Analysis of Factors Affecting Postoperative Opioid Requirement in Adult Patients Undergoing Minimally Invasive Repair of Pectus Excavatum
Minju Kim, Saewon Park, Seung Keun Yoon, Wonjung Hwang

TL;DR
This study identifies factors like male sex, higher BMI, and longer surgery time that increase opioid use after pectus excavatum surgery in adults.
Contribution
The study is the first to focus on adult patients and identifies specific perioperative factors linked to opioid requirements after MIRPE.
Findings
Pain intensity peaks within the first 6 hours post-surgery and increases again between 24–48 hours.
Male sex, higher BMI, and longer operation time are independently associated with increased opioid consumption.
Multiple bar insertion correlates with higher opioid use in the first 6 hours after surgery.
Abstract
Background/Objectives: Minimally invasive repair of pectus excavatum (MIRPE) is an established surgical treatment for adult pectus excavatum (PE). Compared with pediatric patients, adults generally have a more rigid chest wall and greater costal cartilage ossification, often resulting in more severe postoperative pain. However, most previous studies have focused on pediatric patients with PE and on evaluating effective analgesic methods. This study aimed to investigate perioperative factors associated with postoperative opioid requirements and pain intensity in adult patients undergoing MIRPE. Methods: This study was a single-center retrospective study of adult PE patients who underwent MIRPE between March 2011 and January 2023. The primary outcome was total opioid consumption during the first 24 postoperative hours. Secondary outcomes included opioid and rescue analgesic use within…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
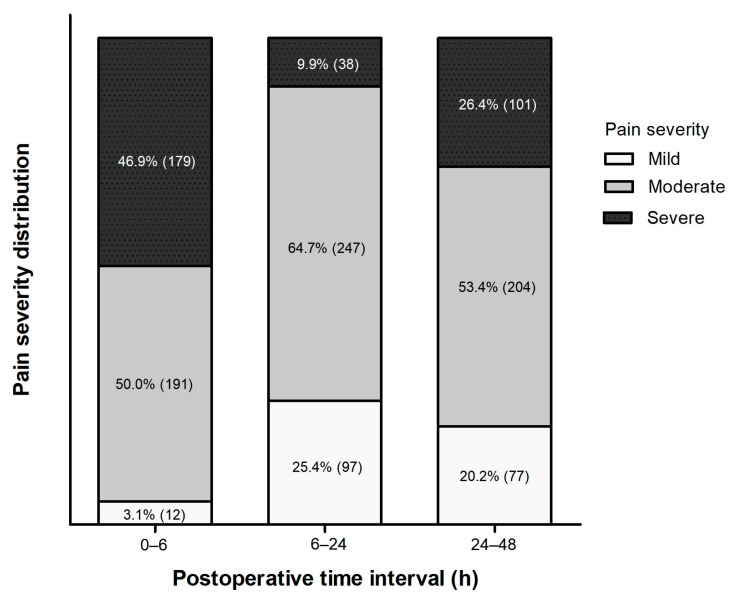 Figure 1
Figure 1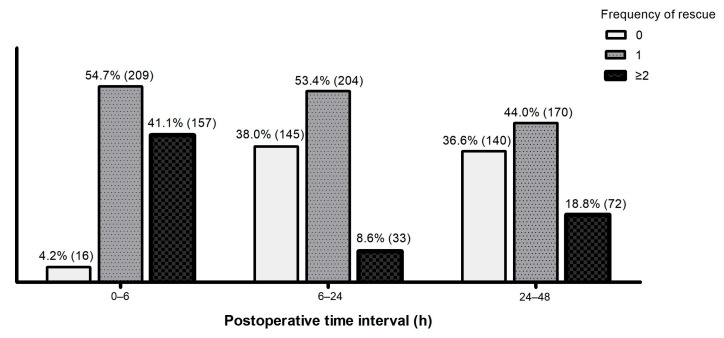 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPectus Deformity Diagnosis and Treatment · Scoliosis diagnosis and treatment · Pleural and Pulmonary Diseases
1. Introduction
Pectus excavatum (PE) is the most common congenital deformity of the anterior chest wall, characterized by posterior depression of the sternum and adjacent costal cartilages. Although the condition is usually diagnosed in childhood or adolescence, many patients present for surgical correction in adulthood due to persistent cosmetic and functional concerns [1,2]. Among available techniques, the minimally invasive repair of pectus excavatum (MIRPE) has become a commonly performed procedure that elevates the depressed sternum using one or more metal bars inserted beneath it [3,4]. Although MIRPE offers less tissue disruption and better cosmetic outcomes than open repair, postoperative pain remains a major clinical concern—particularly in adults whose increased mature chest wall rigidity and costal cartilage ossification exacerbate tissue stress and require greater intercostal nerve traction pressure during bar rotation, contributing to more postoperative pain compared to children and adolescents [5,6].
