Polygenic Collagen Variants and Their Association With Ligament Injury Patterns in Patients With Knee Ligament Injuries
Jurgen Frese-Arroyo, Santiago De la Garza-Castro, José F Vílchez-Cavazos, Victor M Peña-Martínez, Jorge Lara-Arias

TL;DR
This study explores how multiple collagen-related genetic variants may influence the risk and patterns of knee ligament injuries, particularly ACL tears.
Contribution
The study introduces a polygenic score approach to assess genetic susceptibility to knee ligament injuries in a clinical population.
Findings
Patients with multiligament injuries had a higher polygenic burden compared to those with isolated ACL injuries.
Non-contact injury mechanisms were associated with a higher polygenic burden.
Individual genetic variants alone did not show significant associations with injury severity.
Abstract
Knee ligament injuries, particularly anterior cruciate ligament (ACL) tears, represent a major cause of functional limitation in physically active individuals. While biomechanical and environmental factors are well-established contributors, increasing evidence suggests that genetic variability in collagen-related genes may influence individual susceptibility to ligament injury. Most previous studies, however, have focused on elite athletic populations, limiting their applicability to routine clinical settings. A prospective cross-sectional study was conducted in 94 adult patients with clinically and radiologically confirmed knee ligament injuries. The study was conducted at the University Hospital ‘Dr. José Eleuterio González’ (Hospital Universitario “Dr. José Eleuterio González”), Universidad Autónoma de Nuevo León (UANL), Monterrey, Mexico, a tertiary care university hospital. All…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
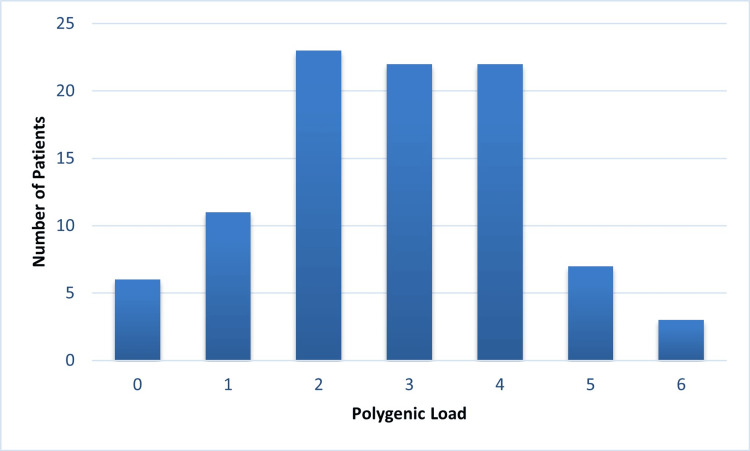 Figure 1
Figure 1| Variable | Category | Result |
| Total participants | Overall | 94 |
| Age (years) | Mean ± SD | 28.4 ± 11.1 |
| Range | 18-68 | |
| Sex | Male | 64 (68.1%) |
| Female | 30 (31.9%) | |
| Activity at the time of injury | Sports | 78 (82.9%) |
| Fall | 9 (9.6%) | |
| Accident | 7 (7.4%) | |
| Injury mechanism | Non-contact | 81 (86.2%) |
| Contact | 13 (13.8%) | |
| ACL rupture | Present | 94 (100%) |
| ACL tear grade | Complete | 65 (69.3%) |
| Partial | 29 (30.7%) | |
| Injury pattern | Isolated ACL injury | 77 (81.9%) |
| Multiligament injury | 17 (18.1%) |
| Gene (polymorphism) | Genotype | n (%) | Interpretation |
| COL1 A1 (G>T) | GG | 35 (37.2%) | Most common genotype |
| GT | 44 (46.8%) | Heterozygous; intermediate genotype / risk trend reported | |
| TT | 15 (16.0%) | Less frequent; increased risk described in athletic cohorts | |
| COL1 A2 (G>C) | GG | 46 (48.9%) | Most common genotype |
| GC | 34 (36.2%) | Heterozygous; intermediate genotype / associated with overload-related injuries | |
| CC | 14 (14.9%) | Least frequent; associated with connective tissue fragility and multiligament injuries | |
| COL3 A1 (G>A) | GG | 30 (31.9%) | Most common genotype |
| GA | 31 (33.0%) | Heterozygous; intermediate genotype | |
| AA | 33 (35.1%) | Risk genotype described in sports-related ligament injuries |
| Type of injury | n | Polygenic risk score (mean ± SD) | p |
| Isolated ACL injury | 77 (81.9%) | 2.61 ± 1.39 | 0.0066 |
| Multiligamentary injury | 17 (18.1%) | 3.65 ± 1.41 |
| Injury mechanism | n | Polygenic risk score (mean ± SD) | p |
| Contact | 13 (13.8%) | 1.83 ± 1.19 | 0.00023 |
| Non-contact | 81 (86.2% | 2.97 ± 1.33 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOsteoarthritis Treatment and Mechanisms · Tendon Structure and Treatment · Knee injuries and reconstruction techniques
Introduction
Knee ligament injuries are among the most frequent musculoskeletal conditions in physically active populations and represent a substantial source of morbidity, functional limitation, and healthcare utilization. Anterior cruciate ligament (ACL) rupture is strongly associated with sports participation and typically affects young, active individuals, often requiring prolonged rehabilitation and, in many cases, resulting in persistent joint instability or early degenerative joint changes [1-3].
