A Clinically Applicable Nomogram for Live Birth Prediction After IVF: The Zubeyde Hanim Model
Pınar Karaçin, Runa Özelçi, Enes Kumcu, Dilek Kaya Kaplanoğlu, Serdar Dilbaz, Yaprak Üstün

TL;DR
This study created a tool to predict the chance of live birth after IVF using common clinical data, which can help doctors guide patients better.
Contribution
The development of a new nomogram called the Zubeyde Hanim IVF Nomogram for predicting live birth outcomes after IVF.
Findings
Female age, embryo quality, day of embryo transfer, and endometrial thickness were identified as independent predictors of live birth.
The nomogram achieved a bootstrap-corrected AUC of 0.64, showing acceptable discrimination and calibration.
The model uses routinely available clinical parameters to estimate individualized live birth probabilities.
Abstract
Objective: In this study, we aimed to develop and internally validate a clinically applicable nomogram for predicting live birth following in vitro fertilization (IVF) using routinely available clinical and embryological parameters. Methods: This retrospective study was conducted at a single tertiary IVF center. Women undergoing IVF/ICSI were included if their baseline demographic and clinical data were available, they had undergone at least one fresh or frozen–thawed embryo transfer, and they had a known live birth outcome. Women with cycles without embryo transfer and those missing key outcome data were excluded from the analysis. As a result, a total of 