The Role of Sex Hormone-Binding Globulin (SHBG) as a Marker of Metabolic Dysfunction-Associated Steatotic Liver Disease, with an Extended Analysis in Both Men and Women
Ljiljana Fodor Duric, Zrinka Čolak Romić, Dino Pavičić, Josip Čurić, Velimir Belčić, Ivija Rajković, Irijana Rajković, Jelena Muslim, Nikolina Basic Jukic, Bozidar Vujicic, Tonko Gulin, Matko Gulin, Mladen Grgurević, Anja Oberiter Korbar

TL;DR
This study shows that SHBG levels are lower in people with liver disease linked to metabolic issues, especially in women, and highlights how SHBG connects to factors like age, BMI, and hormones.
Contribution
The study extends prior male-only research by including both men and women, revealing sex-specific associations between SHBG and MASLD.
Findings
SHBG levels were significantly lower in individuals with MASLD compared to controls.
SHBG reduction was more pronounced in women with MASLD.
SHBG levels correlated with estradiol, age, cholesterol, and triglycerides differently by sex.
Abstract
Introduction: Metabolic dysfunction-associated steatotic liver disease (MASLD) is associated with insulin resistance and metabolic disturbances. Sex hormone-binding globulin (SHBG) is closely linked to metabolic regulation and has been shown to differ between individuals with and without MASLD. Objective: This study aimed to investigate the associations between SHBG and MASLD and their relationships with insulin resistance, body mass index (BMI), age, and sex in a combined male–female cohort. Patients and Methods: We studied 98 men and 54 women with MASLD and 74 men and 55 women without MASLD (aged 25–64 years). Participants underwent abdominal ultrasonography and fasting blood sampling, including measurements of glucose, liver enzymes, lipids, insulin, SHBG, estradiol, and testosterone. Results: SHBG levels were lower in individuals with MASLD than in controls, with a more pronounced…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
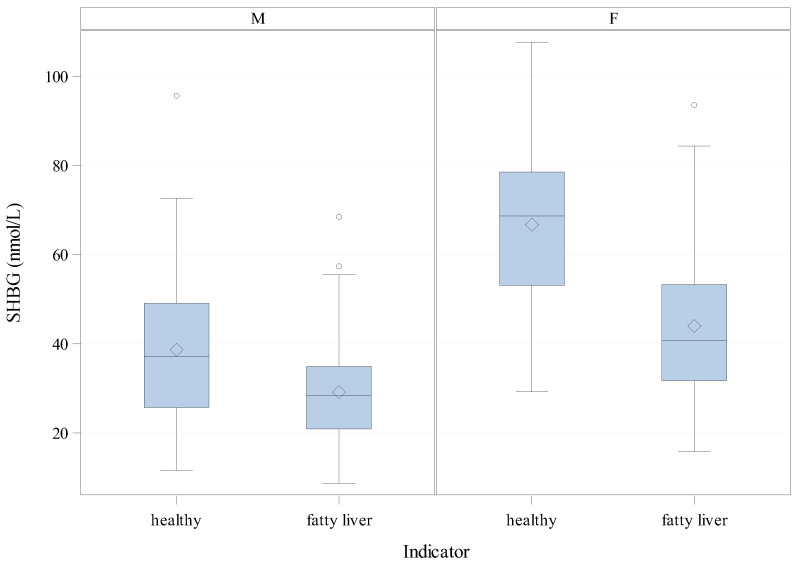 Figure 1
Figure 1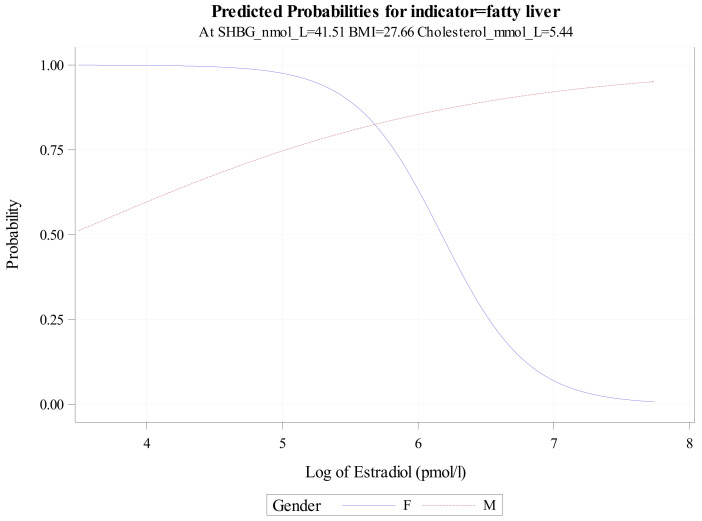 Figure 2
Figure 2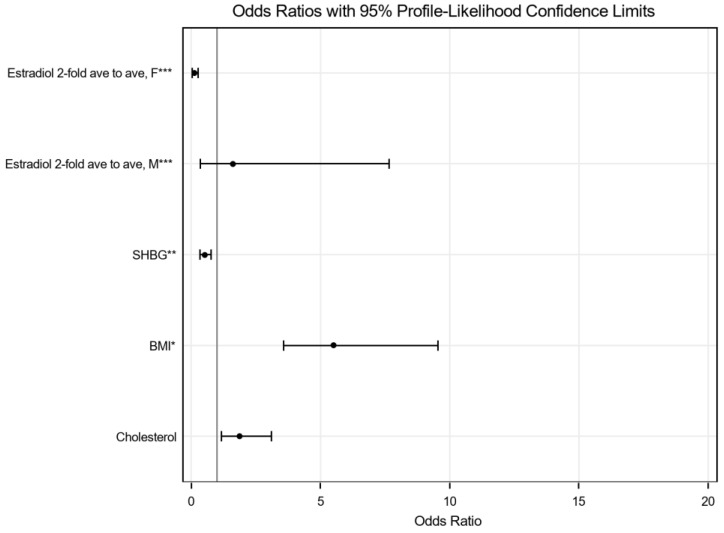 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHormonal and reproductive studies · Liver Disease Diagnosis and Treatment · Diabetes, Cardiovascular Risks, and Lipoproteins
1. Introduction