Epidemiological evidence has consistently shown that a considerable proportion of ACL injuries occur without direct contact, most often during rapid deceleration, pivoting, or landing maneuvers [4,5]. Although biomechanical factors such as neuromuscular control, lower-limb alignment, and training load play a central role, these mechanisms alone do not fully explain why individuals exposed to comparable athletic demands experience markedly different injury outcomes.
From a tissue perspective, ligaments are composed predominantly of type I and type III collagen, which together confer tensile strength, elasticity, and resistance to mechanical stress [6]. Disruptions in collagen synthesis, fibrillar organization, or the relative proportion of these collagen types may compromise ligament integrity and increase the likelihood of failure under physiological loads [6,7]. In this context, genetic polymorphisms in collagen-encoding genes have been proposed as contributors to interindividual variability in ligament structure and injury susceptibility [8-11].
Prior studies have reported associations between variants in collagen type I alpha 1 chain (COL1A1), collagen type I alpha 2 chain (COL1A2), and collagen type III alpha 1 chain (COL3A1) and ligament or tendon injuries, particularly in athletic cohorts [8-11]. Variants within COL3A1 have been linked to changes in collagen elasticity, whereas polymorphisms in COL1A1 and COL1A2 may influence fibrillar organization and tensile properties [8-11]. However, findings across studies have been heterogeneous, and many investigations have assessed single polymorphisms in isolation, which may underestimate the cumulative genetic contribution to ligament vulnerability [8-11].
Increasingly, research in musculoskeletal genetics supports a polygenic model in which multiple low-impact variants collectively contribute to tissue resilience and injury susceptibility [12,13]. This framework may be especially relevant for ligament injuries, where structural failure often reflects a complex interaction of biological, mechanical, and environmental factors rather than a single dominant cause.
Accordingly, the present study aimed to evaluate the relationship between polymorphisms in COL1A1, COL1A2, and COL3A1 and the clinical presentation of knee ligament injuries in a heterogeneous clinical population. In addition, we explored whether a cumulative polygenic burden is associated with injury complexity and mechanism, with the goal of generating clinically meaningful insights applicable to routine orthopedic practice.
Materials and methods
Ethical approval
The study was conducted at the University Hospital ‘Dr. José Eleuterio González’ (Hospital Universitario “Dr. José Eleuterio González”), Universidad Autónoma de Nuevo León (UANL), Monterrey, Mexico, a tertiary care university hospital. This study was reviewed and approved by the Research Ethics Committee of the institution (approval number: OR24-00011). All procedures were conducted in accordance with institutional and national ethical standards and the Declaration of Helsinki.
Study design and population
A prospective, cross-sectional study was conducted in adults with knee ligament injuries evaluated at a tertiary care university hospital, reflecting routine orthopedic and trauma practice in a clinically heterogeneous population. Ninety-four patients were enrolled after meeting eligibility criteria and providing written informed consent. All participants had a clinically and/or imaging-confirmed ligament injury involving the ACL, posterior cruciate ligament (PCL), medial collateral ligament (MCL), lateral collateral ligament (LCL), or combinations of these structures.
Eligibility criteria
Patients aged ≥18 years of either sex with a confirmed knee ligament injury were eligible. Exclusion criteria were high-energy trauma (e.g., motor vehicle accidents or falls from height), known hereditary connective tissue disorders, prior knee reconstructive surgery unrelated to the index injury, significant angular deformity, or any condition that could compromise reliable data collection or buccal DNA sampling.