2119 IVF/ICSI treatment cycles resulting in embryo transfer were included in the analysis. To identify independent predictors of live birth, multivariable logistic regression analysis was performed. Results: Among the 2119 treatment…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1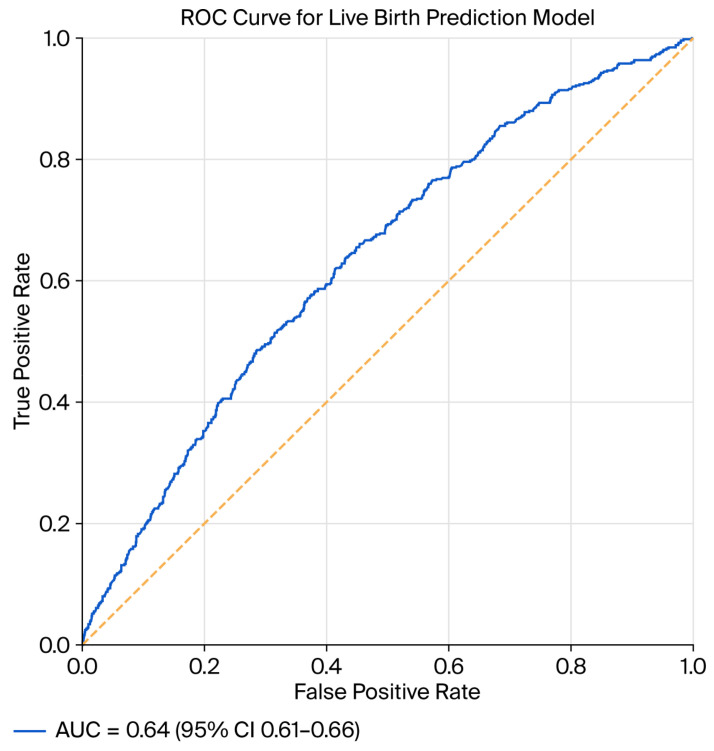 Figure 2
Figure 2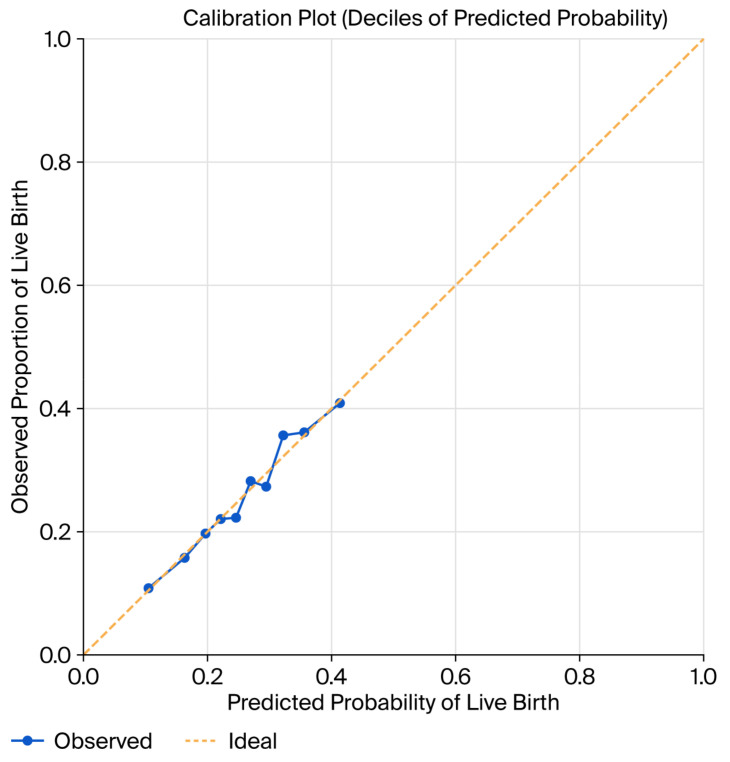 Figure 3
Figure 3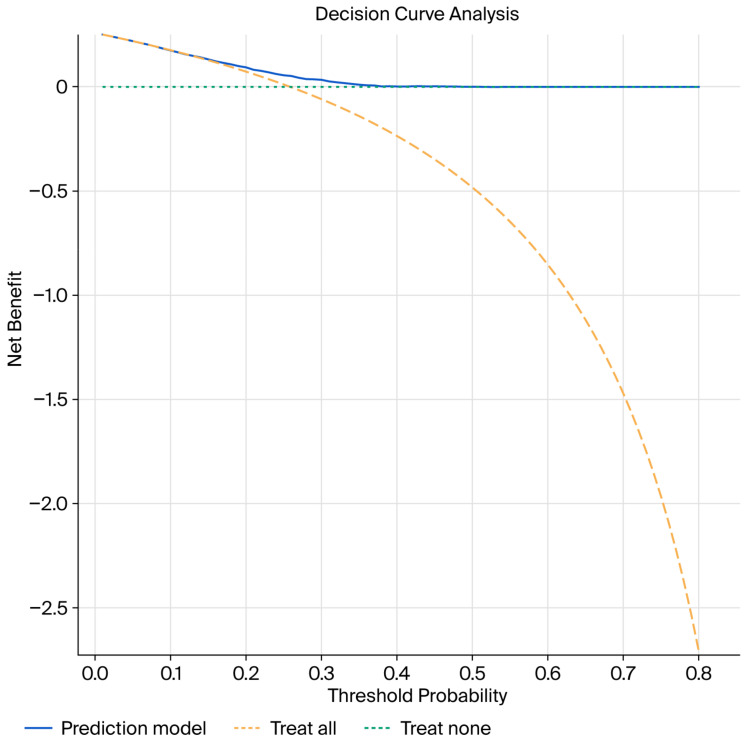 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOvarian function and disorders · Reproductive Health and Technologies · Reproductive Biology and Fertility
1. Introduction
Assisted reproductive technologies (ARTs) have evolved substantially in recent decades, resulting in improved pregnancy outcomes and expanding access to infertility treatment worldwide [1]. Nevertheless, despite the technological progress that has been made in ovarian stimulation, laboratory conditions, and embryo culture, the likelihood of achieving a live birth following in vitro fertilization–embryo transfer (IVF-ET) remains highly heterogeneous among patients and treatment cycles [1]. From both a clinical and patient-centered perspective, live birth represents the most relevant and definitive outcome of IVF, surpassing intermediate endpoints such as biochemical or clinical pregnancy [2]. Consequently, identifying reliable predictors of live birth and integrating them into clinically applicable prediction models has become a priority in contemporary reproductive medicine.
