Nurses’ Experience in Providing End-of-Life Care in Intensive Care Unit: A Scoping Review
Y. Dodi Setyawan, Indah Ayu Susanti, Cecep Eli Kosasih, Hartiah Haroen

TL;DR
This review explores the challenges ICU nurses face when providing end-of-life care, highlighting the need for better training and support.
Contribution
A comprehensive synthesis of ICU nurses' experiences in end-of-life care, identifying key themes and implications for nursing practice.
Findings
ICU nurses face emotional and moral challenges in end-of-life care.
Cultural and spiritual factors significantly influence EoLC experiences.
Organizational support and training are critical for improving EoLC quality.
Abstract
Background: Most ICU patients are in the terminal phase and require complex palliative care support and End-of-Life Care (EoLC). Nurses play a central role in symptom management, emotional support, and shared decision-making. However, evidence on nurses’ experiences in providing EoLC remains fragmented and lacks a comprehensive synthesis. Objective: This review aimed to identify, map, and synthesize global evidence on ICU nurses’ experiences in delivering EoLC, including challenges, coping strategies, and implications for critical care nursing practice. Methods: A scoping review was conducted following Arksey and O’Malley’s framework and PRISMA-ScR guidelines. Systematic searches were performed in the PubMed, Scopus, and EBSCOhost databases for studies published between 2015 and 2025. Thematic analysis was applied to the qualitative studies to identify patterns and key issues. Results:…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
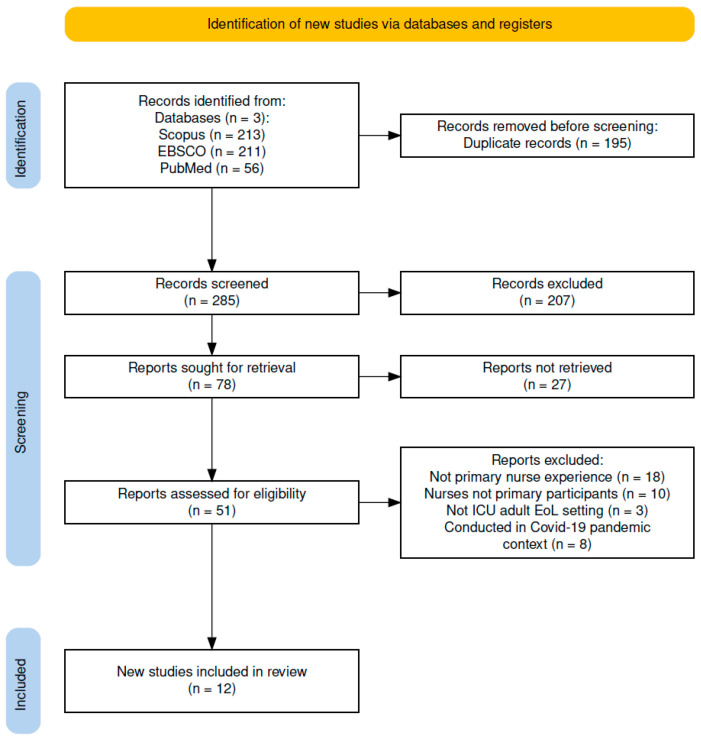 Figure 1
Figure 1- —Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPalliative Care and End-of-Life Issues · Family and Patient Care in Intensive Care Units · Intensive Care Unit Cognitive Disorders
1. Introduction
End-of-Life Care (EoLC) in Intensive Care Units (ICUs) has gained substantial global attention over the past two decades. Since 2014, the World Federation of Intensive and Critical Care Medicine has identified EoLC as a strategic priority for addressing existing challenges and promoting the development of regional and national guidelines [1]. Many ICU patients die during their ICU stay, and most hospital deaths occur in these units [2,3]. Considerable variability in EoLC practices, including decisions on limiting life-sustaining treatment, remains evident across countries and healthcare systems, reflecting disparities in economic resources and differences in legal, ethical, and cultural norms [2,4,5].