Clinical data collection
Clinical and demographic data were obtained using a structured questionnaire administered after written informed consent (see Appendix). The questionnaire was developed by the authors (orthopedic clinicians) for this study, based on routine clinical assessment and commonly reported variables in knee ligament injury practice; it was not adapted from a previously published instrument. Items captured age, sex, level, and type of physical activity, injury mechanism (contact vs non-contact), sport or activity at the time of injury, ligament(s) involved, injury severity, treatment received, and history of prior ligament injuries. These data were used to describe the cohort and to explore associations between clinical variables and genetic findings.
DNA sampling and extraction
Genomic DNA was collected using buccal swabs from the inner cheek. Samples were processed with a semi-automated magnetic bead-based extraction system (Zybio® EXM3000, Zybio Inc., Chongqing, China) according to the manufacturer’s instructions. DNA concentration and purity were assessed spectrophotometrically, and extracts were stored at −20 °C until analysis.
Genotyping by real-time PCR
Genotyping of rs1107946 (COL1A1), rs42524 (COL1A2), and rs1800255 (COL3A1) was performed using real-time polymerase chain reaction (PCR) with allele-specific primers and probes, following previously validated protocols [12,14,15]. Amplification was carried out on a QuantStudio™ 5 Real-Time PCR System (Thermo Fisher Scientific, USA) using a commercial genotyping master mix. Primer sequences were as follows: COL1A1 (rs1107946), forward 5′-CCTACTGTGGGTCAGTTCCAAGAGA-3′ and reverse 5′-CCCCTCCCTAATAGGCGACAGGGT-3′; COL1A2 (rs42524), forward 5′-AGGTGGAAAAGGTGAACAGGGTCCC-3′ and reverse 5′-CTGGTCCTCCAGGCTTCCAGGTAAG-3′; and COL3A1 (rs1800255), forward 5′-TGGTGAACGTGGACCTCCTGGATTG-3′ and reverse 5′-GGTGAATGGAATGCTGTGGAGTTACCTTT-3′. Reactions were performed in a final volume of 20 µL containing master mix, forward and reverse primers, allele-specific probe, approximately 20 ng of genomic DNA per reaction, and nuclease-free water. Cycling conditions were 95 °C for 10 minutes, followed by 40 cycles of 95 °C for 15 seconds and 60 °C for 60 seconds. All samples were analyzed in duplicate, and positive and negative controls were included in each run. Allelic discrimination was performed using the instrument software, and results were exported for statistical analysis.
Polygenic risk assessment
Genotypes were categorized as homozygous wild-type, heterozygous, or homozygous variant. A polygenic risk score was calculated by assigning numerical values according to the number of risk alleles per polymorphism and summing across COL1A1, COL1A2, and COL3A1, allowing assessment of combined genetic burden rather than isolated variants. Higher scores reflected greater cumulative genetic risk.
Statistical analysis
Analyses were performed using IBM SPSS Statistics version 25.0 (released 017, IBM Corp., Armonk, NY, USA). Continuous variables are presented as mean ± standard deviation or median (interquartile range), as appropriate. Categorical variables are reported as frequencies and percentages. Comparative analyses assessed associations between genetic findings (including polygenic score) and clinical injury characteristics. A two-sided p-value < 0.05 was considered statistically significant.
Results
Study population characteristics
A total of 94 patients with confirmed knee ligament injuries were included in the analysis. The mean age was 28.4 years, with a predominance of male participants. Most injuries occurred during physical or sports-related activities, reflecting an active cohort. Non-contact mechanisms were more frequent than contact-related injuries (Table 1).
Overall, the cohort profile aligns with prior reports in physically active populations and is compatible with genotype distributions typically observed in large population-based genomic reference datasets [16].
Distribution of genetic variants
Genotyping showed a predominance of heterozygous genotypes across the three evaluated loci (COL1A1, COL1A2, and COL3A1), including variants previously described as risk-associated. The most frequent genotypes corresponded to reference alleles commonly reported in the general population, whereas lower-frequency genotypes included heterozygous and homozygous variant profiles.
When each polymorphism was assessed individually, no single variant showed a clear independent association with injury severity or ligament involvement. Nevertheless, the observed genotype distribution supported subsequent analyses based on a combined polygenic approach (Table 2).
Table 2: Distribution of collagen gene polymorphisms in the study populationData are presented as mean ± standard deviation. COL1A1: collagen type I alpha 1 chain; COL1A2: collagen type I alpha 2 chain; COL3A1: collagen type III alpha 1 chain; ACL: anterior cruciate ligament; n: number of participants; SD: standard deviation; p: p-value. Statistical comparison performed using Student’s t-test. A p-value < 0.05 was considered statistically significant.