IVF success is determined by a complex interaction of maternal, paternal, embryological, and treatment-related factors [3]. Female age remains the strongest and most consistently reported predictor of live birth, reflecting age-dependent declines in oocyte competence and increasing rates of chromosomal abnormalities [3,4]. However, chronological age alone provides an incomplete assessment of reproductive potential. Ovarian reserve markers, particularly anti-Müllerian hormone (AMH) and antral follicle count (AFC), are widely used to estimate quantitative ovarian response, yet their independent ability to predict live birth is limited and context-dependent [5].
Beyond ovarian reserve, embryological parameters—including embryo morphology, blastocyst development, and stage of embryo transfer—have demonstrated associations with implantation and live birth outcomes [6,7]. However, these parameters are influenced by inter-observer variability, laboratory-specific grading systems, and center-dependent practices, which restrict their universal applicability as standalone predictors [8]. Similarly, treatment-related factors such as stimulation protocols, gonadotropin dose, and endometrial preparation strategies contribute to outcome variability but rarely offer consistent predictive power when evaluated in isolation [9].
In routine clinical practice, counseling regarding IVF success often relies on single predictors or clinician experience rather than integrated, quantitative risk assessment. This approach may lead to inaccurate prognostication, unrealistic patient expectations, and suboptimal individualization of treatment strategies. With the growing availability of large IVF databases, there is increasing interest in multivariable prediction models that better reflect the multifactorial nature of live birth outcomes [10,11].
Several prognostic models and scoring systems for IVF outcomes have been proposed over the past decade. While some have demonstrated moderate discrimination, many are limited by their small sample sizes, restricted patient populations, or reliance on early-cycle outcomes such as oocyte yield or clinical pregnancy rather than live birth [12,13]. Importantly, predictors of ovarian response or implantation do not necessarily translate into predictors of live birth, as pregnancy loss and obstetric factors introduce additional biological complexity [14]. As a result, outcome-specific modeling focused explicitly on live birth has gained increasing attention.
Another methodological challenge in IVF research is the presence of repeated treatment cycles within the same patient. Many individuals undergo multiple IVF attempts, leading to non-independence of observations that can bias traditional regression analyses if not adequately addressed [10]. Predictive models that incorporate real-world treatment trajectories and repeated cycles are therefore more likely to generate clinically meaningful and generalizable estimates.
Developing prediction models based on large, single-center cohorts offers distinct advantages. Standardized clinical protocols, consistent laboratory conditions, and uniform outcome definitions reduce heterogeneity and strengthen internal validity [15]. At the same time, the inclusion of consecutive treatment cycles over an extended period allows for the evaluation of fresh and frozen embryo transfers, diverse stimulation strategies, and cumulative clinical experience, thereby improving real-world applicability.
This study aimed to develop and internally validate a multivariable predictive model for live birth following IVF-ET using data from approximately 2000 treatment cycles performed at a tertiary reproductive medicine center. By integrating readily available demographic, clinical, and laboratory parameters, we sought to construct a clinically applicable prediction tool reflective of routine practice. Such a model may enhance individualized patient counseling, support evidence-based decision-making, and contribute to personalized treatment planning in modern IVF care.
2. Methods
2.1. Study Design and Population
This single-center retrospective cohort study was conducted at a tertiary IVF center. All consecutive IVF/ICSI cycles performed between 2007 and 2023 were screened for eligibility. Cycles resulting in embryo transfer and with complete follow-up data for live birth outcome were included.
A total of 2119 treatment cycles were eligible for analysis. The primary outcome was live birth, defined as the delivery of at least one live-born infant beyond 24 weeks of gestation. Each cycle was treated as an independent observation. In patients undergoing more than one treatment cycle, each cycle was analyzed separately, consistent with previously published IVF prediction models.
Model development and reporting followed the TRIPOD guidelines.
2.2. Inclusion and Exclusion Criteria
2.2.1. Inclusion Criteria
Women undergoing IVF/ICSI were included in this study if they had the following:
- ○Available baseline demographic and clinical data;
- ○At least one embryo transfer (fresh or frozen–thawed);
- ○Known live birth outcome.