EoLC in ICUs requires complex symptom management, psychosocial and spiritual support, and shared decision-making among patients, families, and multidisciplinary teams [6,7]. This approach integrates bioethical principles and relies on clear, compassionate communication that reflects patients’ cultural values [6,8]. However, implementation is often hindered by prognostic uncertainty, ethical dilemmas, conflict with families or within teams, and emotional strain among healthcare professionals [9,10]. These challenges can heighten nurses’ moral distress and exacerbate the suffering of patients and their families [8].
Demographic shifts have increased demand for integrated EoLCs in ICUs. Critically ill populations now largely consist of older adults with chronic complex comorbidities [11,12]. While advanced technology has improved survival, it has also intensified dilemmas surrounding aggressive treatments that may prolong the dying process without enhancing quality of life [13,14]. As ICUs increasingly become environments where end-of-life decisions occur, nurses require strong clinical skills, communication capabilities, cultural sensitivity, and interprofessional collaboration to deliver compassionate, patient-centered care [15,16].
Despite their essential role, ICU nurses frequently experience significant psychological, physical, and moral burdens when providing EoLC [17,18]. Moral distress, compassion fatigue, staffing shortages, and insufficient training in end-of-life communication are major barriers to high-quality practice [19,20]. Limited communication failure among professionals and lack of emotional support exacerbate these challenges [21]. Thus, institutional support and continuous education are critical for enhancing nurses’ capacity to deliver effective EoLCs [22,23,24].
Although many qualitative studies have explored ICU nurses’ experiences with EoLC, the existing evidence is fragmented, context-specific, and lacks comprehensive synthesis. Prior reviews often focused on particular regions, narrow aspects of EoLC, or specific clinical populations [25,26]. Consequently, major gaps remain regarding (a) the full spectrum of challenges nurses face, (b) coping or adaptation strategies they use, and (c) enabling factors that support high-quality EoLCs across diverse settings. Additionally, difference in standardized operational guidelines contribute to variability in EoLC practices worldwide. Given these gaps, this scoping review aimed to synthesize scientific evidence on ICU nurses’ experiences in providing EoLC across diverse international contexts. Specifically, it explored the challenges encountered, coping strategies employed, and implications for critical care nursing practice. The findings are expected to guide policy formulation that support patient-centered and culturally sensitive EoLCs.
2. Materials and Methods
2.1. Study Design
This scoping review adopted Arksey and O’Malley’s methodological framework and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) reporting guidelines [27]. The PRISMA 2020 flow diagram is presented in Figure 1, and the completed PRISMA 2020 checklist is provided in the Supplementary Material. This approach was appropriate for exploring and mapping emerging evidence on ICU nurses’ experiences in providing EoLCs. The primary research question guiding this review was How are ICU nurses’ experiences in delivering EoLC reported in international qualitative literature? To ensure transparency, the protocol for this review was retrospectively registered in the Open Science Framework (OSF) (registration DOI: 10.17605/OSF.IO/GWMQS).
2.2. Eligibility Criteria
Inclusion criteria were defined using the population–concept–context (PCC) framework. The study population consisted of nurses working in ICUs with at least six months to ≥one year of ICU experience. The concept of this study is the nurses’ experiences related to providing EoLC, including challenges, coping strategies, professional roles, and organizational support. The context of this study was All ICU types across diverse healthcare systems and cultural settings worldwide. Additional inclusion criteria were qualitative or mixed-method studies with identifiable qualitative data, peer-reviewed journal articles, publications in English between 2015 and 2025, and availability of full-text versions. This time frame was selected to capture contemporary evidence reflecting recent developments in ICU practices, evolving ethical frameworks, and current organizational and cultural contexts of end-of-life care.
During full-text screening, we include studies focusing exclusively on end-of-life decision-making without exploring nurses’ experiential perspectives, mixed-methods, studies lacking qualitative components, and studies addressing palliative care in non-ICU settings. Moreover, the exclusion criteria consisted of non-empirical publications (e.g., editorials, commentaries, opinion papers, conference abstracts) and non-peer-reviewed preprints.