Fatty liver, or metabolic dysfunction-associated steatotic liver disease (MASLD), is currently one of the most common chronic liver diseases in the general population [1,2]. Its prevalence continues to rise, particularly in the context of the global epidemic of obesity, insulin resistance, and metabolic syndrome. Although MASLD has long been considered a metabolically driven liver disease, accumulating evidence suggests that hormonal factors are associated with its presence and metabolic profile [2,3,4].
Sex hormone-binding globulin (SHBG) is a glycoprotein that binds sex hormones, regulates their bioavailability, and has been widely studied as a marker of metabolic health [5,6]. Lower SHBG concentrations have consistently been linked to insulin resistance, type 2 diabetes, and cardiovascular diseases. Several observational studies have also reported associations between lower SHBG levels and the presence of fatty liver detected by imaging methods [7,8,9,10,11,12].
In our previous study, conducted exclusively in a male population, we demonstrated a significant association between lower SHBG concentrations and MASLD, independent of several metabolic parameters [1]. However, the absence of female participants limited the generalizability of those findings. Given the well-documented sex differences in SHBG concentrations, sex hormone levels, and metabolic characteristics, inclusion of women is necessary for a more comprehensive assessment of the relationship between SHBG and MASLD.
Therefore, the present study aimed to extend our previous research to a combined male–female cohort undergoing routine health examinations, with fatty liver identified by ultrasonography. We examined associations among SHBG, metabolic variables, and sex hormones in relation to MASLD, with particular attention to sex-specific patterns and interactions among hormonal and metabolic parameters.
2. Materials and Methods
This study included 281 participants. In the MASLD group, 98 men and 54 women were diagnosed with metabolic dysfunction-associated steatotic liver disease based on qualitative abdominal ultrasonography, with ages ranging from 29 to 73 years. The control group consisted of 74 men and 55 women without fatty liver on ultrasonography, aged 25 to 64 years.
Inclusion criteria for the MASLD group were age 29–73 years, elevated body mass index (BMI), and ultrasound-confirmed fatty liver. Inclusion criteria for the control group were age 25–64 years and the absence of fatty liver on ultrasound.