2.2.2. Exclusion Criteria
The exclusion criteria comprised the following:
- Cycles without embryo transfer;
- Cycles with missing key outcome data (live birth status);
- Cycles involving experimental stimulation or laboratory protocols;
- Cycles using donor oocytes or donor sperm.
2.3. Clinical and Laboratory Data Collection
The variables that were extracted from the institutional electronic medical records and IVF laboratory database are detailed in the following subsections.
2.3.1. Demographic and Baseline Characteristics
Female age (years), body mass index (BMI, kg/m^2^), and duration of infertility (months) were recorded as baseline demographic variables. Infertility type was classified as primary infertility, defined as the absence of any prior clinical pregnancy, or secondary infertility, defined as a history of at least one previous clinical pregnancy, regardless of outcome.
2.3.2. Infertility Diagnosis
Infertility etiology was classified into male factor infertility, tubal factor infertility, ovulatory or hormonal disorders, polycystic ovary syndrome (PCOS), and unexplained infertility.
2.3.3. Baseline Hormonal Assessment
Baseline hormonal assessment included basal day 3 serum follicle-stimulating hormone (FSH) and estradiol (E2) levels. All hormone measurements were performed using standardized immunoassay techniques in the same institutional laboratory.
2.4. Controlled Ovarian Stimulation and Laboratory Procedures
Controlled ovarian stimulation was conducted using either a GnRH agonist long protocol or a GnRH antagonist protocol, selected according to clinician preference and individual patient characteristics. Oocyte retrieval was performed 34–36 h after ovulation was triggered. Fertilization was achieved predominantly through intracytoplasmic sperm injection (ICSI), in accordance with the routine laboratory practice of the center.
2.5. Embryo Culture and Transfer
Embryos were cultured under standard laboratory conditions and transferred either on day 3 at the cleavage stage or on day 5 at the blastocyst stage. Both fresh and frozen–thawed embryo transfer cycles were included in the analysis. Endometrial thickness was measured using transvaginal ultrasonography on the day of embryo transfer.
Embryo Quality Assessment
Embryo morphology was assessed according to routine laboratory grading systems, in line with the principles of the 2011 Istanbul consensus on embryo assessment [8]. For analytical purposes, embryos were categorized as high-quality (Grade 1 or Grade 2) or low-quality (Grade 3 or Grade 4). The variable “high-quality embryo transfer” was defined as a binary variable (yes/no) indicating whether at least one high-quality embryo was transferred in the cycle based on standardized embryo grading criteria. In cycles where multiple embryos were transferred, embryo quality classification was based on the presence of at least one high-quality embryo.
2.6. Outcome Measure
The primary outcome was live birth, defined as the birth of a living neonate after ≥24 weeks of gestation.
During the preparation of this manuscript, support was received from artificial intelligence-based tools, including Jenni AI (Altum Inc., Wilmington, DE, USA) and ChatGPT-5 (OpenAI, San Francisco, CA, USA), solely to improve the quality and clarity of the English language and overall manuscript structure. No data analysis, statistical modeling, or interpretation of the results was performed using artificial intelligence. All scientific content and data are original. The authors critically reviewed, verified, and edited all AI-assisted outputs and take full responsibility for the accuracy, integrity, and content of this publication.
2.7. Statistical Analysis
Continuous variables were expressed as mean ± standard deviation or median (interquartile range), as appropriate. Categorical variables were presented as counts and percentages. To identify independent predictors of live birth, multivariable logistic regression analysis was performed. Variables considered clinically relevant and supported by the prior literature were entered into the initial model. A backward stepwise elimination approach based on the likelihood ratio test was applied to derive the final prediction model. Variables were retained in the model if they remained statistically significant or demonstrated stable clinical relevance. Candidate variables were selected a priori based on clinical relevance and the previous literature. Multicollinearity among candidate predictors was assessed prior to model fitting, and no significant collinearity was detected. A backward stepwise logistic regression approach was subsequently used to derive a parsimonious prediction model. Variables reflecting clinical treatment decisions, such as the number of embryos transferred, were not included as candidate predictors to avoid confounding by indication and to preserve model interpretability. Model discrimination was assessed using the area under the receiver operating characteristic (ROC) curve (AUC).