2.3. Search Strategy
A comprehensive literature search was conducted in PubMed, Scopus, and EBSCOhost (Medline) databases on 6 September 2025. The search strategy combined controlled vocabulary (Medical Subject Headings/MeSH; Cumulative Index to Nursing & Allied Health Literature/CINAHL Headings) and free-text terms by using Boolean operators. The search was limited to studies published between 2015 and 2025, in accordance with the predefined eligibility criteria. Only studies published in English were included because of feasibility constraints. Complete reproducible search strings for each database include: PubMed: ((“Intensive Care Units”[Mesh] OR “Critical Care”[Mesh] OR “intensive care”[tiab] OR ICU[tiab]) AND (“Nurses”[Mesh] OR nurse*[tiab] OR “registered nurse”[tiab]) AND (“Terminal Care”[Mesh] OR “Palliative Care”[Mesh] OR “end-of-life care”[tiab] OR EoLC[tiab]) AND (experience*[tiab] OR perception*[tiab] OR perspective*[tiab])). Scopus: (TITLE-ABS-KEY (“intensive care” OR “critical care” OR ICU) AND TITLE-ABS-KEY (nurse* OR “registered nurse”) AND TITLE-ABS-KEY (“end of life” OR “end-of-life care” OR “palliative care” OR “terminal care”) AND TITLE-ABS-KEY (experience* OR perception* OR perspective*)). EBSCOhost (CINAHL): ((MH “Intensive Care Units” OR “intensive care” OR ICU) AND (MH “Nurses” OR nurse* OR “nursing personnel”) AND (MH “Terminal Care” OR MH “Palliative Care” OR “end-of-life care”) AND (experience* OR perception* OR perspective*)).
2.4. Study Screening and Selection Process
Two reviewers (YDS and IAS) independently screened titles, abstracts, and full-text articles using predefined eligibility criteria. The Rayyan.ai was utilized to support the screening process, identify duplicate records, and manage blinded reviewer decisions, whereas Mendeley (version 19.8) was used for reference management. Any discrepancies between the two reviewers were discussed to reach a consensus; when disagreements persisted, a third reviewer (HH) adjudicated the final decision.
2.5. Data Extraction and Quality Appraisal
Data extraction was conducted independently by two reviewers (YDS and IAS) using a standardized worksheets. Extracted information included author(s), year of publication, country, study design, participants, ICU setting, and key findings related to ICU nurses’ experiences with EoLC. Any discrepancies in the extracted data were resolved through consensus discussions, and a third reviewer was consulted when agreement was not reached.
2.6. Data Analysis and Thematic Synthesis
Thematic synthesis followed the three-stage approach of Thomas and Harden: (1) line-by-line coding, (2) development of descriptive themes, and (3) generation of analytical themes. Two reviewers (YDS and HH) independently conducted line-by-line coding of the findings sections of the included studies. The initial codes were inductively derived and grouped into categories based on conceptual similarity. The categories were iteratively refined into overarching descriptive themes through constant comparisons across studies.
Analytical themes were subsequently generated through interpretive synthesis integrating recurring patterns, contextual nuances, and conceptual relationships beyond the descriptive level. Discrepancies in coding and theme development were resolved through discussion or adjudication by a third reviewer. Rigor was ensured through independent coding, analytic memoing, audit trials, and triangulation across reviewers (YDS, HH).
3. Results
3.1. Study Selection
The database search yielded 480 records (Scopus, 213; EBSCO, 211; PubMed, 56). After removing 195 duplicate records, 285 unique records were subjected to title and abstract screenings. Of these, 207 were excluded because of irrelevance. A total of 78 full-text articles were retrieved, of which 27 could not be accessed. The remaining 51 full-text articles were assessed for their eligibility. During the 39 full-text screening, studies were excluded for several reasons, including not focusing on ICU nurses’ experiences (n = 18), not being the primary study participants (n = 10), not being conducted in adult ICU end-of-life care settings (n = 3), and being conducted within the COVID-19 pandemic context (n = 8). Ultimately, 12 qualitative studies met all inclusion criteria and were included in the review. The complete study selection process is presented in the PRISMA 2020 flow diagram (Figure 1).