Although the severity of postoperative pain after MIRPE in adult patients has been well recognized, the intensity of postoperative pain and the amount of opioid required for adequate analgesia during this immediate postoperative period vary widely among individuals. Understanding the factors that contribute to this variability is essential for optimizing individualized postoperative pain management. However, the perioperative factors associated with increased opioid requirements and pain severity during this period remain insufficiently defined in adult patients undergoing MIRPE. Most prior studies have focused on pediatric or adolescent populations or have primarily evaluated analgesic techniques rather than patient- or surgery-related determinants of pain. Consequently, data specifically addressing factors associated with postoperative pain and opioid consumption in adult MIRPE remains limited and inconsistent.
This study aimed to investigate perioperative factors associated with postoperative opioid requirements and pain intensity during the early postoperative phase in adult patients undergoing MIRPE.
2. Materials and Methods
2.1. Study Design and Study Population
This retrospective study was conducted at a tertiary university hospital and approved by the Institutional Review Board (KC25RISI0737). The requirement for informed consent was waived due to the retrospective nature of the study. The study was conducted in accordance with the Declaration of Helsinki and reported according to the STROBE guidelines.
Data were collected from the electronic medical records (EMR) of adult patients aged 18 years or older who underwent MIRPE between March 2011 and January 2023. Patients were excluded if they had an American Society of Anesthesiologists (ASA) physical status of III or higher, previous thoracic surgery, including prior MIRPE, preoperative chronic pain or long-term use of analgesic medications, allergy to local anesthetics, or incomplete perioperative data such as pain scores or opioid dosage records.
2.2. Surgical Techniques
All operations in this study were performed by a single, experienced surgeon, which ensured technical consistency and minimized heterogeneity within the study cohort. After induction of general anesthesia, the patient was placed in the supine position. Both arms were gently elevated and suspended overhead with arm slings prior to surgical field preparation and draping, thereby securing optimal exposure.
As an initial step, the Easy crane system (Primemed, Seoul, Republic of Korea) was employed to elevate the depressed sternum using either sternal wire sutures or a spiral screw connected to the crane device. This maneuver improved visualization of the operative field and enhanced procedural safety. Following this step, the surgeon determined the appropriate bar length, configuration, hinge points, and incision sites.
Skin incisions, typically 2 cm in length, were made at the midaxillary lines. The number of incisions was determined by the chosen bar configuration. Various bar configurations—including single, multiple parallel, cross, or XI patterns—were applied depending on the deformity, with the ultimate goal of achieving entire chest wall remodeling. Pectoscopic guidance was utilized for safe mediastinal dissection and controlled passage of the pectus bar beneath the elevated sternum. Once the bar was positioned, it was rotated. The resulting chest wall contour was carefully evaluated, and the maneuver was repeated multiple times when necessary to achieve the most satisfactory chest wall contour.
For stabilization, various methods were applied according to the patient’s condition and bar configuration. These included claw fixators, bridge plates, hinge plates, and intercostal sutures, either individually or in combination, to ensure firm anchorage and to prevent bar displacement. Following bar fixation, chest wall contouring was performed using the “magic string” technique and the “flare-buster” method, effectively addressing costal flares and residual protuberances to achieve smooth remodeling of the chest wall.
Finally, portable anteroposterior chest radiography was obtained intraoperatively to confirm accurate bar positioning and to exclude complications such as pneumothorax and hemothorax. Drainage catheters (EZ-VAC silicone type; Gems Korea, Seoul, South Korea) were routinely inserted into the thoracic cavity and removed during the postoperative course as clinically appropriate.