Internal validation was performed using bootstrap resampling with 500 iterations to estimate optimism-corrected model performance.
Model calibration was evaluated using the following:
- Calibration plots based on deciles of predicted risk;
- Comparison of observed versus predicted live birth probabilities.
Clinical utility was assessed using decision curve analysis, estimating net benefit across a range of threshold probabilities.
To address potential within-patient correlation due to repeated cycles, sensitivity analyses restricted to the first embryo transfer cycle per woman were performed. In addition, clustered marginal models using generalized estimating equations with the patient identifier as the clustering variable were fitted. To assess the robustness of the model assumptions, several sensitivity analyses were performed. These included restriction of the analysis to the first embryo transfer cycle per woman, fitting clustered marginal models using generalized estimating equations to account for within-patient correlation, and stratification by embryo transfer type (fresh versus frozen).
Based on the final multivariable model, a graphical nomogram was constructed to provide individualized predictions of live birth probability.
All statistical analyses were performed using Statistical Package for the Social Sciences (SPSS), version 25.0 (IBM Corp., Armonk, NY, USA), and supplementary analyses, including bootstrap resampling, ROC curve analyses, and figure generation, were performed using R statistical software (version 4.0.2; R Foundation for Statistical Computing, Vienna, Austria). A two-sided p-value < 0.05 was considered statistically significant.
3. Results
A total of 2119 embryo transfer cycles were included in the analysis, of which 541 (25.5%) resulted in live birth. The baseline demographic and clinical characteristics according to live birth outcome are summarized in Table 1. Women who achieved live birth were significantly younger than those who did not (29 ± 4.8 vs. 31 ± 5.6 years, p < 0.001) and had a shorter duration of infertility (55 ± 43.2 vs. 61 ± 50.4 months, p = 0.012). Antral follicle count was also higher in the live birth group (14 ± 8.1 vs. 13 ± 8.1, p = 0.012). No significant differences were observed between groups with respect to body mass index, male age, infertility type (primary vs. secondary), gravidity, previous live birth history, basal gonadotropin levels (FSH and LH), or basal estradiol concentrations. The distribution of infertility diagnoses was largely comparable between groups, although male factor infertility tended to be more frequent among cycles resulting in live birth (43.3% vs. 38.5%, p = 0.050).
Stimulation and laboratory characteristics are presented in Table 2. The use of GnRH agonist and antagonist protocols was similar between cycles with and without live birth (p = 0.372). Total gonadotropin dose and stimulation duration did not differ significantly between groups, with a mean stimulation length of approximately 10 days in both cohorts. Trigger-day estradiol and progesterone levels were comparable, and mean progesterone concentrations remained below clinically relevant thresholds for premature luteinization. While the total number of retrieved and mature oocytes did not differ significantly, the number of normally fertilized oocytes (2PN) was significantly higher in cycles resulting in live birth (5.4 ± 3.4 vs. 4.8 ± 3.6, p = 0.001).
Table 3 summarizes the baseline differences between fresh and frozen embryo transfer cycles and provides the rationale for the performance of additional sensitivity analyses. Endometrial thickness on the day of transfer was similar between fresh and frozen cycles. A significant difference in the day of embryo transfer was observed, with cleavage-stage (day 3) transfers being more frequent in fresh cycles, whereas blastocyst transfers predominated in frozen cycles (p < 0.001). The number of embryos transferred also differed significantly between groups, with single-embryo transfer being more common in fresh cycles and multiple-embryo transfer occurring more frequently in frozen cycles (p < 0.001). High-quality embryos were transferred at a higher rate in frozen embryo transfer cycles compared with fresh transfers (92.1% vs. 86.4%, p = 0.001).
Baseline demographic, clinical, and treatment-related characteristics of the study population were entered into the multivariable analysis as candidate predictors of live birth.