3.2. Study Characteristics
The 12 included studies were conducted across diverse geographic regions, including Europe (Sweden and Spain), Asia (South Korea, China, and Saudi Arabia), Oceania (New Zealand), the Americas (Canada and Brazil), and Africa (Ghana). All studies utilized qualitative methodologies employing phenomenological, descriptive–interpretive, descriptive–exploratory, or ethnographic designs to investigate ICU nurses’ experiences in providing EoLC. The sample sizes varied widely, ranging from 9 to 100 ICU nurses. Most studies were conducted in adult ICU settings within tertiary or university-affiliated hospitals, although several involved multi-center designs or included specialized units such as general ICUs, neuro, trauma, cardiac, or post-anesthetic care units. Participants predominantly consisted of registered ICU nurses with varied levels of professional experience, and one study specifically focused on male ICU nurses. A summary of the key characteristics of the included studies is shown in Table 1.
3.3. Experiences and Challenges of ICU Nurses in Providing EoLC
The thematic synthesis of 12 qualitative studies generated five overarching themes that reflect the emotional, cultural, ethical, and organizational complexities shaping ICU nurses’ experiences in providing EoLC. Table 2 summarizes the major themes and subthemes.
3.3.1. Emotional and Moral Challenges
ICU nurses frequently encounter intense emotional and moral strains while delivering EoLCs. Their close proximity to patient suffering and end-of-life decision-making exposes them to uncertainty, ethical dilemmas, and repeated contact with death, leading to moral distress and value conflict [28,30,35]. Such distress commonly arises when institutional expectations, such as prolonging life-sustaining treatment, conflict with nurses’ clinical judgment and ethical commitment to holistic care [30,32].
Several studies have highlighted that nurses experience profound emotional burdens, including guilt, helplessness, and emotional fatigue, particularly when they perceive treatment as non-beneficial but remain obligated to follow directives shaped by hierarchical decision-making structures [32,37]. Ethical discomfort is heightened during withdrawal of life-sustaining therapy, where nurses feel directly implicated in decisions culminating in patient death, despite limited decision-making authority [37,38].
To manage these pressures, nurses often rely on coping strategies such as emotional distancing or seeking college support, although the effectiveness of such strategies varies widely across clinical environments [28,38]. The evidence collectively indicates that emotional and moral distress is pervasive within the ICU EoLC, reflecting both systemic and interpersonal contributors [37,38].
3.3.2. Cultural and Spiritual Influences
Culture and spirituality strongly shape nurses’ interpretations of death, communication styles, and decision-making during the EoLC. Religious beliefs and cultural norms influence how nurses respond to patient suffering and how they support families in navigating grief and uncertainty [29,33]. In settings where discussing death remains culturally sensitive, nurses may struggle to deliver honest prognostic information, adding emotional complexity to their roles [29,34]. However, providing care to patients from diverse religious backgrounds introduces additional ethical and emotional complexities, requiring nurses to demonstrate high cultural sensitivity, particularly around rituals, family involvement, and expectations for a peaceful death [33,36]. Moreover, cultural diversity within nursing teams creates unique interpersonal dynamics. Nurses who share patient cultural backgrounds often act as informal cultural mediators, which may contribute to cultural fatigue due to repeated cross-cultural role demands [34,36]. Respecting cultural and spiritual values are consistently viewed as essential to safeguard patient dignity [34,39].
3.3.3. Interprofessional Communication and Collaboration
Effective interprofessional communication is foundational for high-quality EoLC, particularly during ethically complex decisions such as withdrawal of treatment [32,37]. However, evidence consistently shows that nurses are frequently marginalized in their decision-making processes. When physicians or families dominate discussions, nurses experience frustration and a sense of powerlessness, as their unique insights grounded in close bedside interactions are not fully acknowledged [5,37]. Additionally, communication barriers and rigid hierarchies intensify moral distress, creating misalignments between medical directives and ethical nursing perspectives [28,32]. These dynamics reduce team cohesion and contribute to emotional conflict during critical care decisions.
Despite these challenges, nurses actively work to promote collaboration by facilitating communication between physicians and families and ensuring clarity and emotional support during patient deterioration [5,28,40]. Their role as communicative bridges helps integrate psychosocial and spiritual needs into medical decision-making. Studies emphasize that open, inclusive communication enhances ethical clarity, strengthens team-based decision-making, and supports patient-centered EoLC [5,32,37].
