Long-Term Response Without Immune-Related Adverse Events to Atezolizumab Treatment in TMB-High Thymoma: A Case Report from the KOSMOS-II Study
In Hee Lee, Moonsik Kim, An Na Seo, Soo Jung Lee, Jee Hyun Kim

TL;DR
A patient with a rare, high TMB thymoma achieved long-term stable disease with atezolizumab and no immune-related side effects.
Contribution
Reports a rare case of TMB-high thymoma responding well to atezolizumab without immune-related adverse events.
Findings
The patient remained progression-free for 14 months after starting atezolizumab treatment.
No significant immune-related adverse events were observed during treatment.
TMB-high status predicted a positive response to immunotherapy in this rare thymoma case.
Abstract
Background: Thymic epithelial tumors (TETs), including thymic carcinomas and thymomas, are rare malignancies originating in the mediastinum. Therapeutic options remain limited for patients experiencing disease progression following platinum-based chemotherapy. High tumor mutational burden (TMB) is uncommon in thymic malignancies but may predict response to immunotherapy. We report a patient with TMB-high TET who participated in the KOSMOS-II study in South Korea and achieved a durable response to atezolizumab without developing immune-related adverse events (irAEs). Case presentation: A 73-year-old woman who had been treated for thymoma 20 years ago presented with a left neck mass. A biopsy of the neck mass confirmed recurrent thymoma, type B3, and her disease progressed despite platinum-based chemotherapy and subsequent pemetrexed treatment. TMB-high thymoma is very rare, but based on…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
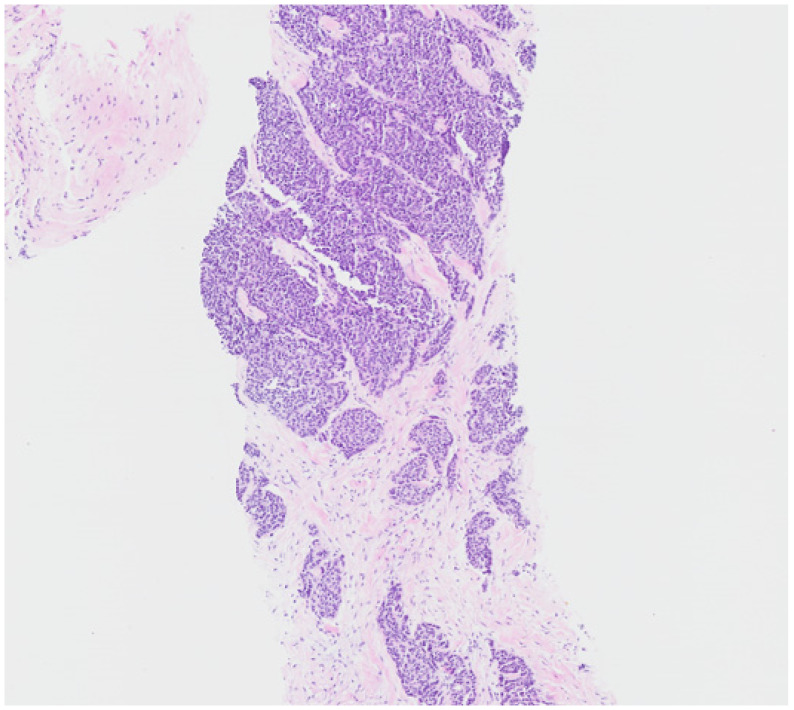 Figure 1
Figure 1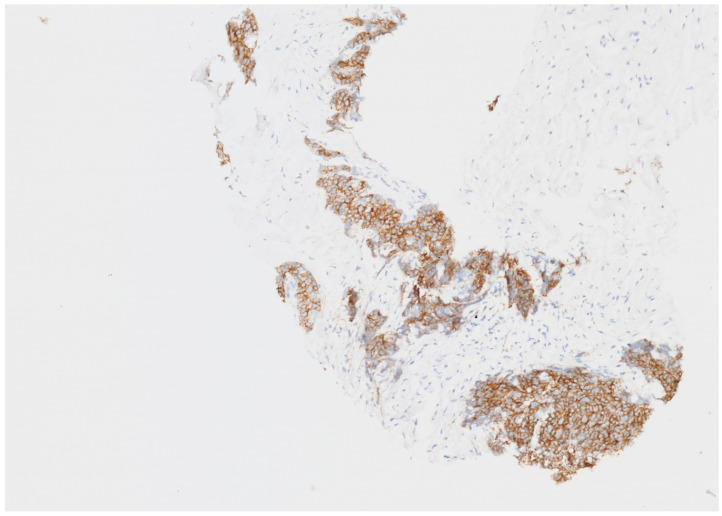 Figure 2
Figure 2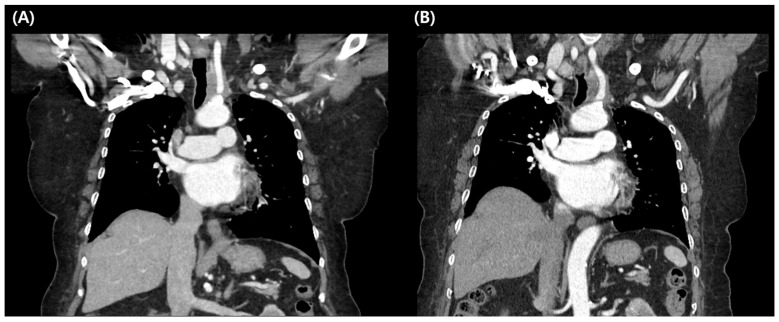 Figure 3
Figure 3- —National R&D Program for Cancer Control, Ministry of Health and Welfare, Republic of Korea
