Longitudinal Observation by Optical Coherence Tomography in Patients Treated with Ethambutol: A Systematic Review and Meta-Analysis
Rui Luo, Jin Ma, Yong Zhong

TL;DR
This study finds that ethambutol treatment does not generally cause retinal nerve fiber layer thinning in mycobacterial infection patients, though some subgroups like males show significant changes.
Contribution
The study provides a meta-analysis of OCT measurements to clarify ethambutol's effects on retinal layers in patients without optic neuropathy.
Findings
Ethambutol does not cause significant retinal nerve fiber layer (RNFL) thinning overall in patients without EON.
Male-dominant studies and those in Turkey and India show significant RNFL thickness decreases.
Only two studies reported GCIPL thickness changes, with significant decreases in male-dominant studies.
Abstract
Background: The retinal changes caused by ethambutol are not clear in patients with the administration of ethambutol and without ethambutol-induced optic neuropathy (EON). The aim of this systematic review is to estimate the changes in retinal nerve fiber layer (RNFL) and ganglion cell layer and inner plexiform layer (GCIPL) thicknesses measured by optical coherence tomography (OCT) in patients with mycobacterial infection treated with ethambutol and not suffering from EON. Methods: A systematic review of articles was conducted by searching PubMed, Embase, and Web of Science until November 2025. Additional studies were identified by the review of references. Search terms included OCT and ethambutol. Longitudinal observational studies using an OCT device to measure RNFL and GCIPL thicknesses before and after the administration of ethambutol in patients with mycobacterial infection…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
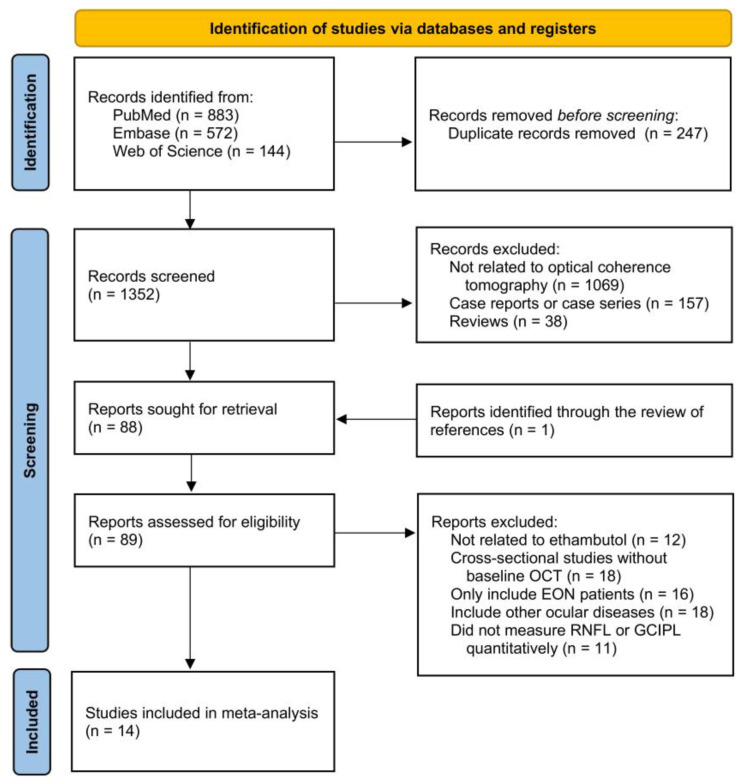 Figure 1
Figure 1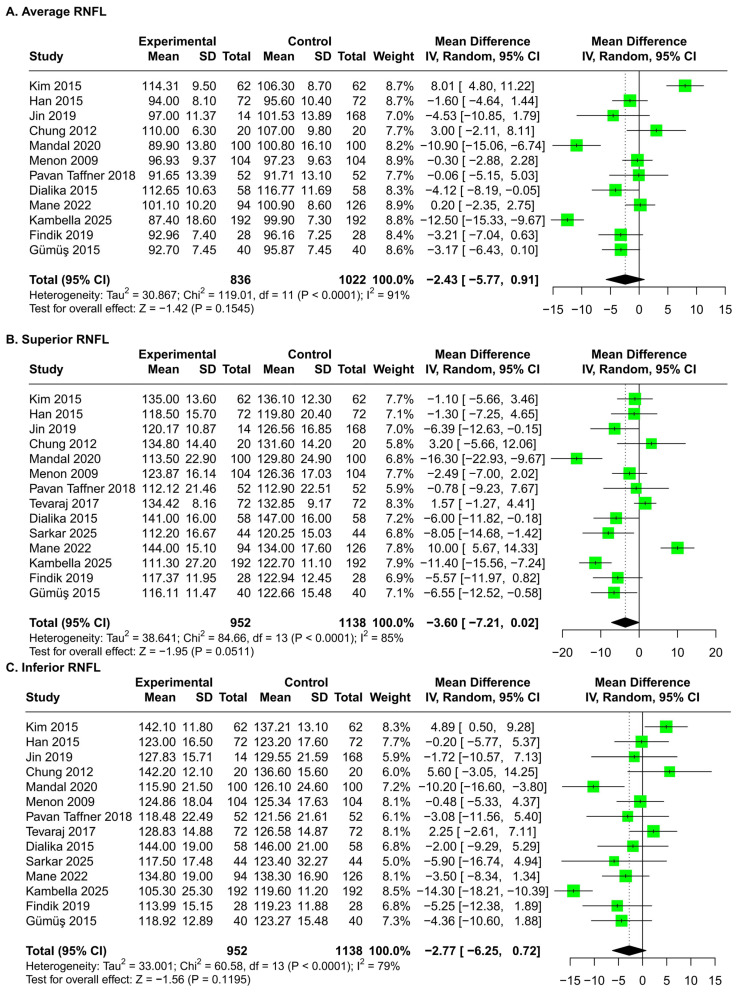 Figure 2
Figure 2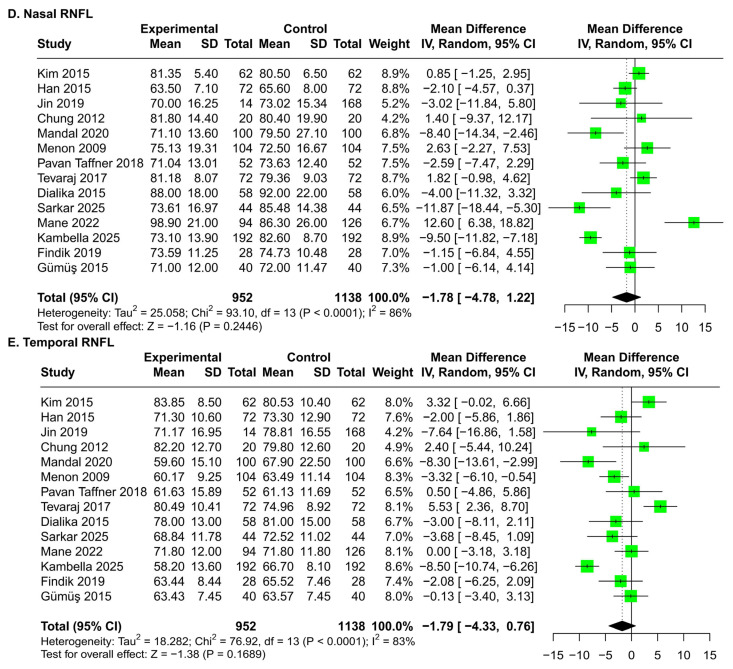 Figure 3
Figure 3 Figure 4
Figure 4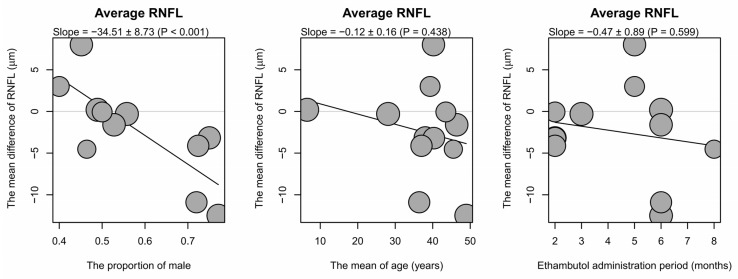 Figure 5
Figure 5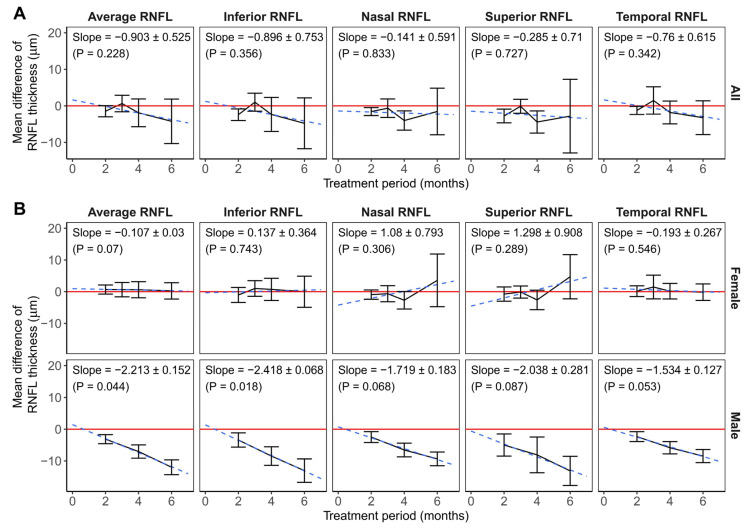 Figure 6
Figure 6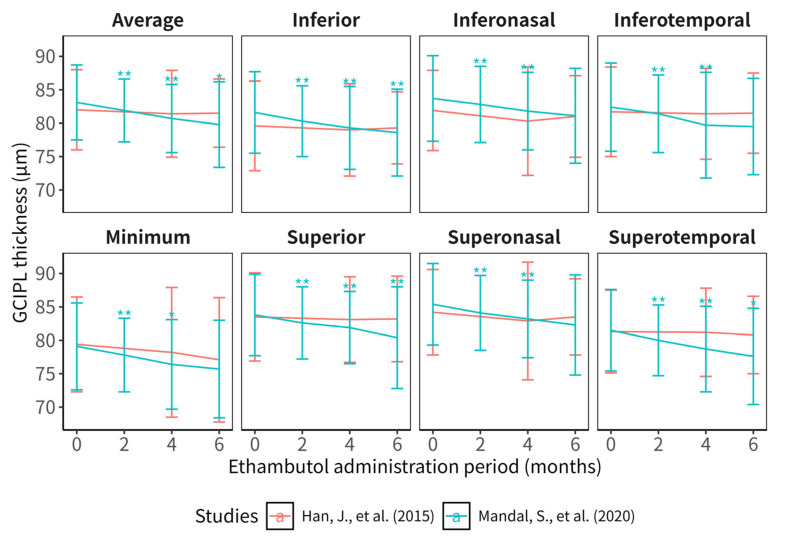 Figure 7
Figure 7- —National High Level Hospital Clinical Research Funding
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDrug-Induced Ocular Toxicity · Infectious Encephalopathies and Encephalitis · Hallucinations in medical conditions
1. Introduction
Ethambutol is an effective antibiotic broadly used in the treatment of mycobacterial infection, especially tuberculosis. However, toxic optic neuropathy is one of the most common severe adverse effects caused by this drug. The reported incidence of ethambutol-induced optic neuropathy (EON) varies from 0.25% to 6.5% in different retrospective observational studies [1,2,3,4,5,6]. Patients with EON present with decreased visual acuity, abnormal color vision, optic disc pallor, and visual field defects [7], which usually show bilateral involvement and are dose- and duration-dependent [4,6].
Since there is no effective treatment for EON [8], the prognosis of EON is poor. A retrospective study conducted by Valenchia and colleagues [9] showed that visual improvement was observed in only 56.9% of patients with EON despite cessation of ethambutol, and the proportion was lower in old patients and patients with hypertension or kidney diseases. The visual outcome is worse in patients with a delay of more than a month from symptom onset and the drug cessation [10]. On the contrary, subclinical ocular lesions caused by ethambutol are reversible after the discontinuation of the drug [11]. Therefore, a thorough understanding of subclinical changes related to ethambutol may help improve the screening strategy and reduce the burden of EON.
