a power calculation. Data distribution was evaluated using histograms, Shapiro–Wilk tests, and quantile-quantile plots. Continuous variables are presented as means ± standard deviation or medians [25th, 75th percentile], while categorical variables are reported as counts and percentages. For the comparison of two groups, appropriate statistical tests were applied based on variable type and distribution: continuous variables were compared using Student’s t-tests or Mann–Whitney U tests, and dichotomous variables were compared using χ^2^ tests or Fisher’s exact tests.
Subgroup analyses were performed in patients with confirmed TBI (head Abbreviated Injury Scale score of 3 or higher) and, separately, in patients with isolated TBI (head Abbreviated Injury Scale score of 3 or higher, scores for all other Abbreviated Injury Scales of 2 or lower) compared with those with non-isolated TBI. All analyses were conducted using complete cases only. Given the substantial proportion of missing data across several key variables, including CPR characteristics and injury severity measures, no imputation techniques were applied. Analyses were therefore explicitly designed to be descriptive and exploratory in nature rather than inferential. Denominators for each variable and analysis are reported throughout the tables to ensure transparency regarding data completeness.
3. Results
3.1. Patient Demographics and Injury Characteristics
A total of 2589 patients were registered in the BRAIN-PROTECT database. After excluding 472 patients who were transferred to non-participating centers, 2117 patients were eligible for inclusion. Of these, 1861 patients were excluded because they either did not require prehospital CPR or, in cases of cardiac arrest on scene, because CPR was not initiated or was terminated early. The final study cohort included in the analysis consisted of 256 patients who underwent prehospital CPR and were transported to a participating trauma center (Figure 1).
Patient characteristics are summarized in Table 1. The median age of included patients was 46.0 years (IQR 25–66 years), and 72.3% of patients were male. The initial on-scene neurological status was profoundly impaired, with a median prehospital GCS of 3 (IQR 3–3). The median ISS was 34 (IQR 25–43), which reflects a severely traumatized patient population. Falls from height (26.2%) and traffic-related mechanisms (64.3%) were the predominant causes of injury, and most incidents occurred on the road (63.8%). Nearly all injuries were blunt in nature (97.2%), with only a very small proportion of penetrating trauma. Confirmed TBI was present in 92.9% of patients, and 23.2% had isolated TBI. Major prehospital hemorrhage (estimated >1000 mL) was present in 44.6% of included patients. A detailed overview of missing data for all variables included in the analysis is provided in Supplementary Table S1.
3.2. Clinical Outcomes
Early outcomes were poor: 22.6% were declared dead in the emergency department and an additional 28.9% within the first 24 h, resulting in 48.5% survival beyond 24 h (Table 1). At 30 days, mortality reached 79.9%, resulting in 48 surviving patients (20.1%). In terms of functional outcome, around 45.7% of patients alive at discharge showed good recovery or only moderate disability, while the other half showed severe disability or a vegetative state.
3.3. Patient Characteristics of Survivors and Non-Survivors
Patient characteristics stratified by 30-day survival are presented in Table 2. Survivors and non-survivors did not differ in age or sex distribution. However, survivors had slightly higher initial GCS values (p < 0.001) and lower injury severity (ISS median 29 vs. 34, p = 0.024). Injury mechanism and location did not significantly differ between groups. Confirmed TBI was more common among non-survivors (95.6% vs. 80.6%, p = 0.003), and major hemorrhage occurred significantly more often in non-survivors (55.0% vs. 14.7%, p < 0.001).
3.4. CPR Specifics
Prehospital CPR characteristics are shown in Table 3. Arrests were witnessed at similar rates in both groups. Although not statistically significant, survivors more often had bystander-initiated CPR in our sample of patients, while non-survivors more frequently received no bystander CPR. AED deployment did not differ between groups. Etiology of arrest differed significantly (p = 0.040): cardiac or submersion-related causes were more frequent in survivors, whereas traumatic arrest predominated among non-survivors. CPR Initial rhythm showed the strongest association with survival: 35.3% of survivors presented with VF (Ventricular Fibrillation) compared with 5.2% of non-survivors (p < 0.001). Moreover, when grouped as shockable versus non-shockable rhythms, 12.5% of survivors had a shockable rhythm versus only 4.7% of non-survivors (p < 0.001). A substantial proportion of patients had no documented initial rhythm during resuscitation. Survival differed across rhythm categories, with the highest survival observed among patients with shockable rhythms, the lowest survival among those with non-shockable rhythms, and intermediate survival among patients with unknown rhythm documentation. Early ROSC (<20 min) was also significantly more common in survivors (100% vs. 79%, p = 0.009).