Polygenic risk distribution
The cumulative polygenic risk score, defined as the total number of risk alleles across COL1A1, COL1A2, and COL3A1, showed that most participants clustered within intermediate values, most commonly between two and four risk alleles. This pattern reflects adequate genetic variability within the cohort and avoids overrepresentation of extremely low- or high-burden profiles.
This balanced distribution enabled meaningful comparisons across clinical subgroups and injury characteristics, supporting subsequent analyses examining the relationship between genetic burden, injury type, and injury mechanism.
Figure 1 illustrates the distribution of the cumulative polygenic risk score in the study population, expressed as the total number of risk alleles identified across the three collagen-related genes.
Distribution of polygenic load in the study population.The histogram shows the number of patients according to the cumulative number of risk alleles identified across the COL1A1, COL1A2, and COL3A1 genes. Most participants clustered within intermediate polygenic load values (2–4 risk alleles), indicating adequate genetic variability within the cohort.
Polygenic risk and type of ligament injury
When polygenic risk was compared by injury pattern, patients with multiligament involvement exhibited a higher cumulative number of risk alleles than those with isolated ACL injuries. Statistical testing demonstrated a significant difference between groups.
This finding suggests that the accumulation of collagen-related risk variants may be associated with greater susceptibility to complex ligament injury patterns, rather than isolated ACL disruption. In practical terms, individuals with injuries affecting more than one ligament tended to show a higher genetic burden involving collagen type I and III, which may translate into reduced structural stability of ligament tissue under functional loading.
Table 3 summarizes the comparison of cumulative polygenic risk scores between patients with isolated ACL injuries and those with multiligament injuries (analysis performed on participants with available polygenic-score data).
Polygenic risk and mechanism of injury
Comparison by injury mechanism showed a clear pattern: patients who sustained ligament injuries through non-contact mechanisms had, on average, higher cumulative polygenic risk scores than those whose injuries occurred through direct contact.
This pattern supports the concept that collagen-related genetic variability may contribute to ligament failure under routine biomechanical demands, particularly during sports movements that involve deceleration, pivoting, or abrupt changes in direction. By contrast, contact-related injuries appeared to be less dependent on baseline tissue susceptibility and more strongly driven by external traumatic forces.
To quantify this association, cumulative polygenic risk scores were compared between contact and non-contact injury mechanisms. As shown in Table 4, the non-contact group demonstrated a significantly higher polygenic burden, reinforcing the hypothesis that genetic predisposition may be more influential in low-energy injury scenarios.
Discussion
The present study evaluated the potential association between polymorphisms in extracellular matrix-related genes (COL1A1, COL1A2, and COL3A1) and knee ligament injuries in adult patients with a history of recreational or sports-related physical activity. In contrast to prior investigations focused mainly on elite or professional athletes, a key strength of this work is the inclusion of a heterogeneous cohort that more closely reflects routine orthopedic and trauma practice. This strengthens the external validity of the findings for everyday clinical settings beyond highly selected athletic cohorts.
From a biological standpoint, evidence from large-scale population genomics suggests that the clinical relevance of many variants lies less in isolated effects and more in their cumulative contribution to tissue integrity and functional resilience. Analyses of mutational constraint across diverse human populations support the concept that multiple low-impact variants may collectively influence susceptibility to complex phenotypes, particularly in structurally dependent tissues such as connective tissue [17].
In our cohort, most injuries occurred during recreational sports and were associated with non-contact mechanisms. Sudden deceleration, pivoting, and landing maneuvers have been repeatedly identified as predominant injury mechanisms, even in the absence of direct trauma [18,19]. This observation supports the concept that, beyond mechanical factors, intrinsic biological determinants may influence how ligament tissue responds to functional loading under everyday athletic demands.
Regarding genetic findings, the distribution of COL3A1 rs1800255 (G>A) genotypes was comparable to that reported in international literature. Stepien-Słodkowska et al. described an overrepresentation of the AA genotype among Polish skiers with rupture, suggesting a relevant role of type III collagen in ligament elasticity and resistance [20]. Similarly, Lince et al. reported a higher frequency of risk-associated variants in South African athletes with ligament injuries, reinforcing the notion that alterations in collagen composition may predispose individuals to injury under repetitive or submaximal loading conditions [14].
Unlike studies restricted to highly selected athletic cohorts, the present investigation included individuals with varying levels of physical activity, allowing assessment of the clinical expression of these polymorphisms in a more generalizable context. The findings suggest that collagen-related genetic variability may contribute to ligament injury susceptibility beyond elite sport settings and may also be relevant in recreationally active individuals.