The changes in several functional indicators in patients treated with ethambutol have been studied in previous research. Changes in visual evoked potentials and multifocal electroretinography were observed in patients with the administration of ethambutol and without EON; however, changes in visual acuity, color vision, contrast sensitivity, and visual field were not significant [8,11,12]. Although electrophysiological indicators may be able to detect EON early, these examinations are time-consuming and not appropriate for screening subclinical EON.
Optical coherence tomography (OCT) is a noninvasive and noncontactable device and can detect retinal lesions quantitatively; thus, it is broadly used in the evaluation of many ocular diseases, such as glaucoma [13], uveitis [14], retinopathy [15], and optic neuritis [16]. Ocular lesions related to ethambutol were also detected by OCT in previous studies, which reported decreased thicknesses in both retinal nerve fiber layer (RNFL) and ganglion cell layer and inner plexiform layer (GCIPL) in patients with EON [17,18,19]. In addition, Lee and colleagues [20] found a good diagnostic performance of GCIPL thicknesses in the diagnosis of EON, and Kang and colleagues [21] reported the prognostic value of RNFL and GCIPL in the visual function of EON patients. However, the results of the OCT changes are controversial in patients treated with ethambutol and not suffering from EON, leading to difficulties in the evaluation of subclinical toxicity related to ethambutol.
Therefore, in the present meta-analysis, we aimed to compare the changes in RNFL and GCIPL thicknesses detected by OCT before and after the administration of ethambutol in patients with mycobacterial infection.
2. Materials and Methods
This systematic review and meta-analysis were conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses COnsensus-based Standards for the selection of health Measurement INstruments (PRISMA-COSMIN) for outcome measurement instruments (OMIs) 2024 (checklist shown in Table S1) [22] and registered at PROSPERO with the number CRD420251234154.
2.1. Selection Criteria
Studies eligible for this meta-analysis are required to meet the following criteria: (1) participants included in the study must be patients with mycobacterial infection treated with ethambutol; and (2) the study must be a longitudinal observational study in which the thicknesses of RNFL or GCIPL were measured by OCT before both the administration and the cessation of ethambutol. Articles were excluded if they were reviews, case reports, or case series with fewer than 10 participants, or if they observed patients with EON or other ocular diseases before the administration of ethambutol.
2.2. Search Strategy and Study Selection
We used the following terms to search the electronic databases of PubMed, Embase, and Web of Science (up to November 2025): “OCT”, “optical coherence tomography”, “RNFL”, “GCIPL”, “retinal nerve fiber”, “ganglion cell”, and “ethambutol”. The Medical Subject Headings (MeSH) and other related keywords were used in the search. Additional studies were identified by the review of references. No limits were applied for languages, and papers written in languages except English were translated. There were also no publication status or follow-up period restrictions.
After the deletion of duplicates, the titles and abstracts of all records obtained by the searches were screened to omit reviews, case reports, and studies not related to OCT. The full text of the remaining records was then viewed to select studies eligible for the meta-analysis. All the evaluation of eligibility was performed in an unblinded manner by 2 reviewers, and disagreement was solved by consulting a senior researcher.
2.3. Data Collection and Risk of Bias Assessment
We developed a data extraction sheet to collect data, which was revised after the test on 3 studies selected randomly. We extracted the following information: the first author; the publication year; country; sample size; the proportion of males; the mean age; the dose of ethambutol; the type of OCT devices; the duration of follow-up; and the mean and standard deviation (SD) of the thickness of RNFL, and GCIPL on average and in different subsectors. The data collection was performed by 2 researchers, and disagreement was solved through discussion between the 2 researchers.
The risk of bias of studies included in this meta-analysis was evaluated by using the criteria recommended by the risk of bias in non-randomized studies of interventions (ROBINS-I) [23].
2.4. Data Analysis
The primary outcome measure of this study was the thickness of retinal layers before and after the administration of ethambutol. The meta-analysis was performed if there were 3 or more studies measuring the thicknesses. We conducted the meta-analysis by calculating the standardized mean differences (SMDs) and 95% confidence intervals (CIs) between the retinal layer thicknesses before and after the ethambutol administration using the random-effect model. If the retinal layer thicknesses were measured several times after the ethambutol administration, data obtained after the longest administration period were included in the primary analysis. For studies reporting data for the left and right eyes separately, the data were synthesized by meta-analysis using the random-effect model, and the results were used in the primary analysis. The inconsistency of included studies was evaluated by the I^2^. The risk of bias across studies was assessed by evaluating the funnel plots, and Egger’s test was performed to reduce the subjectivity of the visual evaluation.