3.5. Prehospital Clinical Findings and Interventions
Prehospital clinical parameters and interventions are listed in Table 4. Pupillary reactivity differed substantially between groups: 41.0% of survivors had reactive pupils compared with 12.4% of non-survivors (p < 0.001). Anisocoria did not differ between groups. Airway management was performed in nearly all patients, predominantly via endotracheal intubation. Although airway management was statistically more common in non-survivors (100%) than survivors (97%) (p = 0.047), the absolute difference was small. Therefore, despite reaching statistical significance, the clinical relevance of this finding is limited. Advanced procedures such as thoracostomy, needle decompression, and chest tube placement were infrequent and showed no significant differences. Transport mode (helicopter vs. ground transport) and dispatch category (primary vs. secondary) were also comparable. Air distance from the scene to the hospital did not differ between survivors and non-survivors.
3.6. Subgroup Analysis: Isolated TBI
Mortality and clinical outcomes for patients with isolated versus non-isolated TBI are summarized in Table 5. Early clinical outcomes showed no significant differences between groups (p = 0.120). Thirty-day mortality was nearly identical (80.8% vs. 80.6%, p = 0.913). Functional outcomes at discharge were similarly distributed between isolated and non-isolated TBI (p = 0.184).
3.7. Subgroup Analysis: Confirmed TBI
In total, 152 patients had confirmed TBI, 12 had non-confirmed TBI, and for 87 patients, information on TBI confirmation was missing. Mortality at 30 days was significantly higher among patients with confirmed TBI compared with those without confirmed TBI (132 patients, 84.7%, versus 6 patients, 50.0%). Early outcomes, including death in the emergency department, death within 24 h after admission, and survival beyond 24 h, did not differ significantly between groups. Neurological outcome at discharge, assessed by the GOS, was significantly worse in patients with confirmed TBI (p < 0.001).
3.8. Subgroup Analysis: Surviving Patients with Good Recovery at Discharge
Thirteen patients achieved a good recovery at discharge (Table 6). These patients were not limited to young age/certain age groups (17–74 years), certain types of mechanism of injury, or specific injury severity (ISS 8–41). Although most presented with a GCS of 3, all 13 achieved prehospital ROSC, and most had shockable rhythms such as VF. Anisocoria was absent in nearly all cases.
4. Discussion
4.1. Key Findings
This study examined a scarcely described, clinically complex and rare population: patients with severe TBI for whom CPR in the prehospital setting in the Netherlands was initiated and who subsequently entered hospital-based care. The main descriptive finding of this study is that survival in this specific patient group, although limited, is not negligible. Mortality at 24 h was 51.5%, increasing to 79.9 at 30 days. However, the remaining 20.1% of patients who survived demonstrated that favorable outcomes are indeed possible. Notably, around half of these 30-day survivors achieved good to moderate neurological functional recovery at discharge.
Importantly, these results should be interpreted as conditional on resuscitation being attempted and on patients reaching hospital care; they therefore do not imply uniformly favorable outcomes after CPR in all TBI-related arrests. Rather, they indicate that once ROSC is achieved and hospital care is reached, the probability of survival and meaningful neurological recovery may be higher than is often assumed. In daily practice, TBI patients requiring CPR are often considered beyond meaningful recovery, and treatment is frequently regarded as futile. Our findings fill an important knowledge gap and provide a more accurate and nuanced view of the outcome potential for those who survive to definitive hospital care, thereby informing whether continued aggressive treatment may be justified in selected patients.