Exclusion criteria included ongoing treatment for malignant diseases and a diagnosis of type 2 diabetes. Alcohol consumption and physical activity were assessed anamnestically; participants reported moderate alcohol intake and low levels of physical activity. As these characteristics did not differ substantially between groups, they were not presented in tabular form. All participants had normal fasting glucose values, and individuals with diabetes were excluded to minimise potential metabolic confounding.
Ultrasound examinations were performed using a Siemens Acuson Sequoia ultrasound system. MASLD was diagnosed qualitatively based on increased liver echogenicity, without specific grading of steatosis severity, as standardised ultrasound criteria for precise classification are not established. Patients with MASLD underwent abdominal ultrasound with an extended protocol due to increased waist circumference, while healthy controls underwent standard abdominal ultrasound. For a more detailed assessment of fatty liver, future studies could incorporate elastography or FibroScan.
Blood samples were collected to measure biochemical, hormonal, and metabolic parameters, including estradiol, testosterone, and sex hormone-binding globulin (SHBG). Estradiol and testosterone were assessed at a single time point, and their temporal variability was not addressed in this study.
Enrollment for the study occurred between January 2024 and August 2025. The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethical Board of Medikol Polyclinic on 28 October 2025 (approval number 01.01.024 26/22-13). Informed consent was obtained from all participants before their inclusion in the study.
3. Results
3.1. Statistical Analysis
To investigate the role of SHBG (sex hormone-binding globulin) in MASLD and to identify determinants of MASLD (sex hormone-binding globulin), a series of complementary statistical approaches was applied. First, descriptive statistics were used to summarise the distribution of clinical, biochemical, and hormonal variables in the study population, providing an overview of central tendencies and variability and establishing baseline characteristics of participants with and without fatty liver. A t-test was then performed among women to evaluate whether hormonal or metabolic parameters differed significantly between affected and unaffected individuals, and to allow comparison with results from the corresponding analysis previously conducted in men.
Subsequently, two general linear models (GLMs), a complete and a stepwise model, were applied to assess associations between continuous variables and SHBG as the outcome measure. These models allowed adjustment for potential confounding factors and enabled the formal testing of interaction effects, which were further illustrated using interaction plots [13,14]. Logistic regression analyses were then performed to model the probability of fatty liver as a binary outcome. Univariate and bivariate models were used to evaluate the independent effects of individual factors and to explore specific interactions. Finally, a multivariate logistic regression model was constructed to jointly examine metabolic and hormonal factors in relation to MASLD, allowing assessment of their combined associations with the presence of fatty liver [15,16]. This multivariate modelling strategy was undertaken primarily for exploratory and explanatory purposes, to characterise patterns of association, rather than to develop a predictive model intended for clinical application.
Statistical analyses were performed using SAS software, version 9.4 (SAS Institute Inc., Cary, NC, USA).
3.1.1. Descriptive Characteristics of the Study Population
Univariate summaries of numeric variables, stratified by gender (men/women) and MASLD status (healthy vs. fatty liver), are presented in Table 1. Descriptive statistics summarise central tendency and variability and inform subsequent modelling; no inferential comparisons are included at this stage. For each stratum, Table 1 shows the number of observations (N), the mean (SD), the median, and the range (minimum and maximum values). Overall, participants with fatty liver exhibited higher central values of liver enzymes (ALT, AST, GGT), adiposity markers (BMI, waist circumference, weight), fasting insulin and HOMA2, triglycerides, and CRP, along with lower HDL, in both men and women. Total cholesterol and LDL levels showed less consistent differences across groups.
Fasting glucose medians were generally similar between groups, although upper ranges were wider among participants with fatty liver. SHBG levels were lower in the fatty liver groups for both men and women. In men, total testosterone was lower among those with fatty liver, while in women, free testosterone tended to be higher in the fatty liver group. Estradiol distributions were similar between groups in men, whereas in women, estradiol was markedly lower in the fatty liver group and showed a right-skewed distribution, particularly among healthy women. Age differed between the female groups (mean 44.0 vs. 53.3 years for healthy and fatty liver groups, respectively), which may partially explain the observed estradiol differences.