We performed a meta-regression to explore the association between the thicknesses of retinal layers and continuous study characteristics, such as the male proportions, the mean ages, and the periods of the ethambutol administration. In addition, subgroup analysis was conducted to evaluate the association between the thicknesses and categorial study characteristics, including countries. Continuous characteristics found to be significantly associated with the thicknesses were split to categorial characteristics, which were included in the subgroup analysis subsequently.
To explore the association between thickness changes in retinal layers and the duration of the ethambutol administration, we performed meta-analyses focusing on retinal layer thicknesses measured after the same period of the ethambutol administration if the thicknesses were measured by more than 3 studies after that period. Further evaluation of retinal layer thickness changes and ethambutol administration periods was conducted by linear regression, analyzing the correlation between the meta-analysis results and the time periods.
All statistical analyses were performed using R software (version 4.5.2) and the package named meta (version 8.2-1) [24]. Continuous variants distributed normally were shown as mean ± standard deviation. Two-sided p-value of less than 0.05 was considered to indicate statistical significance.
3. Results
3.1. Study Selection
Figure 1 summarizes the selection process of studies included in this meta-analysis. The search of PubMed, Embase, and Web of Science electronic databases provided 1599 citations in total, 1352 of which remained after the deletion of duplicates. In total, 1264 records were omitted after the screening of abstracts since these studies were reviews or case reports, or not related to OCT. The full text of the remaining 88 studies, as well as another study identified through the review of references, was reviewed in detail. Seventy-five of them did not meet the selection criteria and thus were removed. The remaining 14 studies were eligible for this systematic review and meta-analysis [11,25,26,27,28,29,30,31,32,33,34,35,36,37]. No unpublished relevant studies were obtained.
3.2. Study Characteristics and Risk of Bias
Table 1 summarizes the characteristics of studies included in this meta-analysis. The included studies involved 1138 eyes of tuberculosis patients treated with ethambutol. Five and four studies were conducted in India and Korea, respectively, and the other studies were conducted in Turkey, Indonesia, Brazil, and Malaysia. The male proportion and mean age were 0.4 to 0.771 and 6.5 to 46.4 years, respectively. The daily doses of ethambutol ranged from 14.72 to 20 mg/kg, and the periods of follow-up ranged from 2 to 8 months. All 12 studies measured RNFL thicknesses, and GCIPL thicknesses were measured in 2 studies conducted by Han, Mandal, and their colleagues [29,33].
The risk of bias was evaluated using the criteria recommended by ROBINS-I. Most of the studies included in the systematic review were at low risk of bias (Table S2).
3.3. RNFL Thickness Changes After the Longest Periods of Ethambutol Administration
No significant changes in RNFL thicknesses occurred in patients after the ethambutol administration compared with baseline (Figure 2), and funnel plots and Egger’s test did not show publication bias (Figure 3).
3.4. Factors Associated with Changes in RNFL Thicknesses
The association between male proportions, mean ages, ethambutol administration periods, and RNFL thickness changes was analyzed by the meta-regression (Figure 4 and Figure S1; Table 2). The association between the RNFL thickness changes and ethambutol dose was not included in the analysis due to the similarity of the dosages in these studies. The results of the analysis revealed a significantly negative correlation between the male proportion and the changes in average, superior, inferior, and nasal RNFL thicknesses, while the temporal subsector showed an insignificant trend. There was a significantly negative association between superior and nasal RNFL thicknesses and the mean age. The period of the ethambutol administration was not significantly correlated with RNFL thickness changes.