4.2. Interpretation/Clinical Implications
To advance this line of inquiry, it is important to identify and characterize the factors associated with an elevated mortality risk in patients with TBI who require prehospital CPR. Although the mortality rate within the cohort is high (79.9%), comparisons of survivors versus non-survivors yield useful insights. Non-survivors more often showed indicators of greater injury burden and physiological derangement, including higher ISS and a higher prevalence of major hemorrhage. In contrast, survivors more frequently presented with a shockable initial rhythm and all of these patients achieved prehospital ROSC.
The observed 100% mortality among patients who did not achieve prehospital ROSC highlights the extremely narrow therapeutic window in this population and underscores the critical importance of rapid, goal-directed prehospital intervention. In practical terms, these findings suggest that achieving early ROSC is a key prerequisite for any chance of survival, and they support continued efforts toward timely resuscitation to mitigate the cascade of secondary ischemic injury following cardiac arrest, correction of reversible causes, and rapid transport when ROSC is obtained.
Another notable finding is that the proportion of survivors achieving a favorable neurological outcome is comparable to that observed in the broader population of severe TBI patients who did not require CPR [21]. This suggests that, in a selected subset of patients who reach hospital care after successful resuscitation, cardiac arrest does not inevitably translate into universally poor neurological outcomes beyond the already high baseline risk associated with TBI. At the same time, however, it is important to consider that “suspected severe TBI” in the prehospital setting is a working diagnosis, and some patients may have had a primary non-traumatic cause of arrest (e.g., myocardial infarction or another medical event) with secondary trauma as a consequence of collapse. Consistent with this, when restricting the analysis to patients with confirmed clinically relevant head injury severity, survival was markedly lower, and favorable outcomes in the total cohort were to a large extent driven by patients without evidence of severe intracranial injury. Although the number of patients without confirmed TBI was relatively small compared with those with confirmed TBI, this contrast remains clinically informative and underscores the heterogeneity within the population of patients initially classified as having suspected severe TBI.
Importantly, this does not diminish the clinical relevance of our overall findings; rather, it highlights a key real-world challenge: in the prehospital environment, providers can often not reliably distinguish TBI-driven arrests from other causes. This diagnostic uncertainty should therefore be explicitly considered when deciding on initiation or continuation of CPR in patients with suspected TBI. In particular, patients with a shockable rhythm seem to have better outcomes; however, patients with PEA or even asystole have also survived with good recovery, advocating for a carefully selected, aggressive and well-coordinated resuscitation effort in patients with cardiac arrest and (suspected) TBI. Nevertheless, overall prognosis remains poor, and these observations should not be interpreted as justification for indiscriminate resuscitation, but rather as support for a nuanced, physiology-driven approach to decision-making in this high-risk population. Importantly, these observations should also be interpreted as descriptive and hypothesis-generating rather than as evidence of causal or generalizable treatment effects.
Historically, traumatic cardiac arrest was widely regarded as futile, including arrests associated with severe extracranial trauma. In recent years, this view has been challenged by an improved understanding of traumatic arrest pathophysiology and a reprioritization of resuscitation strategies, with emphasis on early identification and correction of reversible causes rather than immediate chest compressions. Structured approaches focusing on hemorrhage control, oxygenation, relief of tension pneumothorax, and management of cardiac tamponade have been associated with improved outcomes in selected patients [25]. The survival observed in the present cohort of patients with TBI and cardiac arrest may, at least in part, reflect the impact of these evolving resuscitation principles within modern prehospital trauma care.
In addition, a specific subgroup of patients with TBI-associated cardiac arrest may be explained by the concept of impact brain apnea [26,27]. In these cases, cardiac arrest occurs shortly following head impact, potentially in the absence of major structural brain injury, and is primarily driven by transient central apnea. When treated early with prompt airway management, oxygenation, and basic CPR to bridge the apneic period, spontaneous circulation and ventilation may be restored before substantial hypoxic brain injury develops. Although the incidence of impact brain apnea cannot be determined in the present cohort, this mechanism may partly explain the favorable outcomes observed in some patients, particularly those with early ROSC and good neurological recovery. This further supports the notion that TBI-associated cardiac arrest does not represent a uniform pathophysiological entity or prognosis.