However, data on menopausal status and hormone therapy were not available, which should be considered when interpreting these descriptive summaries. Distributions of estradiol (pmol/L), insulin, triglycerides, CRP, and GGT were right-skewed, as indicated by larger SDs, differences between means and medians, and coefficients of skewness. Creatinine values were within expected gender-specific ranges.
3.1.2. Comparison of Individuals Diagnosed with Fatty Liver to Healthy Participants About SHBG, Separately by Gender
In our earlier article [1], t-test results indicated a statistically significant difference in SHBG levels between men with fatty liver and healthy participants. We now apply the same t-test framework to the female cohort to evaluate whether analogous differences are present in women.
The table below (Table 2) displays the mean SHBG difference (along with the respective 95% Confidence Interval (CI) limits) between MASLD groups for women (−22.75, 95% CI −15.21, −30.29) and compares it to the previously reported estimates (−9.51, 95% CI −5.23, −13.79) for male participants (Table 3). Group differences were tested using the Welch–Satterthwaite t-test (Table 4 and Table 5 for women and men, respectively).
Among women, mean SHBG concentrations were markedly lower in participants with fatty liver than in the healthy ones (44.01, 95% CI 38.59, 49.43 vs. 66.76, 95% CI 61.40, 72.13), yielding a mean difference of −22.75 (with 95% CI limits of −15.21 to −30.29) and a p-value of less than 0.0001. In men, the same pattern was observed but with smaller absolute values: fatty liver 29.14 (95% CI 26.88, 31.41) vs. healthy 38.65 (95% CI 34.99, 42.32), for a mean difference of −9.51 (95% CI −5.23, −13.79), also statistically significant. Comparing genders, women have higher SHBG than men within each of the MASLD strata, and the difference in SHBG between MASLD groups in women (−22.75) is roughly 2.4-fold to that in men (−9.51); notably, the 95% confidence intervals for these gender-specific differences do not overlap (women −15.21, −30.29; men −5.23, −13.79), indicating a clearly stronger contrast in women.
The distributions and between-group contrasts are visualised in the boxplots below (Figure 1), which highlight medians, interquartile ranges, and potential outliers, allowing a side-by-side appraisal of SHBG patterns for women (F) versus men (M).
3.1.3. General Linear Model Analysis for SHBG
SHBG was analysed as the outcome in a combined male–female cohort using a general linear model (GLM). Two strategies were applied: (i) a complete model including all candidate variables without automated selection, and (ii) a stepwise selection approach (using the SAS GLMSELECT procedure with the Schwarz Bayesian Information Criterion (SBC) as the stopping criterion). To better meet model assumptions, variables with right-skewed distributions (AST, CRP, GGT, glucose, triglycerides, HOMA2, and estradiol) were log-transformed before the analysis [17].
Results for the full model are displayed in Table 6.
As shown in Table 6, the MASLD Indicator (fatty liver) was associated with lower SHBG concentrations (p = 0.0024), indicating that individuals with fatty liver had lower SHBG than healthy controls, after adjustment for all other variables in the model. Gender was a strong determinant, with women exhibiting markedly higher levels than men (p = 0.0003). Among metabolic parameters, total cholesterol was positively associated with SHBG (p = 0.0025), while log-transformed triglycerides showed a negative relationship (p = 0.0202), highlighting opposing lipid effects.
Hormonal variables were also relevant. Log-transformed estradiol was positively associated with SHBG (p = 0.0076), and a significant log (Estradiol) × gender interaction (p = 0.0311) indicated that the strength of this association differed by gender. Specifically, increases in estradiol were associated with greater increases in SHBG in men than in women, suggesting gender-specific slopes.
Other variables, including BMI, age, BMI × gender, BMI × age, log (HOMA2), HDL cholesterol, creatinine, log (AST), log (CRP), log (GGT), log (Glucose), and free testosterone, were not significantly associated with SHBG after mutual adjustment (all p > 0.05). Although age was included as a covariate in general linear models and thus adjusted for, this adjustment does not fully account for unmeasured reproductive or hormonal factors influencing estradiol levels, leaving the possibility of residual confounding.