2.3. Anesthetic and Analgesic Management
All patients underwent general anesthesia and postoperative pain management according to the institutional protocol for this procedure. General anesthesia was induced with propofol (1.5–2.0 mg/kg) and rocuronium (0.6–1.0 mg/kg), followed by endotracheal intubation. Mechanical ventilation was maintained with a tidal volume of 4–6 mL/kg and an inspired oxygen fraction of 0.4–0.5, keeping end-tidal CO_2_ between 35 and 40 mmHg. Anesthesia was maintained with sevoflurane and continuous remifentanil infusion as part of a balanced anesthesia technique. Sevoflurane was primarily titrated based on a bispectral index of 40–60, and remifentanil was subsequently adjusted to maintain hemodynamic parameters within 20% of baseline. At the end of the procedure, sevoflurane and remifentanil infusion were stopped and residual neuromuscular blockade was reversed with 4 mg/kg sugammadex.
A multimodal analgesic protocol was applied throughout the perioperative periods. After bar placement, intercostal nerve blocks were performed by the surgeon at the fourth to ninth intercostal spaces using 0.5% ropivacaine (2 mL per level, diluted with normal saline). A continuous wound infiltration system (CWIS; ON-Q^®^ Pain Relief System, Halyard, Alpharetta, GA, USA) was placed bilaterally through posterior axillary lines to deliver 0.25% ropivacaine (diluted to a total volume of 300 mL with normal saline) at a rate of 4 mL/h per side. Intravenous patient-controlled analgesia (IV–PCA; AutoMed 3200^®^, ACE Medical Corp., Seoul, Republic of Korea) solution contained fentanyl (20 µg/kg) diluted with normal saline to a total volume of 100 mL. PCA devices were set to deliver a basal infusion of 1 mL/h and a bolus of 1 mL with a lockout interval of 10 min. Both CWIS infusion and IV PCA were initiated immediately upon the patient’s arrival in the post-anesthesia care unit (PACU).
In the PACU, pain intensity was evaluated every 10 min using the visual analog scale (VAS; 0 = no pain, 10 = worst imaginable pain). When the VAS score exceeded 4 despite the use of CWIS and IV PCA, supplemental fentanyl (25–50 µg) or pethidine (12.5–25 mg) was administered intravenously. If pain persisted, intravenous ketorolac (30 mg) was administered as an adjunct rescue analgesic.
During the ward stay, pain scores were assessed every 4 h. All patients routinely received scheduled oral combination analgesics consisting of codeine phosphate 10 mg, ibuprofen 200 mg, and acetaminophen 250 mg three times daily to provide baseline analgesia. Oral medications were not used as rescue analgesics. When breakthrough pain occurred (VAS > 4) despite scheduled oral analgesics, intravenous ketorolac (30 mg) was administered first, followed by intravenous pethidine (25 mg) if pain persisted. If nausea or vomiting occurred, opioid-based PCA was temporarily discontinued and replaced with non-opioid analgesics. The CWIS catheters were routinely removed approximately 24 h postoperatively, at the time of wound drain removal.
2.4. Data Collection
Demographic, anatomic, operative, and analgesic data were extracted from electronic medical records. Demographic variables included age, sex, body mass index (BMI), and ASA physical status. Anatomic severity was quantified using the Haller index (HI) and depression index (DI), both calculated from preoperative chest computed tomography (CT) scans. The HI was defined as the ratio of the transverse chest diameter to the anteroposterior distance between the posterior surface of the sternum and the anterior border of the vertebral body [7]. The DI was calculated on the same CT slice as the ratio of the vertical distance from the deepest point of the sternum to a line connecting the most anterior portions of the bilateral ribs, divided by the transverse diameter of the corresponding vertebral body [8]. Operative data included operation time, number and length of inserted bars, and intraoperative fluid balance, calculated as total infused volume minus blood loss. Analgesic-related data included the total opioid dose delivered via PCA and the frequency and dosage of additional rescue analgesics, including both opioid and non-opioid agents.
All opioid consumption (including PCA and rescues) was converted to morphine equivalent dose (MED) normalized by body weight (MED/kg) using standard conversion ratios (10 mg morphine = 100 µg fentanyl = 100 mg pethidine) [9]. Opioid use was analyzed using two complementary measures: (1) interval MED/kg, representing the opioid amount administered within each time window; and (2) cumulative MED/kg, representing the total opioid dose from the end of surgery up to each corresponding time point.