The association between countries and the changes in RNFL thicknesses was analyzed by subgroup analysis. Since male proportion and mean age showed significant influences on the RNFL thickness changes, we divided the studies with cut-off values of 2/3 in the male proportion and 40 in the mean age, and we conducted subgroup analysis subsequently. Table 3 and Figure S2 show the results of subgroup analysis. There was a statistically significant decrease in RNFL thicknesses of all subsectors in male-dominant studies and not in female-dominant studies, and the difference between the subgroups was significant in all subsectors except temporal RNFL. The meta-analysis synthesizing studies from Turkey showed a significant decrease in average, inferior, and superior RNFL thicknesses, and results from Indian studies revealed a significant decrease in inferior and temporal RNFL thicknesses. However, the difference among countries was significant only in the inferior RNFL. The RNFL decreases were significant in all subsectors except the temporal RNFL in studies conducted with Cirrus (Carl Zeiss Meditec, Dublin, CA, USA), and the difference among subgroups was significant in the inferior and nasal RNFL. There was no significant difference between subgroups with different mean ages.
3.5. RNFL Thickness Changes After the Same Periods of the Ethambutol Administration
Since RNFL thicknesses 2, 3, 4, and 6 months after the start of the ethambutol administration were reported in more than three studies, we conducted meta-analyses comparing the thicknesses measured at these times and at baseline (Figure 5A and Figure S4, and Table S3). Superior, inferior, nasal, and temporal RNFL thicknesses measured at month 2, and the superior and nasal RNFL thicknesses measured at month 4 showed significant changes when compared with baseline, and the changes in RNFL thicknesses in other subsectors and after other periods of ethambutol administration were not significant.
RNFL thicknesses measured at all time points and subsectors were significantly different from the baseline in male-dominant studies, while meta-analysis combining female-dominant studies did not show significant changes in RNFL thicknesses (Figure 5B and Table S3).
Linear regression analyzing all studies did not show a significant association between RNFL thicknesses and the ethambutol administration period. However, linear regression including male-dominant studies revealed significant decreases in average and inferior RNFL thicknesses with longer ethambutol administration periods, and the decreases in nasal, superior, and temporal RNFL showed a nonsignificant trend. There was no significant relationship between RNFL thicknesses and the ethambutol administration period in the linear regression analysis of all studies or female-dominant studies (Figure 5; Table S3). The inferior RNFL thickness showed a significant increase during ethambutol administration in Korean studies, and those of other subsectors did not show a significant decrease. In addition, the results of linear regression analyzing RNFL thicknesses and the administration period did not reveal significant changes in Indian studies, as well as in studies of both mean age groups (Figure S3; Table S3).
3.6. GCIPL Changes After the Ethambutol Administration
Since only two studies eligible for the systematic review reported GCIPL thicknesses, we focused on describing the results of GCIPL changes after the ethambutol administration rather than meta-analysis (Figure 6 and Table 4). Mandal and colleagues [33] reported significant decreases in GCIPL in all subsectors 2 and 4 months after the start of the ethambutol administration, and the decreases in average, superior, inferior, and superotemporal GCIPL were also significant in month 6. However, Han and colleagues [29] did not find significant changes in GCIPL in any subsectors in months 4 and 6. The male proportions were 0.720 and 0.528 in studies conducted by Mandal and Han and their colleagues, respectively.
4. Discussion
The meta-analysis combining data after the longest periods of ethambutol administration suggested that the effect of ethambutol on RNFL is insignificant overall. However, meta-regression and subgroup analysis revealed heterogeneity of the effect.
Meta-analysis synthesizing studies conducted by different OCT devices showed a significant difference, and the decrease in superior RNFL was more than the test–retest variability of RNFL thickness measured by OCT in previous studies (4.16 to 5.61 μm) [38,39,40,41] in the results synthesizing research conducted by Cirrus (Carl Zeiss Meditec, Dublin, CA, USA). Therefore, differences in RNFL thickness may result from differences in segmentation algorithms, axial resolutions, and standard databases across OCT devices.
Subgroup analysis also showed different effects of ethambutol in patients from different countries, and the thickness changes in superior RNFL in Turkey and inferior RNFL in India were higher than the test–retest variability. This may imply the role of genetic heterogeneity in the development of optic nerve damage induced by ethambutol. Several genes have been found to be related to EON. Zhang and colleagues found optic atrophy-1 (OPA1) gene mutation and Leber hereditary optic neuropathy (LHON)–mitochondrial DNA mutation in 46.8% of EON patients [42]. OPA1 gene mutation was also found in an Indian patient with EON [43]. Since RNFL decrease is a subclinical damage caused by ethambutol, the difference in the decrease may be associated with the distribution of these genes.