These findings indicate that fatty liver, gender, cholesterol, triglycerides, and estradiol (with a gender interaction) are the principal independent determinants of SHBG levels. In contrast, other metabolic and biochemical variables do not contribute significantly to the whole model. Because tests of individual covariates are conditional on the remaining terms in the model, their statistical significance in the complete model may be affected by substantial correlations among the included measures.
Therefore, stepwise selection of model covariates was performed using the Schwarz Bayesian Information Criterion (SBC) as the stopping criterion.
The chosen model results are presented in Table 7, below (General Linear Model—Parameter Estimates for the Chosen Model). After adjustment for all covariates, SHBG levels differed by gender (p = 0.0018), with higher levels in women than men (by 80 nmol/L on average, regardless of the fatty liver status). MASLD Indicator (fatty liver) was associated with lower SHBG (by 10 nmol/L) compared with healthy status (p < 0.0001), and this reduction was more pronounced in women (gender × MASLD Indicator p = 0.0462). (On average, this reduction in SHBG was by 10 nmol/L higher in women than in men.) The association between estradiol (log-transformed) and SHBG also varied by gender, being weaker among women than men (gender × log (Estradiol) p = 0.0147). Furthermore, higher estradiol (log-transformed) was associated with higher SHBG (p = 0.0009). Overall, older age and higher total cholesterol were associated with higher SHBG (p = 0.0058 and p = 0.0003, respectively), whereas higher triglycerides (log-transformed) were associated with lower SHBG (p = 0.0012).
3.1.4. Association of Metabolic and Hormonal Factors with the MASLD Status Using Logistic Regression
To investigate the metabolic and hormonal determinants of MASLD status, logistic regression models of increasing complexity were applied: from univariate to bivariate models incorporating key interactions, and culminating in a multivariate model. This sequential approach allowed us first to assess the independent associations of individual measures with the MASLD indicator, then examine potential gender-specific hormonal effects, and finally jointly evaluate metabolic and endocrine factors within a comprehensive modelling framework. Further details regarding variable selection approaches are provided in the Supplementary Materials.
In the univariate analyses (Table 8 (1. Univariate) and Figure S1), body mass index (BMI), cholesterol, and SHBG each showed significant associations with the MASLD status. Specifically, every two-unit increase in BMI was associated with an approximate fourfold increase in the odds of fatty liver (OR = 4.070, 95% CI: 3.021–5.804). These results should be interpreted as statistical associations rather than causal effects, consistent with the study’s cross-sectional design.
The bivariate logistic regression model, including an interaction between gender and log-transformed estradiol (Table 8 (2. Bivariate); Figure 2), demonstrated a sex-specific association pattern. Among women, a 0.693-unit increase in log-transformed estradiol concentration (corresponding to a doubling of estradiol levels) was associated with lower odds of the outcome (OR = 0.152, 95% CI: 0.070–0.273). In men, estradiol concentration was not significantly associated with the outcome, with point estimates in the opposite direction (OR = 1.513, 95% CI: 0.697–3.340). These estimates reflect cross-sectional associations and should not be interpreted as evidence of causality. Information on menopausal status, hormone replacement therapy, and oral contraceptive use was not available.
Figure 2 presents the fitted associations between log-transformed estradiol and the outcome, stratified by gender. The crossing of the curves reflects the inclusion of a gender-by-estradiol interaction term. It is shown to visualise the modelled associations rather than to imply a biologically meaningful threshold, directional effect, or individual-level risk.
The final multivariable logistic regression model results are shown in Table 8 (3. Multivariate) and Figure 3. Body mass index (BMI; per 2-unit increase) showed the strongest association with MASLD (OR = 5.508, 95% CI: 3.574–9.545), followed by total cholesterol (OR = 1.864, 95% CI: 1.174–3.104). Sex hormone-binding globulin (SHBG; per 10 nmol/L increase) was associated with lower odds of MASLD (OR = 0.521, 95% CI: 0.331–0.764).
Estradiol showed a sex-specific association pattern. In women, higher estradiol concentrations were associated with lower odds of MASLD (OR = 0.113, 95% CI: 0.031–0.265 for a two-fold increase), whereas no statistically significant association was observed in men (OR = 1.612, 95% CI: 0.354–7.656). These estimates represent cross-sectional associations and should not be interpreted as evidence of causality.