Postoperative pain intensity was evaluated by nurses using the VAS at regular postoperative intervals and documented in the EMR. For analysis, peak VAS values were categorized into three postoperative time windows: 0–6 h, 6–24 h, and 24–48 h after arrival in the PACU. Pain severity was further classified as mild (VAS 0–3), moderate (VAS 4–6), or severe (VAS 7–10).
2.5. Outcome
The primary outcome was total opioid consumption during the first 24 postoperative hours. Secondary outcomes included cumulative opioid consumption at 6 and 48 postoperative hours; opioid consumption over 0–6, 6–24, and 24–48 h; rescue requirement across these intervals; temporal changes in pain intensity (peak VAS) and pain-severity distribution within each window.
2.6. Statistical Analysis
Continuous variables were tested for normality using the Shapiro–Wilk test and are presented as mean ± standard deviation (SD) or median (interquartile range, IQR), as appropriate. Categorical variables are expressed as counts and percentages. Differences in pain scores and opioid consumption across postoperative time intervals (0–6, 6–24, and 24–48 h) were analyzed using the Friedman test with Bonferroni-adjusted pairwise comparisons.
To identify factors independently associated with postoperative opioid consumption, multivariable linear regression analysis was performed. Covariates were selected a priori based on previously published data and clinical relevance, including age, sex, BMI, HI, DI, operation time, and the number and length of inserted bars. Ordinal logistic regression was applied to explore associations between the same covariates and pain severity (mild, moderate, or severe). Statistical significance was defined as a two-sided p < 0.05. All analyses were performed using IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, NY, USA).
3. Results
3.1. Baseline Characteristics of the Study Population and Intraoperative Variables
Data were retrospectively collected from patients who underwent MIRPE between March 2011 and January 2023. Patients with missing or incomplete data were excluded, resulting in a total of 382 patients included in the final analysis. The baseline demographic and surgical characteristics of the study population are summarized in Table 1. The mean age was 22.5 ± 5.0 years, and 80.6% of the patients were male. The mean BMI was 25.9 kg/m^2^. The mean HI and DI were 4.9 ± 3.2 and 1.9 ± 1.0, respectively. Most patients underwent bar insertion with fewer than two bars and bar lengths shorter than 14 inches. No major intraoperative complications, such as bleeding or pneumothorax, were observed.
3.2. Postoperative Opioid Requirements and Pain Intensity
Postoperative opioid consumption and pain intensity exhibited significant time-dependent variations during the first 48 h after surgery (Table 2). Opioid use increased over time, with the largest amount administered within the first 24 h postoperatively (p < 0.001). Pain intensity, as indicated by the peak VAS score, was highest during the initial 0–6 h and decreased markedly during the subsequent 6–24 h (p < 0.001). A mild but statistically significant increase in pain intensity was again observed during a 24–48 h period (p < 0.001).
The proportion of patients experiencing severe pain (VAS score ≥ 7) was highest during the initial 0–6 h (n = 179, 46.9%), then decreased markedly during 6–24 h (n = 38, 9.9%). However, it increased again during 24–48 h postoperatively (n = 101, 26.4%) (Figure 1).
Rescue analgesics were administered to nearly all patients across the three postoperative intervals (0–6, 6–24, and 24–48 h). The proportion of patients who required two or more doses of PRN medication increased during 24–48 h compared with 6–24 h (Figure 2).
3.3. Predictors of Postoperative Opioid Consumption and Pain Severity
Multivariable linear regression analyses for postoperative opioid consumption at 6, 24, and 48 h are summarized in Table 3. During the first 6 h, insertion of more than three bars and higher BMI were independently associated with greater opioid requirements (p < 0.001). At 24 h—the primary analysis time point—male sex, longer operation time, and higher BMI were significant predictors of increased opioid use (p < 0.01). These associations persisted up to 48 h postoperatively, with male sex and operation time demonstrating the strongest and most consistent influence on cumulative opioid consumption (Supplementary Tables S1–S3).