Given the relatively young age of this patient population and the substantial disability-adjusted life years at stake, the potential for meaningful neurological recovery in a subset of patients underscores the broader societal relevance of this condition. In this context, our findings suggest that continued refinement of prehospital trauma care, including rapid assessment, controlled resuscitation, and timely transport, may influence outcomes in selected patients with severe TBI and cardiac arrest.
4.3. Comparison with Literature
Reported survival rates of traumatic cardiac arrest vary widely across studies, ranging from approximately 4% to 40%, depending on inclusion criteria, case mix, and definitions of survival [28,29,30], largely due to differences in study design and case selection [27]. Importantly, many of these studies report overall survival rather than neurologically meaningful recovery, which is substantially less frequent [31].
While the aforementioned literature describes traumatic cardiac arrest in general and does not consistently distinguish between TBI and non-TBI patients, to our knowledge, only one previous study has examined a comparable population of patients with severe TBI requiring prehospital CPR. Zhao et al. [32] analyzed a smaller cohort of 42 patients, reporting a 19% survival rate, with most survivors achieving favorable neurological outcomes. Our findings broadly align with these observations. In our larger national cohort, 20.1% of patients survived to 30 days, approximately half of whom achieved moderate to good neurological recovery at discharge. In both studies, favorable neurological signs, including preserved pupillary reactivity, were associated with survival.
When placed in a broader context beyond trauma, the survival rate observed in our cohort appears comparable to that reported for out-of-hospital cardiac arrest in the general Dutch population. In the Netherlands, survival after EMS-treated OHCA is approximately 23% [33]. However, this comparison should be interpreted cautiously because case mix and inclusion criteria differ substantially. Importantly, the present cohort is conditional on patients reaching hospital care. Nonetheless, the data suggest that outcomes in patients with suspected TBI who require CPR may not be as uniformly poor as traditionally assumed.
4.4. Strengths and Limitations
This study has several notable strengths. Leveraging data from a large, prospectively collected multicenter registry allowed us to characterize a rare and critically ill population of patients who underwent prehospital CPR for suspected severe TBI. The availability of detailed prehospital information, alongside outcome data, enabled a comprehensive description of patient characteristics, resuscitation patterns, and clinically relevant prognostic signals.
However, several limitations should be considered. First, the cohort definition introduces inherent selection: the results are conditional on resuscitation being attempted and on patients reaching hospital care; therefore, the findings are not directly generalizable to all patients with suspected TBI-related arrest at the scene.
Second, although most core clinical variables (including age, GCS, ISS, airway management, and mortality outcomes) were largely complete, several CPR-specific and prehospital operational variables exhibited substantial proportions of missing data. This was particularly pronounced for cardiac rhythm during resuscitation, for which nearly half of the cohort lacked documented data. As all analyses were restricted to complete cases for the variables under study, selection bias cannot be excluded, especially in subgroup analyses. The high degree of missingness limits the interpretability of rhythm-related findings. Although shockable rhythms were more frequently observed among survivors, this observation should be interpreted with caution. To improve transparency, patients with undocumented initial rhythm were included as a separate descriptive category, revealing intermediate survival compared with shockable and non-shockable rhythms. However, given the extent of missing data and limited subgroup sizes, formal sensitivity analyses were not performed, as these would have been severely underpowered. All rhythm-related findings are therefore presented descriptively and should not be interpreted as evidence of a causal association.
Third, the extremely high 30-day mortality in this cohort limited the discriminative power of statistical modeling, restricting analyses primarily to descriptive and exploratory interpretations. This limitation, combined with heterogeneous arrest etiology and incomplete data, precluded robust comparative or causal inference.
Fourth, important neurological prognostic factors known to influence outcome after severe traumatic brain injury, such as the presence and extent of diffuse axonal injury, were not consistently available in the dataset and could therefore not be included in the analyses. Diffuse axonal injury is recognized as a key determinant of neurological outcome after TBI, but its reliable assessment requires detailed neuroimaging data that were beyond the scope of the present registry-based study [34].