3.3.4. Professional Development and Organizational Support
Providing EoLCs in ICU settings requires substantial professional competence and psychological resilience. Many nurses, especially those with limited experience, feel inadequately prepared for emotionally intense encounters with patient deaths [34,41]. Targeted training in empathetic communication, reflective practice, and ethical reasoning increases nurses’ confidence, emotional readiness, and ability to provide compassionate care [35,41].
Insufficient organizational support is associated with heightened emotional exhaustion and moral distress. Interventions such as debriefing sessions, peer consultation, and stress management programs contribute significantly to nurses’ psychological resilience and reduce the risk of burnout [30]. These structured supports help nurses process emotional strain and maintain their professional integrity.
Experienced nurses demonstrate a greater capacity for ethical reflection, enabling them to navigate complex moral dilemmas more effectively [5]. Work environments that foster reflective practice and interprofessional dialog enhance both individual well-being and the overall quality of EoLC. Moreover, when organizations provide training, mentorship, and conducive work structures, nurses are better equipped to deliver empathetic patient-centered care. Conversely, a lack of institutional support increases vulnerability to emotional fatigue and diminishes professional meaning [5].
3.3.5. Organizational and Resource-Related Factors
The quality of EoLCs in ICUs is heavily influenced by organizational conditions, including staffing, workload, and clarity of institutional policies. High patient acuity combined with staffing shortages contribute to emotional exhaustion, limited capacity for holistic care, and reduced job motivation among nurses [30]. Resource scarcity, including inadequate equipment and limited physical space, further constrains nurses’ ability to meet patient needs and intensifies feelings of helplessness and moral distress [30,32]. Organizational hierarchies and poor communication structures exacerbate emotional strain, particularly when nurses feel excluded from critical end-of-life decisions [29,32]. Additionally, systemic barriers, such as overcrowded environments, absence of EoLC-specific guidelines, and pressure for maximal medical intervention, complicate the delivery of dignified and comfort-oriented care. Imbalances in interprofessional roles diminish nursing autonomy and elevate work-related stress, undermining collaboration and professional satisfaction [5,29,32].
4. Discussion
4.1. Main Findings
This scoping review found that the multidimensional challenges experienced by ICU nurses in delivering EoLC. Five overarching themes were identified: (1) emotional and moral challenges; (2) cultural and spiritual influences; (3) interprofessional communication and collaboration; (4) professional development and organizational support; and (5) organizational and resource-related factors.
This review showed emotional and moral challenges emerged consistently as the most prominent themes across the included studies. ICU nurses frequently reported a psychological burden when delivering life-sustaining treatments perceived as non-beneficial or misaligned with patient values. Moral distress, manifested through feelings of guilt, powerlessness, and value conflict, was frequently described in situations where nurses disagreed with the treatment decisions made by physicians or family members [18,42]. Previous evidence further links moral distress with burnout, emotional exhaustion, and decreased retention in critical care environments [18]. Additional literature reinforces these findings, showing that structured interventions such as clinical debriefings, facilitated ethical reflection, and peer support programs can significantly decrease emotional burden and strengthen resilience among ICU nurses [42]. Collectively, these insights emphasize the importance of organizational strategies that acknowledge both the emotional labor and ethical complexities inherent in the EoLC.
The findings of this review underscore the need for cultural humility and integration of spiritual sensitivity into routine EoLC practices. Cultural and spiritual contexts strongly shaped how nurses navigated the EoLC. Religious beliefs, family hierarchies, and culturally grounded expectations about death influence communication, decision-making, and perceptions of a “good death” [28,36]. The Theory of Planned Behavior (TPB) provides a useful interpretive framework, suggesting that attitudes, subjective norms, and perceived behavioral control shape nurses’ intentions and behaviors in EoLC settings [43]. Broader scholarship indicates that cultural norms and family centered decision-making can either support or constrain nurses’ clinical judgment, emotional comfort, and willingness to participate in EoLC discussions.