In this meta-analysis, the data suggested that sex was related to changes in RNFL thickness caused by ethambutol. There were significant decreases in RNFL thickness in male-dominant studies, which exceeded the test–retest variability of RNFL thickness shown before, while the changes were insignificant in female-dominant studies. Additionally, male-dominant studies showed a significantly negative correlation between RNFL thicknesses and periods of the ethambutol administration. There were only two studies reporting GCIPL changes, and the study involving a higher proportion of males showed a significant decrease in GCIPL thicknesses, while the change in the other study was insignificant. This result was consistent with a retrospective study conducted by Guo and colleagues [18] which observed EON patients for 12 months and found a slower RNFL thinning in female patents compared to males. In addition, another retrospective study revealed better recovery in female EON patients [44]. Therefore, the data in this systematic review suggested higher risks of these changes in male patients treated with ethambutol, and a regular OCT test may be useful in the early diagnosis of EON and necessary for patients treated with ethambutol, especially for male patients.
The gender bias in ethambutol-induced ocular damage may be associated with the pathogenesis, in which ethambutol-induced mitochondrial dysfunction may play a role. Retinal nerve fibers are unmyelinated before they form optic nerves, and this process allows them to maintain the transparency of the retina, but it leads to higher energy demands and vulnerability to oxidative stress in these fibers [45], thereby contributing to EON. LHON is the mitochondrial optic neuropathy that has been studied most thoroughly, and the male–female ratio was approximately 3:1 [46]. The gender bias in LHON was considered to be associated with estrogens and exposure to tobacco and alcohol [47,48,49]. Therefore, these factors may also lead to a higher risk of ethambutol-induced ocular damage in males.
The association with male predominance may also be influenced by confounding factors. First, the prevalence of smoking is higher in males worldwide [50], including India [51], Turkey [52], and Korea [53], where most included studies were held. Smoking has been reported as an independent risk factor for EON [2] and may also cause subclinical damage. Second, research conducted in India, Turkey, and Indonesia tended to recruit patients with a higher male proportion than those conducted in Korea and Brazil. Therefore, regional variation may also contribute to the gender difference. Third, males were at a higher risk of tuberculosis infection and had a more severe form of the disease [54,55] and lower adherence to anti-tuberculosis treatment [56,57]. Therefore, the RNFL decrease in male patients may be associated with the higher levels of inflammation caused by tuberculosis and substandard treatment.
Previous studies have reported numerous factors correlated with EON, including age, ethambutol dosage, treatment period, smoking, hypertension, diabetes, and renal diseases [2,4,6,7]. However, since studies eligible for the meta-analysis did not report information about smoking, hypertension, diabetes, and renal diseases, and patients included in these studies were treated with ethambutol of similar dosage, the association between these factors and retinal layer thicknesses was not analyzed in this study.
This study did not find a significant association between mean ages and RNFL thickness changes, except nasal RNFL. A possible reason is that a significantly increased risk of ethambutol-induced ocular damage was observed in patients aged more than 40 years, especially in those more than 65 years [58]. Therefore, the limited range of mean ages reported by the included studies (28.1 to 46.4 years, except the study by Mane et al. [31]) may not be wide enough to reveal the association.