The multivariable model was developed for exploratory, hypothesis-generating purposes rather than for clinical prediction. Accordingly, it should not be interpreted as a clinically applicable predictive model. The use of multivariable analysis reflects the joint evaluation of correlated metabolic and hormonal factors and does not imply definitive predictive accuracy.
3.1.5. Association of BMI, Blood Pressure, and Gender with MASLD/Fatty Liver Indicator
In this expanded cohort, including both men and women, the larger sample size provided greater statistical power to detect associations between blood pressure and MASLD Indicator (Table 9). In the univariate analyses, BMI, diastolic blood pressure, and systolic blood pressure were all strongly associated with MASLD Indicator. BMI showed the most robust effect (Wald χ^2^ = 71.7986, p < 0.0001), followed by systolic blood pressure (Wald χ^2^ = 31.8567, p < 0.0001) and diastolic blood pressure (Wald χ^2^ = 23.2789, p < 0.0001). Gender was not significantly associated with MASLD Indicator when examined univariately (Wald χ^2^ = 1.4822, p = 0.2234).
The bivariate models further clarified these associations. When BMI and diastolic blood pressure were entered together, BMI remained highly significant (Wald χ^2^ = 67.9669, p < 0.0001). In contrast, diastolic blood pressure lost significance (Wald χ^2^ = 3.5003, p = 0.0614), due to a strong correlation among BMI, diastolic and systolic blood pressure. In the model including BMI and systolic blood pressure, BMI retained a strong association (Wald χ^2^ = 65.4434, p < 0.0001), while systolic blood pressure showed a modest but significant effect (Wald χ^2^ = 5.4772, p = 0.0193).
In the final multivariate model including BMI, gender, and diastolic and systolic blood pressure, BMI remained the variable most strongly associated with fatty liver (Wald χ^2^ = 64.4213, p < 0.0001). Neither diastolic blood pressure (Wald χ^2^ = 0.9434, p = 0.3314) nor systolic blood pressure (Wald χ^2^ = 2.8172, p = 0.0933) remained significant after mutual adjustment, and gender was not associated with MASLD Indicator (Wald χ^2^ = 0.0066, p = 0.9351).
These findings demonstrate that, in the larger mixed-gender cohort, BMI showed the strongest and most consistent association with fatty liver. In contrast, diastolic and systolic blood pressure and gender were not significantly associated after mutual adjustment.
4. Discussion
In this cross-sectional study, we investigated the associations of SHBG, estradiol, and metabolic factors with MASLD in a combined male and female cohort.
Consistent with previous findings in men, SHBG levels were significantly lower in individuals with fatty liver. Extending the analysis to women revealed even stronger contrasts, with women showing a roughly 2.4-fold greater difference in SHBG levels between MASLD patients and healthy participants than men. These findings highlight the importance of considering sex-specific hormonal and metabolic influences in MASLD.
Estradiol demonstrated a potentially protective association in women, whereas no significant relationship was observed in men. This supports the concept that sex hormones may modulate MASLD pathophysiology in a sex-specific manner, particularly in women. Our results align with previous studies reporting associations between lower SHBG concentrations, altered sex hormone profiles, metabolic dysregulation, and hepatic steatosis.
A notable limitation of this study is the significant age difference observed between female MASLD patients and female controls. The MASLD group was, on average, nearly a decade older, suggesting a higher proportion of postmenopausal women. The menopausal transition is associated with substantial changes in oestrogen levels, SHBG concentrations, and metabolic risk profiles, all of which may influence SHBG levels and MASLD development. As direct data on menopausal status were unavailable, this potential confounding factor could not be fully adjusted for, and should be carefully considered when interpreting sex-specific associations in our results.
Given the cross-sectional design, no causal or mechanistic conclusions can be drawn, and the observed associations do not allow inference regarding directionality. In particular, alterations in hepatic metabolic function associated with MASLD may influence SHBG synthesis, rather than SHBG changes contributing causally to disease development.
BMI emerged as the most robust predictor of MASLD, independent of sex and blood pressure. While systolic and diastolic blood pressure were initially associated with MASLD, these associations were attenuated after adjustment for BMI, suggesting that adiposity mediates much of the cardiovascular contribution to fatty liver risk. Lipid parameters, including cholesterol and triglycerides, also influenced SHBG levels and MASLD risk, underscoring a complex interplay between lipid metabolism, hormonal status, and hepatic fat accumulation.