3.1. Multivariable Logistic Regression Analysis Results
Using a backward stepwise logistic regression approach, independent predictors of live birth were identified. The final model retained four variables as statistically significant predictors: female age, high-quality embryo transfer, day of embryo transfer (day 5 vs. day 3), and endometrial thickness on the day of transfer.
The results of the multivariable logistic regression analysis evaluating independent predictors of live birth are presented in Table 4. Female age was independently and inversely associated with live birth, with each additional year of age associated with a reduced likelihood of live birth (odds ratio [ORs] 0.959; 95% confidence interval [CI] 0.940–0.978; p < 0.001). The transfer of a high-quality embryo was a strong positive predictor of live birth compared with low-quality embryos (OR 2.752, 95% CI 1.857–4.077; p < 0.001). Blastocyst-stage transfer (day 5) was also independently associated with higher odds of live birth compared with cleavage-stage transfer (day 3) (OR 1.427, 95% CI 1.161–1.754; p = 0.001). In addition, greater endometrial thickness on the day of embryo transfer was associated with a modest but statistically significant increase in live birth probability (OR 1.086 per mm, 95% CI 1.042–1.132; p <0.001).
Other candidate variables—including body mass index, infertility type (primary vs. secondary), basal follicle-stimulating hormone levels, infertility diagnosis (including ovulatory disorders, unexplained infertility, and polycystic ovary syndrome), male factor infertility, number of normally fertilized oocytes (2PN), transfer type (fresh vs. frozen), and prior live birth history—were not retained in the final multivariable model during the backward elimination process due to the lack of independent predictive value.
3.2. Nomogram Development
Based on the final multivariable logistic regression model, a clinically applicable nomogram was constructed to estimate the individualized probability of live birth (Figure 1). Each predictor was assigned a weighted point value proportional to its regression coefficient, with total points corresponding to the predicted live birth probability.
3.3. Model Discrimination
The discriminative performance of the model was evaluated using the area under the receiver operating characteristic curve (AUC). The model demonstrated acceptable discrimination, with an apparent AUC of approximately 0.64 (95%CI: 0.61–0.66). After internal validation using 500 bootstrap resamples, the optimism-corrected AUC remained stable, indicating minimal overfitting (Figure 2).
3.4. Model Calibration
Calibration of the model was assessed using calibration plots based on deciles of predicted risk. The calibration curve demonstrated good agreement between predicted and observed live birth probabilities across the entire range of risk, with only minor deviation at extreme probability values (Figure 3). This finding suggests that the model provides reliable absolute risk estimates.
3.5. Decision Curve Analysis
Decision curve analysis was performed to evaluate the clinical utility of the nomogram. The model demonstrated a net clinical benefit across a wide range of threshold probabilities compared with both “treat-all” and “treat-none” strategies (Figure 4), supporting its potential usefulness in individualized clinical decision-making.
3.6. Sensitivity Analyses
Supplementary Tables S1–S3 present the results of the sensitivity analyses, including those restricted to first cycles, clustered models, and stratification by transfer type. Specifically, Table S1 shows the results for the sensitivity analysis restricted to the first IVF cycle per woman. This analysis was performed to address potential within-patient correlation due to repeated cycles. The AUC was 0.63, 95% CI: 0.61–0.67; thus, even when limited to first cycles, the results did not change (Table S1). Model discrimination was comparable between fresh and frozen embryo transfer cycles. Stratified analyses by transfer type are presented in Supplementary Table S3.
3.7. Internal Validation
Internal validation using bootstrap resampling (500 iterations) confirmed the robustness of the model. Regression coefficients, AUC values, and calibration parameters showed minimal optimism, indicating that the model maintains predictive accuracy when applied to new samples drawn from the same population. Details of the bootstrap internal validation, including apparent and optimism-corrected AUC estimates, are provided in Supplementary Table S4. The apparent AUC was 0.64, 95% CI (bootstrap percentile: 0.61–0.66), and the optimism-corrected AUC was 0.63.