This review also highlights that effective interprofessional communication is another essential determinant of high-quality EoLC. Most nurses reported being excluded from decision-making processes regarding prognosis, treatment withdrawal, or goals of care despite their central role in bedside monitoring [37,42]. Hierarchical structures, inconsistent communication, and limited interdisciplinary dialog have contributed to frustration and intensified moral distress. Another evidence suggest the benefits of structured communication frameworks, regular interdisciplinary meetings, and family conferences in improving team coordination, clarifying roles, and reducing conflicts [44]. These findings highlight the need to strengthen collaborative structures to meaningfully integrate nursing perspectives into shared decision-making processes.
A consistent finding across studies was nurses’ perceptions of inadequate preparation for the emotional, ethical, and clinical complexities associated with EoLC. Formal training programs, such as the End-of-Life Nursing Education Consortium (ELNEC), have been shown to enhance communication, ethics, and clinical competence [45,46,47]. Complementary approaches, including reflective practice, mentorship, and supportive supervision, can further reduce emotional burden and foster ongoing professional development [48,49]. Therefore, sustained organizational investment in education and support systems is important to promote competence and confidence across all levels of nursing experience.
Institutional factors, including chronic understaffing, high workloads, limited resources, and inconsistent protocols, have a substantial impact on nurses’ EoLC experiences. These challenges often hinder the delivery of compassionate and ethically grounded care [29,30]. Evidence shows that supportive leadership, clear guidelines, collaborative team cultures, and adequate staffing ratios enhance nurses’ perceived behavioral control within the TPB framework, thereby strengthening their confidence and capacity to provide high-quality EoLC [50,51,52,53].
4.2. Study Limitations
This study had several limitations. First, a large proportion of the included studies were conducted in Asian and Middle Eastern contexts, which may have introduced cultural bias. Sociocultural norms in these regions, such as hierarchical clinical decision-making, strong family involvement, and culturally specific interpretations of death and dying, may shape nurses’ experiences differently than those in Western or multicultural ICU settings, thus limiting transferability. Second, the evidence base consisted predominantly of qualitative studies, resulting in limited opportunities for methodological triangulation or quantitative comparisons to further validate the identified thematic patterns. Third, although a comprehensive search strategy was applied across the three major databases, restricting the review to English-language publications and excluding inaccessible full texts may have led to language and retrieval bias. Finally, methodological variability across the included studies, such as incomplete reporting of reflexivity, sampling strategies, contextual descriptions, or analytic rigor, may have affected the consistency, depth, and comparability of findings within the synthesis.
4.3. Implications for Practice and Research
Reflective and psychologically supportive interventions have been demonstrated to be effective in reducing moral distress and strengthening resilience among ICU nurses. Routine debriefings, ethics rounds, and peer support initiatives facilitate ethical communication, enhance moral courage, and reduce emotional exhaustion [33,54,55]. Moreover, programs such as ELNEC significantly improve nurses’ competencies in communication, symptom management, and ethical decision-making [46,48,56]. Continuous education, simulation-based learning, and technology-enhanced training strengthen self-efficacy and empathy in caring for terminally ill patients [57,58]. Integrating cultural and spiritual competence training ensures holistic and equitable EoLC [59,60]. Cultural reflection-based training and structured interprofessional communication approaches help reduce disparities and enhance the alignment between clinical decisions and patient values [59,61,62]. Simulation-based interprofessional education fosters teamwork and role clarity [63,64]. Incorporating culturally sensitive and spiritually informed care practices improves patients and families [64].
In addition, compassionate and supportive leadership positively influenced the nurses’ well-being and EoLC performance. Perceived organizational support mitigates the impact of workload on burnout [22], while leadership grounded in empathy helps establish a healthy resilience-promoting work culture [65,66]. Moreover, Enhanced interprofessional collaboration and structured family involvement support shared decision-making and improve satisfaction with care [67,68]. Cultural and spiritual competence across healthcare teams further supports sensitive, value-oriented EoLC [39,69,70]. Multidisciplinary spiritual care models show evidence of improved patient quality of life and family experiences [70].