Our study has several limitations. First, this is a meta-analysis synthesizing data from observational studies. Therefore, selective and confounding biases are inevitable. For example, several studies showed the ocular toxicity of isoniazid [59,60] and the neuroprotective effects of rifampicin [61], which were also involved in these studies and may lead to the misestimation of the changes caused by ethambutol. Second, ethambutol has been proven to be effective in the treatment of tuberculosis for a long time, and OCT is a relatively novel device to detect the retinal layer thicknesses. Therefore, control groups without the administration of ethambutol were not included due to ethical reasons, and these studies were self-controlled. Since tuberculosis may also affect the ocular region [62], the changes in retinal layer thicknesses may be related to subclinical damage induced by tuberculosis. Third, there were only 14 studies eligible for the meta-analysis due to the limited availability of literature sources. Therefore, the small number of studies may not be enough to detect the RNFL thickness changes caused by ethambutol and related factors. The limited data also led to the absence of meta-analyses focusing on GCIPL thickness changes. Fourth, there may be a lack of power to detect RNFL thickness changes in the statistical analysis. Since most participants enrolled in these longitudinal studies underwent detection of RNFL thicknesses before and after the ethambutol administration, paired t-tests were used in these studies. Paired t-test was able to increase the power to detect the RNFL thickness changes since it reduced the individual differences that are independent of the changes caused by ethambutol. Therefore, a meta-analysis of paired t-tests was more appropriate for this study. However, SDs of RNFL changes or the correlation coefficients between RNFL before and after the ethambutol administration were needed in the calculation (Appendix A), and neither of them were reported in these studies. For this reason, we calculated the SMDs through the statistical methods typically used to synthesize unpaired data, which may reduce the power to detect the RNFL thickness changes. Fifth, although this study illustrated the RNFL changes in patients treated with ethambutol, the relationship between the decrease in RNFL and the risk of EON remains unclear. Therefore, further studies are needed to clarify the diagnostic value of OCT in subclinical EON.
5. Conclusions
In summary, the results of our meta-analysis suggest that ethambutol administration does not cause significant RNFL changes generally in patients with mycobacterial infection. However, RNFL thickness is reduced in male patients and patients in some countries after ethambutol administration. Further studies are needed to explore the relationship between ethambutol dosages, systemic diseases, smoking, and the changes in RNFL thickness, and the predictive value of RNFL in the development of EON in the future. In addition, we need more research to observe the thickness changes in other retinal layers in patients with ethambutol administration and without EON.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Singh P. Karkhur S. Verma V. Ethambutol-Induced Optic Neuropathy: A Retrospective Study of Incidences and Risk Factors Cureus 202517 e 7916010.7759/cureus.7916040109812 PMC 11921821 · doi ↗ · pubmed ↗
- 2Chaitanuwong P. Srithawatpong S. Ruamviboonsuk P. Apinyawasisuk S. Watcharapanjamart A. Moss H.E. Incidence, Risk Factors and Ophthalmic Clinical Characteristic of Ethambutol-Induced Optic Neuropathy: 7-Year Experience Front. Ophthalmol.20233115221510.3389/fopht.2023.115221538983080 PMC 11182281 · doi ↗ · pubmed ↗
- 3Kim J. Kwon H.Y. Ahn S.J. Nationwide Usage of Ethambutol and Incidence and Screening Practices of Optic Neuropathy Front. Pharmacol.202415146111110.3389/fphar.2024.146111139474613 PMC 11518835 · doi ↗ · pubmed ↗
- 4Lee S. Ryu W.Y. Kang D. Lee J.K. Prevalence and Incidence of Ethambutol-Induced Optic Neuropathy and Its Risk Factors in Korea: A Nationwide Population-Based Study J. Korean Med. Sci.202540 e 6510.3346/jkms.2025.40.e 6540425190 PMC 12105990 · doi ↗ · pubmed ↗
- 5Liu S.-S. Feng S.-C. Wu M.-F. Chin C.-S. Chen H.-C. Huang W.-C. Programmatic Assessment of Ethambutol-Related Optic Neuropathy in Patients with Mycobacterial Infections: A Prospective Observational Cohort Study Infect. Dis. Ther.2025142391240410.1007/s 40121-025-01219-x 40900291 PMC 12480191 · doi ↗ · pubmed ↗
- 6Kim J. Ahn S.J. Risk Factors of Optic Neuropathy in Ethambutol Users: Interaction with Isoniazid and Other Associated Conditions of Toxic Optic Neuropathy Toxics 20241254910.3390/toxics 1208054939195651 PMC 11359443 · doi ↗ · pubmed ↗
- 7Lee E.J. Kim S.-J. Choung H.K. Kim J.H. Yu Y.S. Incidence and Clinical Features of Ethambutol-Induced Optic Neuropathy in Korea J. Neuro-Ophthalmol.20082826927710.1097/WNO.0b 013e 31818 e 3c 6b 19145123 · doi ↗ · pubmed ↗
- 8Sudhakar P. Acharya K. Kini T.A. Ethambutol Optic Neuropathy Front. Neurol.202516162690910.3389/fneur.2025.162690941018187 PMC 12460111 · doi ↗ · pubmed ↗