For COL1A1 and COL1A2, our results were consistent with prior work reporting modest but reproducible associations between type I collagen variants and injury risk. Studies in European and South American athletic populations have suggested that COL1A1 (rs1107946) and COL1A2 (rs42524) variants may alter fibrillar organization and tensile properties, potentially increasing susceptibility to injury from repetitive stress or overload [12,21]. In the present study, although individual polymorphisms did not show strong independent associations, combined analysis suggested a tendency toward higher genetic burden in patients with more complex or combined ligament injuries.
One of the most relevant findings was the utility of a composite polygenic risk variable integrating multiple collagen-related polymorphisms. This approach aligns with contemporary genomic research, indicating that susceptibility is unlikely to depend on a single variant and may instead reflect the cumulative interaction of multiple loci involved in connective tissue structure and remodeling [22]. In this context, the multigene association analysis by Kim et al. supports models that consider the aggregated contribution of several variants to ligament injury susceptibility [23].
Clinically, these findings are not intended to support immediate diagnostic or screening applications of genetic testing. Rather, they provide exploratory evidence that may help explain interindividual variability in ligament response under comparable mechanical loads. Prior studies on risk factors for re-injury have emphasized variables such as age, graft type, and activity level, while acknowledging an unexplained component that may have a biological basis [24,25]. In the future, integrating genetic information could contribute to more refined risk stratification models and individualized preventive strategies.
Several limitations should be acknowledged, including sample size and the absence of a non-injured control group. Nevertheless, the cross-sectional design and the integration of clinical and genetic data allow the generation of meaningful hypotheses for future research. The principal strength of this study lies in its integrative approach, linking real-world clinical information with relevant genetic variation, thereby expanding current knowledge on biological susceptibility to knee ligament injuries in a context applicable to orthopedic practice.
Conclusions
This study suggests that susceptibility to knee ligament injury is better explained by a cumulative polygenic profile than by any single collagen-gene polymorphism. While individual variants in COL1A1, COL1A2, and COL3A1 did not show strong independent effects, a higher combined genetic burden was associated with more complex injury patterns and a greater tendency toward non-contact mechanisms, consistent with the idea that subtle differences in connective tissue structure may influence how ligaments tolerate routine biomechanical loading. Overall, these findings support a multifactorial view of ligament injury risk and provide a rationale for future work exploring how genetic information might complement clinical and biomechanical assessment in prevention and patient counseling.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Effect of anterior cruciate ligament rupture on physical activity, sports participation, patient-reported health outcomes, and physical function in young female athletes Am J Sports Med Ezzat AM Brussoni M Mâsse LC Emery CA 146014694920213383082110.1177/03635465211002530 · doi ↗ · pubmed ↗
- 2Anterior cruciate ligament injury: identification of risk factors and prevention strategies Curr Sports Med Rep Acevedo RJ Rivera-Vega A Miranda G Micheo W 1861911320142481901110.1249/JSR.0000000000000053 · doi ↗ · pubmed ↗
- 3Clinical examination of anterior cruciate ligament rupture: a systematic review and meta-analysis Acta Orthop Traumatol Turc Huang W Zhang Y Yao Z Ma L 22315020162685404510.3944/AOTT.2016.14.0283 · doi ↗ · pubmed ↗
- 4Understanding and preventing noncontact anterior cruciate ligament injuries: a review of the Hunt Valley II meeting, January 2005 Am J Sports Med Griffin LY Albohm MJ Arendt EA 151215323420061690567310.1177/0363546506286866 · doi ↗ · pubmed ↗
- 5Sport-specific injury mechanisms and situational patterns of ACL injuries: a comprehensive systematic review Sports Med Sundberg A Högberg J Tosarelli F 248925275520254069016210.1007/s 40279-025-02271-w PMC 12513954 · doi ↗ · pubmed ↗
- 6Ligament cell biology: effect of mechanical loading Cell Physiol Biochem Stańczak M Biały M Hagner-Derengowska M 2522955920254033636110.33594/000000773 · doi ↗ · pubmed ↗
- 7Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies J Am Acad Orthop Surg Griffin LY Agel J Albohm MJ 141150820001087422110.5435/00124635-200005000-00001 · doi ↗ · pubmed ↗
- 8The evaluation of variants within eight collagen genes COL 1A 1, COL 1A 2, COL 3A 1, COL 5A 1, COL 11A 1, COL 15A 1, COL 22A 1, and COL 27A 1 and a risk of non-contact knee ligament rupture in elite handball players: Aa case-control study Balt J Health Phys Act Krawczak-Wojcik K Mastalerz A Bojarczuk A 172025