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMyasthenia Gravis and Thymoma · Thyroid Cancer Diagnosis and Treatment · Adrenal Hormones and Disorders
1. Introduction
Thymic epithelial tumors (TETs), which include thymomas and thymic carcinomas, are rare malignancies in adults but represent the most frequent neoplasms of the anterior mediastinum [1]. Their annual incidence is approximately 0.15 per 100,000. Surgical resection remains the only curative treatment for TETs [2]. However, standard treatment is lacking for patients with recurrent disease [3]. Therapeutic options are particularly limited following the failure of platinum-based chemotherapy, with few prospective studies exploring alternative strategies.
The TMB refers to the total number of somatic non-synonymous mutations in a particular region of the tumor genome. A TMB of ≥10 mutations per megabase was reported to predict a better response to ICIs in several cancers [4]. In thymomas, high TMB is uncommon. The Cancer Genome Atlas (TCGA) Project reported that thymic carcinoma shows a high TMB (21.29 mutations per megabase), whereas thymoma has the lowest average TMB (0.48 mutations per megabase) among adult cancers [5]. High TMB is a predictive marker for response to immune checkpoint inhibitors (ICIs), leading to FDA approval of ICIs for tumors with high TMB [6,7]. However, in TETs, treatment with ICIs is associated with a high incidence of immune-related adverse events (irAEs), requiring careful attention.
Here, we report a case of a patient with TMB-high recurrent thymoma who achieved a durable long-term response to atezolizumab without experiencing severe irAEs. Although, the use of ICIs for TMB-high cancers in not approved in Korea, this patient was able to receive atezolizumab treatment by participating in the KOrean Precision Medicine Networking Group Study of MOlecular profiling-guided therapy based on genomic alterations in advanced Solid tumors (KOSMOS)-II trial [8]. Written informed consent was obtained to publish the patient’s clinical details and images.