The strong predictive performance of the multivariate stepwise logistic regression model, incorporating metabolic and hormonal variables, demonstrates the potential value of integrative approaches for MASLD risk assessment. However, the absence of an independent validation cohort warrants caution, and external validation in separate populations is needed to confirm generalizability.
These findings have several potential clinical implications. SHBG and estradiol may serve as adjunct biomarkers for identifying individuals at higher risk of MASLD, particularly women, whereas BMI remains the primary modifiable risk factor. Interventions targeting weight management and metabolic health are likely to represent the most effective strategies for MASLD prevention.
Future research should aim to validate these associations in larger, multi-ethnic cohorts, assess longitudinal predictive value, and further explore mechanistic pathways linking sex hormones, SHBG, and hepatic lipid accumulation. Such studies could contribute to individualised risk stratification and inform targeted therapeutic approaches.
5. Conclusions
Our results confirm that lower SHBG levels are associated with MASLD in both men and women, with more potent effects in women. Estradiol shows a sex-specific association in women, whereas BMI remains the dominant metabolic determinant of fatty liver. Integrating metabolic and hormonal biomarkers may help in MASLD risk assessment and inform individualised prevention strategies. Future studies should focus on validation, mechanistic insights, and the development of gender-specific interventions to reduce the risk of fatty liver.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Duric L.F. BelčićV. Korbar A.O. ĆurkovićS. Vujicic B. Gulin T. Muslim J. Gulin M. GrgurevićM. Cuti E.C. The Role of SHBG as a Marker in Male Patients with Metabolic-Associated Fatty Liver Disease: Insights into Metabolic and Hormonal Status J. Clin. Med.202413771710.3390/jcm 1324771739768643 PMC 11677371 · doi ↗ · pubmed ↗
- 2Portincasa P. Khalil M. Mahdi L. Perniola V. Idone V. Graziani A. Baffy G. Di Ciaula A. Metabolic Dysfunction-Associated Steatotic Liver Disease: From Pathogenesis to Current Therapeutic Options Int. J. Mol. Sci.202425564010.3390/ijms 2511564038891828 PMC 11172019 · doi ↗ · pubmed ↗
- 3NCD Risk Factor Collaboration Rising rural body-mass index is the main driver of the global obesity epidemic in adults Nature 201956926026410.1038/s 41586-019-1171-x 31068725 PMC 6784868 · doi ↗ · pubmed ↗
- 4Vecchie A. Dallegri F. Carbone F. Bonaventura A. Liberale L. Portincasa P. Fruhbeck G. Montecucco F. Obesity phenotypes and their paradoxical association with cardiovascular diseases Eur. J. Intern. Med.20184861710.1016/j.ejim.2017.10.02029100895 · doi ↗ · pubmed ↗
- 5Dubey P. Singh V. Venishetty N. Trivedi M. Reddy S.Y. Lakshmanaswamy R. Dwivedi A.K. Associations of sex hormone ratios with metabolic syndrome and inflammation in US adult men and women Front. Endocrinol.202415138460310.3389/fendo.2024.1384603 PMC 1103996438660513 · doi ↗ · pubmed ↗
- 6Hammond G.L. Wu T.-S. Simard M. Evolving utility of sex hormone-binding globulin measurements in clinical medicine Curr. Opin. Endocrinol. Diabetes Obes.20121918318910.1097/MED.0b 013e 328353732 f 22531107 · doi ↗ · pubmed ↗
- 7Goldštajn M.Š. Toljan K. GrgićF. JurkovićI. Baldani D.P. Sex Hormone Binding Globulin (SHBG) as a Marker of Clinical Disorders Coll. Antropol.20164021121829139641 · pubmed ↗
- 8Qu X. Donnelly R. Sex Hormone-Binding Globulin (SHBG) as an Early Biomarker and Therapeutic Target in Polycystic Ovary Syndrome Int. J. Mol. Sci.202021819110.3390/ijms 2121819133139661 PMC 7663738 · doi ↗ · pubmed ↗