Fifth, neurological outcome was assessed using the Glasgow Outcome Scale at hospital discharge, which represents an early time point after severe traumatic brain injury and may not reliably reflect long-term functional recovery. Patients may substantially improve or deteriorate in the months following discharge. As long-term follow-up data were not consistently available within the BRAIN-PROTECT registry, the proportion of patients classified as having “good recovery” should be interpreted as early neurological status rather than definitive long-term outcome.
Finally, the subgroup of patients achieving good neurological recovery was small. While clinically informative, these observations should be considered hypothesis-generating and interpreted within the broader context of the study’s descriptive design and methodological constraints. In addition, because this study was conducted within a physician-staffed Helicopter Emergency Medical Services system with advanced on-scene capabilities, the observed outcomes may not be directly generalizable to paramedic-led EMS systems with more limited prehospital treatment options.
5. Conclusions
In this study of patients with TBI requiring prehospital CPR, we found that, despite an overall high 30-day mortality rate of approximately 80%, a meaningful proportion (about one in five patients) survived, and roughly half of these survivors achieved moderate to good neurological functional outcomes at hospital discharge. Key favorable signals included early ROSC and the presence of shockable initial rhythms at the scene. These findings suggest that resuscitation efforts may be considered in selected patients with suspected TBI, as outcomes may not be uniformly futile in those who achieve prehospital ROSC, while acknowledging the overall poor prognosis and heterogeneity of this population. Larger prospective studies are needed to better identify which subgroups are most likely to benefit from aggressive resuscitative interventions and to optimize treatment strategies for this vulnerable population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Langlois J.A. Rutland-Brown W. Wald M.M. The epidemiology and impact of traumatic brain injury: A brief overview J. Head Trauma Rehabil.20062137537810.1097/00001199-200609000-0000116983222 · doi ↗ · pubmed ↗
- 2Rubiano A.M. Carney N. Chesnut R. Puyana J.C. Global neurotrauma research challenges and opportunities Nature 2015527 S 193S 19710.1038/nature 1603526580327 · doi ↗ · pubmed ↗
- 3Majdan M. Plancikova D. Brazinova A. Rusnak M. Nieboer D. Feigin V. Maas A. Epidemiology of traumatic brain injuries in Europe: A cross-sectional analysis Lancet Public Health 20161 e 76e 8310.1016/S 2468-2667(16)30017-229253420 · doi ↗ · pubmed ↗
- 4Dewan M.C. Rattani A. Gupta S. Baticulon R.E. Hung Y.C. Punchak M. Agrawal A. Adeleye A.O. Shrime M.G. Rubiano A.M. Estimating the global incidence of traumatic brain injury J. Neurosurg.20191301080109710.3171/2017.10.JNS 1735229701556 · doi ↗ · pubmed ↗
- 5Feigin V.L. Vos T. Nichols E. Owolabi M.O. Carroll W.M. Dichgans M. Deuschl G. Parmar P. Brainin M. Murray C. The global burden of neurological disorders: Translating evidence into policy Lancet Neurol.20201925526510.1016/S 1474-4422(19)30411-931813850 PMC 9945815 · doi ↗ · pubmed ↗
- 6Gravesteijn B.Y. Sewalt C.A. Stocchetti N. Citerio G. Ercole A. Lingsma H.F. von Steinbuchel N. Steyerberg E.W. Wilson L. Maas A.I.R. Prehospital Management of Traumatic Brain Injury across Europe: A CENTER-TBI Study Prehospital Emerg. Care 20212562964310.1080/10903127.2020.181721032877267 · doi ↗ · pubmed ↗
- 7Badjatia N. Carney N. Crocco T.J. Fallat M.E. Hennes H.M. Jagoda A.S. Jernigan S. Letarte P.B. Lerner E.B. Moriarty T.M. Guidelines for prehospital management of traumatic brain injury 2nd edition Prehospital Emerg. Care 200812 S 1S 5210.1080/1090312070173205218203044 · doi ↗ · pubmed ↗
- 8Wiles M.D. Braganza M. Edwards H. Krause E. Jackson J. Tait F. Management of traumatic brain injury in the non-neurosurgical intensive care unit: A narrative review of current evidence Anaesthesia 20237851052010.1111/anae.1589836633447 · doi ↗ · pubmed ↗