2. Case
A 73-year-old female patient presented with a left neck mass. Twenty years prior, she had a history of myasthenia gravis, during the investigation of which a thymic mass was discovered and surgically removed. Following thymectomy, she was diagnosed with thymoma and received two cycles of ADOC (doxorubicin, cisplatin, vincristine, and cyclophosphamide) chemotherapy along with radiotherapy. She remained disease-free until the recent presentation with a left neck mass. A core needle biopsy of the left neck mass led to a diagnosis of metastatic thymoma, type B3. Figure 1 shows a representative image of the thymic epithelial tumor. The tumor cells exhibited moderate nuclear atypia with eosinophilic cytoplasm and were found within a fibrotic stroma. PET/CT imaging revealed no distant metastasis. She subsequently underwent six cycles of etoposide and cisplatin (EP) chemotherapy, followed by radiotherapy, achieving a partial response. However, her disease progressed again, and she received eight cycles of pemetrexed. Despite this treatment, the neck mass continued to enlarge, leading to aspiration symptoms during swallowing.
Next-generation sequencing (NGS) testing was performed using biopsy tissue from the neck mass, and a high TMB (20.3 mutations/Mb) was confirmed (Table 1). On DNA sequencing using OncoAccuPanel (hybrid capture-based DNA sequencing using illumina platform), a relatively large number of tier 2 mutations and tier 3 mutations were detected, which suggests a TMB-high type. Estimated TMB was 20.3 muts/Mb. (TMB-high criteria of our institution is more than 20.0 muts/Mb). TMB was calculated as the number of somatic nonsynonymous mutations divided by the targeted coding region (0.65 Mb) and was automatically reported by the OncoAccuPanel analysis pipeline. Although the tumor harbored MLH1 splice site mutation, it was determined to be microsatellite-stable type on the MSI algorithm of OncoAccuPanel and the absence of MLH1 nuclear expression on immunostaining (Figure 2). Despite the fact that the tumor harbored a pathogenic splice donor–site mutation, it showed a relatively low proportion of indel mutations and a predominance of missense mutations, which is not consistent with the typical mutational profile of MSI-high tumors. In addition, the MSI algorithm implemented in the OncoAccuPanel classified the tumor as MSS. We further confirmed MSS status by MSI-PCR (Taken together, these findings led us to hypothesize that the MLH1 mutation represents a single (one-hit) event. Pathogenic mutations in MLH1, TP53, SMAD2, ETV6, and DNMT3A were identified.
High TMB is recognized as a predictive biomarker for response to immunotherapy, and the Food and Drug Administration (FDA) has approved immune checkpoint inhibitors for the treatment of tumors with this characteristic [9]. However, in Korea, immune checkpoint inhibitors are not yet approved for use based on TMB status. This patient was enrolled in the KOSMOS-II study [8], a large-scale nationwide master observational study involving a framework for screening patients with metastatic solid tumors for actionable genetic alterations based on local NGS testing and recommends molecular profiling-guided therapy through a remote and centralized molecular tumor board. Following evaluation by the molecular tumor board (MTB) [10,11], the patient initiated atezolizumab treatment through the therapeutic use of investigational drugs program.
Baseline laboratory tests, including thyroid and adrenal hormone levels, revealed no abnormalities before immunotherapy. The patient commenced her first cycle of atezolizumab and achieved stable disease after three cycles. She has maintained stable disease on atezolizumab and has now completed 20 cycles of treatment and has remained progression-free for 14 months without significant immune-related adverse events (Figure 3). The neck mass in the left perithyroidal region measured 3.3 cm on axial imaging, and after atezolizumab treatment, it decreased to 3.0 cm, consistent with SD.
Regular laboratory tests, including thyroid hormone and ACTH/cortisol levels, were performed, and no significant abnormalities were observed during treatment. Furthermore, during atezolizumab therapy, there was no aspiration or dyspnea, and the patient only complained of mild general weakness. The patient continued maintenance therapy for myasthenia gravis (MG) and regular follow-up with her neurologist throughout the immunotherapy course. She had MGFA class IIA myasthenia gravis and was being treated with pyridostigmine 60 mg four times daily and prednisone 10 mg daily. No exacerbation of MG occurred during treatment, and atezolizumab was well tolerated.
3. Discussion
We report a case of recurrent TMB-high thymoma that remained progression-free for more than 14 months with the ICI, atezolizumab, without experiencing severe irAEs. The significance of this case is that TMB-high thymoma is extremely rare, and although the incidence of irAEs during ICIs is high in TETs with MG, this case demonstrated a long-term response without any notable irAEs.