4. Discussion
In this large, single-center cohort study including 2119 IVF treatment cycles, we developed and internally validated a nomogram to predict live birth based on routinely available clinical and embryological parameters. Using a backward stepwise logistic regression approach with bootstrap validation, four variables emerged as independent predictors of live birth: female age, embryo quality, day of embryo transfer, and endometrial thickness on the day of transfer. The final model demonstrated acceptable discrimination, with a bootstrap-corrected AUC of approximately 0.64, which is comparable to previously published IVF prediction models.
Female age remained a strong and independent negative predictor of live birth in our model. This finding is entirely consistent with the established literature and reflects the well-documented age-related decline in oocyte competence, embryo developmental potential, and endometrial receptivity [16,17]. Numerous IVF prediction models and nomogram studies have consistently identified female age as one of the most influential determinants of live birth, often with effect sizes comparable to or exceeding those observed in our cohort [10,18]. Importantly, the persistence of female age as a significant predictor even after adjustment for embryo-related variables underscores its overarching biological impact, which cannot be fully mitigated by laboratory advances alone.
Embryo quality emerged as the strongest positive predictor of live birth, with cycles involving the transfer of at least one high-quality embryo demonstrating an approximate threefold increase in live birth probability. This result aligns closely with previous studies showing that morphological embryo grading remains a robust proxy for implantation and live birth potential, despite increasing interest in adjunctive technologies such as time-lapse imaging and preimplantation genetic testing [8,19]. Several prior nomogram-based prediction models have similarly identified embryo quality as a central determinant of treatment success [12,20]. Our findings reinforce the continued relevance of conventional morphology-based embryo assessment in real-world clinical practice, particularly in settings where advanced selection techniques are not universally applied.
Day 5 embryo transfer was independently associated with higher odds of live birth compared with day 3 transfer. This observation is consistent with both randomized trials and large observational studies suggesting superior implantation and live birth rates with blastocyst-stage transfer, largely due to improved embryo self-selection and enhanced synchrony with endometrial receptivity [21,22]. Several previously published IVF prediction models have incorporated transfer day as a key predictive variable and achieved results similar to ours [13,18]. Nevertheless, it is important to acknowledge that blastocyst transfer is often reserved for cycles with favorable embryological development, which may partly explain its strong association with live birth.
Endometrial thickness on the day of embryo transfer demonstrated a modest but statistically significant association with live birth. Although the clinical relevance of endometrial thickness has been debated, multiple meta-analyses and large cohort studies support the existence of a positive relationship between increasing endometrial thickness and pregnancy outcomes, particularly at lower thickness thresholds [23,24]. Our findings are in line with previous nomogram studies that retained endometrial thickness as an independent predictor, suggesting that it provides additive prognostic information beyond embryo-related factors [12,20]. Endometrial thickness remained an independent predictor of live birth and contributed meaningfully to overall model performance; however, its clinical interpretation should be considered within the context of other key predictors rather than as a standalone determinant.
Compared with earlier IVF prediction models, our nomogram offers several strengths. It focuses on live birth rather than clinical pregnancy, incorporates both fresh and frozen embryo transfer cycles, and relies exclusively on widely available clinical parameters, enhancing its applicability in routine practice. The observed AUC of 0.64 is comparable with those reported in many previously published IVF nomograms, which typically range between 0.65 and 0.75 [10,18].
The major strengths of this study include the large sample size, cycle-based analysis, focus on live birth as the primary outcome, and rigorous internal validation using bootstrap resampling. Additionally, the use of routinely collected variables enhances the generalizability and ease of implementation of the proposed nomogram. However, this study was conducted in a single tertiary referral center with highly standardized stimulation, laboratory, and embryo transfer protocols. Practices such as the high utilization of intracytoplasmic sperm injection (ICSI) and the use of a specific embryo grading system may differ across centers and could limit the direct generalizability of the model. Therefore, the performance of the proposed nomogram may vary in settings with different laboratory techniques or clinical practices. Given the single-center retrospective design, external validation in independent, preferably multi-center cohorts is mandatory before routine clinical application of this prediction model.