Moreover, these recommendations should follow the future studies to providing evidence-based recommendation. Future studies should evaluate the effectiveness of reflective practices, peer support programs, interprofessional training, and compassionate leadership models on both caregiver and patient outcomes. Longitudinal and cross-cultural research is required to examine the adaptability and impact of moral resilience and cultural competence interventions in diverse healthcare environments. There is also a need to develop validated measurement tools for spiritual competence, inter-professional collaboration, and psychological outcomes among ICU nurses. Mixed-methods study and evaluation designs are recommended to generate context-sensitive evidence-based guidelines for EoLC.
5. Conclusions
This scoping review mapped the current evidence on ICU nurses’ experiences in providing EoLCs. The findings indicated that nurses navigate a range of emotional, ethical, cultural, professional, and organizational challenges; however, these experiences vary across settings, cultures, and healthcare systems. This review suggests that emotional burden, moral dilemmas, communication barriers, and cultural considerations are commonly reported, but the extent and expression of these challenges differ among the included studies. This synthesis highlights the potential value of strengthening institutional support, enhancing ethical reflection, and incorporating cultural and spiritual sensitivity into EoLC practices. These insights should be interpreted as indicative rather than definitive patterns given the predominance of qualitative designs and contextual diversity. Future research may benefit from developing and evaluating context-specific interventions, such as structured education, psychosocial support, and culturally responsive interprofessional collaboration, to better understand how these strategies influence nurses’ well-being and quality of care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Myburgh J. Abillama F. Chiumello D. Dobb G. Jacobe S. Kleinpell R. Koh Y. Martin C. Michalsen A. Pelosi P. End-of-life care in the intensive care unit: Report from the Task Force of World Federation of Societies of Intensive and Critical Care Medicine J. Crit. Care 20163412513010.1016/j.jcrc.2016.04.01727288625 · doi ↗ · pubmed ↗
- 2Avidan A. Sprung C.L. Schefold J.C. Ricou B. Hartog C.S. Nates J.L. Jaschinski U. Lobo S.M. Joynt G.M. Lesieur O. Variations in end-of-life practices in intensive care units worldwide (Ethicus-2): A prospective observational study Lancet Respir. Med.202191101111010.1016/S 2213-2600(21)00261-734364537 · doi ↗ · pubmed ↗
- 3Martin-Loeches I. Sprung C.L. Wolsztynski E. Cusack R. Lobo S.M. Protti A. Avidan A. End-of-life decision disparities according to the gross national income in critically ill patients: A secondary analysis of the ETHICUS-2 study Ann. Intensive Care 2025152910.1186/s 13613-025-01419-140055260 PMC 11889315 · doi ↗ · pubmed ↗
- 4Brooks L.A. Manias E. Nicholson P. Communication and decision-making about end-of-life care in the intensive care unit Am. J. Crit. Care 20172633634110.4037/ajcc 201777428668920 · doi ↗ · pubmed ↗
- 5Xu D.D. Li J. Ding X.B. Ma J. Hou R.T. Chen N.N. Cheng X.L. Hu F. Experiences of providing end-of-life care in adult intensive care units: A qualitative study BMC Nurs.20252476810.1186/s 12912-025-03340-140598520 PMC 12211952 · doi ↗ · pubmed ↗
- 6Vincent J.-L. End-of-life issues in the intensive therapy unit: 10 important points to remember Eur. Heart J. Acute Cardiovasc. Care 20251424524910.1093/ehjacc/zuaf 01139834171 · doi ↗ · pubmed ↗
- 7Mc Curry I. Jennett P. Oh J. White B. Delisser H.M. Chaplain Care in the Intensive Care Unit at the End of Life: A Qualitative Analysis Palliat. Med. Rep.2021228028610.1089/pmr.2021.001234927154 PMC 8675270 · doi ↗ · pubmed ↗
- 8Gallagher A.M. Szylit R. Mc Carthy J. Kohlen H. Andrews T. Paganini M.C. Abu-El-Noor N.I. Cox A.C. Haas M. Arber A. Negotiated reorienting: A grounded theory of nurses’ end-of-life decision-making in the intensive care unit Int. J. Nurs. Stud.20155279480310.1016/j.ijnurstu.2014.12.00325648380 · doi ↗ · pubmed ↗