High TMB is a well-established biomarker predictive of response to immunotherapy, particularly immune checkpoint inhibitors [12]. Multiple studies have demonstrated that tumors with high TMB generate more neoantigens, which enhance T-cell recognition and increase the likelihood of a favorable response to immunotherapy [7]. However, in thymoma, the proportion of high-TMB tumors is extremely low, and the overall TMB level is among the lowest across solid cancers [5,13]. In TCGA data, 117 TETs were classified into four molecular subtypes according to genomic hallmarks and their association with survival and WHO histological subtypes. And when compared with 21 other solid cancers, TETs showed the lowest average TMB, with an average of 0.48 mutations per megabase [5].
Consequently, studies on immunotherapy responses in high-TMB thymoma are rare. In high-TMB thymic carcinoma, a few case reports and small-cohort studies have described clinical responses to immune checkpoint inhibitors. Kaneko et al. demonstrated that a patient with MSI-high thymoma and pleural dissemination achieved a partial response after three cycles of pembrolizumab [14]. In the TAPUR basket trial of pembrolizumab for high-TMB solid tumors, efficacy was analyzed separately for colorectal and non-colorectal cohorts. The non-colorectal cohort, which included one case of TET, showed a disease control rate of 45% (one-sided 90% CI, 35–100) and an objective response rate of 26% [15]. This case is unique in that it represents a very rare TMB-high thymoma, and within the TMB-high TETs, the patient achieved a more favorable response than those reported in the previous studies.
According to previous studies that included patients with histologically confirmed TETs, regardless of biomarkers such as TMB, the response to ICIs ranges from 20 to 30%, with a median PFS of 4–6 months [16,17]. In a phase 2 study of 41 patients by Giaccone et al., an ORR of 22.5% (95% CI 10·8–38·5) and a median PFS of 4·2 months (95% CI 2·9–10·3) were reported [16]. Six (15%) patients developed severe autoimmune toxicity in this study. Cho et al. reported a median PFS of 6.1 months and an ORR of 28.6% in thymoma and 19.2% in thymic carcinoma among 33 patients with platinum-resistant TETs treated with pembrolizumab [17]. In this study, five (71.4%) of seven patients with thymoma developed grade ≥ 3 irAEs, including hepatitis, MG, thyroiditis, colitis, and subacute myoclonus.
Furthermore, the patient in this case had underlying MG, and in contrast to previous reports that ICIs can exacerbate pre-existing MG, this case demonstrates successful ICI treatment without any significant MG exacerbation. Mitsune et al. reported that a patient with pre-existing MG in remission developed a relapse of MG symptoms, polymyositis, and rhabdomyolysis after nivolumab treatment [18]. Cooper et al. described a patient with non–small cell lung cancer (NSCLC) and ocular (MG) in virtual remission who developed severe generalized MG, leading to a myasthenic crisis after anti-PD-1 therapy [19]. Plus, in a cohort study of 65 patients, ICI-related MG (new onset or disease flare) occurred in 63 patients (97%), with a median onset of 4 weeks (range, 1–16 weeks) after treatment initiation [20]. In this study, death was reported in 24 patients (38%), with 15 (23%) due to MG complications. Patients who received intravenous immunoglobulin (IVIG) or plasmapheresis (PLEX) as first-line therapy demonstrated superior outcomes compared with those treated with steroids alone. MG is a life-threatening adverse event with acute onset and rapid progression after ICI treatment. This case demonstrates successful ICI treatment without worsening MG through regular laboratory test and neurological follow-up.