This study has several limitations that should be acknowledged. First, the retrospective and single-center design may limit external generalizability, and external validation in independent cohorts is warranted. Second, each cycle was treated as an independent observation, which may introduce within-patient correlation in women undergoing multiple cycles. Third, detailed embryo genetic data and advanced embryo selection tools were not available and therefore not included in the model. Anti-Müllerian hormone (AMH), an important marker of ovarian reserve, could not be included in the prediction model because AMH measurements were available for only a limited proportion of women in the cohort, which would have resulted in a substantial loss of sample size and potential selection bias. Detailed male factor parameters were not included to maintain model simplicity and applicability across different clinical settings. Dichotomizing embryo quality improved model simplicity and clinical interpretability but may have resulted in the loss of more granular prognostic information, such as the number or relative quality of transferred embryos. Given the long inclusion period, changes in laboratory techniques, stimulation strategies, and embryo culture practices over time cannot be excluded and may have influenced the outcomes. Finally, although internal validation was robust, prospective validation is required before widespread clinical adoption of this model. Although multiple cycles from some women were included, sensitivity analyses accounting for within-patient correlation yielded consistent results, supporting the robustness of the model.
5. Conclusions
In conclusion, we developed and internally validated a clinically practical nomogram for predicting live birth following IVF treatment. Female age, embryo quality, transfer day, and endometrial thickness were identified as key independent predictors. This model may serve as a useful tool for individualized patient counseling and treatment planning, pending external validation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adamson G.D. de Mouzon J. Chambers G.M. Zegers-Hochschild F. Mansour R. Ishihara O. Banker M. Dyer S. International Committee for Monitoring Assisted Reproductive Technology: World report on assisted reproductive technology, 2011 Fertil. Steril.20181101067108010.1016/j.fertnstert.2018.06.03930396551 · doi ↗ · pubmed ↗
- 2Zegers-Hochschild F. Adamson G.D. Dyer S. Racowsky C. De Mouzon J. Sokol R. Rienzi L. Sunde A. Schmidt L. Cooke I.D. The international glossary on infertility and fertility care, 2017 Hum. Reprod.2017321786180110.1093/humrep/dex 23429117321 PMC 5850297 · doi ↗ · pubmed ↗
- 3Nelson S.M. Telfer E.E. Anderson R.A. The ageing ovary and uterus: New biological insights Hum. Reprod. Update 201319678310.1093/humupd/dms 04323103636 PMC 3508627 · doi ↗ · pubmed ↗
- 4Zhu H. Zhao C. Xiao P. Zhang S. Predicting the likelihood of live birth in assisted reproductive technology according to the number of oocytes retrieved and female age using a generalized additive model: A retrospective cohort analysis of 17,948 cycles Front. Endocrinol.20211260623110.3389/fendo.2021.60623133995268 PMC 8120808 · doi ↗ · pubmed ↗
- 5Harris B.S. Jukic A.M. Truong T. Nagle C.T. Erkanli A. Steiner A.Z. Markers of ovarian reserve as predictors of future fertility Fertil. Steril.20231199910610.1016/j.fertnstert.2022.10.01436460524 PMC 10074834 · doi ↗ · pubmed ↗
- 6Awadalla M.S. Ho J.R. Mc Ginnis L.K. Ahmady A. Cortessis V.K. Paulson R.J. Embryo morphology and live birth in the United States FS Rep.2022313113710.1016/j.xfre.2022.02.006PMC 925011635789729 · doi ↗ · pubmed ↗
- 7Li N. Guan Y. Ren B. Zhang Y. Du Y. Kong H. Zhang Y. Lou H. Effect of blastocyst morphology and developmental rate on euploidy and live birth rates in preimplantation genetic testing for aneuploidy cycles with single-embryo transfer Front. Endocrinol.20221385804210.3389/fendo.2022.858042 PMC 904403335498424 · doi ↗ · pubmed ↗
- 8Alpha Scientists in Reproductive Medicine and ESHRE Special Interest Group of Embryology. The Istanbul consensus workshop on embryo assessment: Proceedings of an expert meeting Hum. Reprod.2011261270128310.1093/humrep/der 03721502182 · doi ↗ · pubmed ↗