TMB has several limitations as a biomarker for immunotherapy response [10]. A standardized method for measuring TMB is lacking, leading to variability in results across sequencing platforms and mutation-calling pipelines. Universal TMB thresholds do not perform consistently across different tumor types [4], and many patients with low TMB respond to immunotherapy, whereas some with high TMB do not respond [10]. In certain cancers, such as GBM, patients with lower-than- median TMB have shown longer survival after ICB treatment compared to those with higher TMB, suggesting that TMB alone has limitations as a predictive marker for immunotherapy response [8]. ICI treatment is not approved for TMB-high tumors in Korea. However, this patient participated in the KOSMOS-II study, and the NGS results were reviewed by the MTB, which included medical oncologists, pathologists, and a bioinformatics specialist (BI). Based on the MTB’s recommendation, atezolizumab was offered as an appropriate treatment for the TMB-high tumor. The patient remains on immunotherapy with no severe treatment-related adverse events observed to date. However, given the high risk of irAEs, careful risk–benefit assessment and shared decision-making are required.
This case demonstrates a favorable outcome with biomarker-directed ICI treatment in recurrent TET with limited treatment options, highlighting the importance of appropriate markers to predict drug response. Although TMB-based immunotherapy is FDA-approved in the U.S., it remains unavailable in Korea. Its limited availability in Korea underscores the need to explore flexible access pathways, including the potential use of immunotherapy beyond current indications, to improve treatment options for patients with life-threatening conditions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zucali P.A. De Vincenzo F. Perrino M. Digiacomo N. Cordua N. D’Antonio F. Borea F. Santoro A. Systemic treatments for thymic tumors: A narrative review Mediastinum 202152410.21037/med-21-1135118329 PMC 8794302 · doi ↗ · pubmed ↗
- 2Engels E.A. Epidemiology of thymoma and associated malignancies J. Thorac. Oncol.20105 S 260S 26510.1097/JTO.0b 013e 3181 f 1f 62d 20859116 PMC 2951303 · doi ↗ · pubmed ↗
- 3Pavese V. CarfìF.M. Capelletto E. TabbòF. Leo F. Passiglia F. Righi L. Novello S. Merlini A. Bironzo P. Therapeutic management of patients with advanced thymic malignancies: A review for clinicians Lung Cancer 202520410855410.1016/j.lungcan.2025.10855440334289 · doi ↗ · pubmed ↗
- 4Sakane T. Haneda H. Okuda K. Insights into molecular aspects and targeted therapy of thymic carcinoma: A narrative review Mediastinum 202483610.21037/med-23-4838881813 PMC 11176997 · doi ↗ · pubmed ↗
- 5Radovich M. Pickering C.R. Felau I. Ha G. Zhang H. Jo H. Hoadley K.A. Anur P. Zhang J. Mc Lellan M. The Integrated Genomic Landscape of Thymic Epithelial Tumors Cancer Cell 201833244258.e 1010.1016/j.ccell.2018.01.00329438696 PMC 5994906 · doi ↗ · pubmed ↗
- 6Gandara D.R. Agarwal N. Gupta S. Klempner S.J. Andrews M.C. Mahipal A. Subbiah V. Eskander R.N. Carbone D.P. Riess J.W. Tumor mutational burden and survival on immune checkpoint inhibition in >8000 patients across 24 cancer types J. Immunother. Cancer 202513 e 01031110.1136/jitc-2024-01031139915003 PMC 11815411 · doi ↗ · pubmed ↗
- 7Goodman A.M. Kato S. Bazhenova L. Patel S.P. Frampton G.M. Miller V. Stephens P.J. Daniels G.A. Kurzrock R. Tumor Mutational Burden as an Independent Predictor of Response to Immunotherapy in Diverse Cancers Mol. Cancer Ther.2017162598260810.1158/1535-7163.MCT-17-038628835386 PMC 5670009 · doi ↗ · pubmed ↗
- 8Kim S.Y. Kim J.H. Kim T.Y. Park S.R. Yoon S. Lee S. Lee S.H. Kim T.M. Han S.W. Kim H.R. Pragmatic nationwide master observational trial based on genomic alterations in advanced solid tumors: K Orean Precision Medicine Networking Group Study of M Olecular profiling guided therapy based on genomic alterations in advanced Solid tumors (KOSMOS)-II study protocol KCSG AL-22-09BMC Cancer 2024245743872499110.1186/s 12885-024-12338-y PMC 11080169 · doi ↗ · pubmed ↗