Ordinal logistic regression analyses for postoperative pain severity are summarized in Table 4. During the first 6 h, patients with insertion of more than three bars reported significantly higher pain severity (p < 0.001). From 6 to 24 h, male sex and longer operation time were independently associated with more severe pain (p < 0.01). These associations remained significant at 48 h, indicating that male patients and those undergoing longer procedures consistently experienced greater postoperative pain. Neither the Haller index nor the depression index was significantly associated with pain severity at any time point.
4. Discussion
This study aimed to identify perioperative factors affecting postoperative opioid use and pain intensity during the early postoperative phase in adult patients undergoing MIRPE. Among the variables examined, male sex, higher BMI, longer operation time, and a greater number of implanted bars were significantly associated with increased opioid requirements and pain severity after surgery. In contrast, anatomical severity indices such as the HI and the DI showed no significant correlation with either opioid use or pain scores. These findings suggest that postoperative discomfort during the first 48 h after MIRPE in adults is primarily influenced by patient- and surgery-related factors rather than the severity of anatomical deformity.
Compared to earlier reports, our findings were partially consistent but also showed differences, particularly regarding gender-related variations in early postoperative pain. Most previous studies, mostly involving pediatric or mixed-age groups, have yielded inconsistent results: some indicated that female patients experienced higher pain scores and complication rates [10,11], whereas others reported the opposite [12,13]. In our adult group, male patients reported greater pain intensity and required higher opioid doses during the early postoperative period after MIRPE. Anatomical and biomechanical features of the adult thorax may explain these results. Stiffness of the costal cartilage is greater in males than in females [14], leading to greater mechanical stress on the intercostal nerves and surrounding muscles during bar rotation and fixation [15]. Additionally, males typically have thicker chest walls and more muscle mass, which can increase intercostal tension and decrease tissue flexibility [16,17]. Overall, these anatomical factors likely contribute to increased nociceptive activation, resulting in more postoperative discomfort and higher opioid needs in male patients.
The relationship between the number of inserted bars and postoperative pain has also varied across studies. One biomechanical analysis suggested that double-bar placement reduced postoperative pain during the first two postoperative days by more evenly distributing chest wall stress [18]. However, our findings showed that patients requiring three or more bars experienced greater pain in the early postoperative period. This difference may reflect the broader correction range and greater mechanical force applied across each intercostal space, rather than the number of bars itself [19,20]. Similarly, longer operation times often indicated more extensive or complex corrections, during which multiple bars were adjusted or repositioned to achieve proper correction, thereby increasing mechanical stress on the chest wall.
The absence of a significant link between deformity indices (HI and DI) and postoperative pain in our adult group differs from previous pediatric studies [6,13]. These indices measure geometric deformity but not structural rigidity, which increases significantly with age as the costal cartilage ossifies [21]. In pediatric patients, more severe deformities may cause more pain due to the elastic recoil of the flexible chest wall [22]. In contrast, in adults, ossified ribs and reduced thoracic compliance are the main factors influencing pain, decreasing the impact of geometric deformity on pain perception. This interpretation is supported by biomechanical evidence showing that the force required to achieve a similar level of sternal elevation grows exponentially with increasing thoracic stiffness [15,23].
Although BMI was not linked to differences in reported pain intensity, patients with higher BMI consistently needed higher opioid doses across all postoperative periods. This suggests that opioid requirements do not necessarily match subjective pain perception and may be influenced by multiple interacting factors. Individuals with higher body mass may have altered pharmacokinetics of lipophilic opioids such as fentanyl, including increased distribution into adipose tissue and decreased effective plasma concentrations [24]. Therefore, even at similar pain levels, patients with higher BMI may require larger doses of opioids to achieve equivalent analgesic effects.
An additional notable observation was the biphasic postoperative pain pattern, characterized by an initial peak within 6 h, a transient decline by 24 h, and a secondary rise at 24–48 h. In most surgical populations, postoperative pain generally peaks within the first 24–36 h and gradually decreases thereafter [25]. However, in our cohort, pain did not continue to decrease after 24 h but instead increased again, accompanied by a parallel rise in rescue analgesics use. While a causal relationship cannot be definitively established, the timing of this secondary increase coincided with the routine removal of the CWIS, suggesting that termination of local anesthetic delivery may expose residual inflammation and peripheral sensitization. Similar rebound phenomena have been reported following discontinuation of epidural or local infiltration in thoracic and upper abdominal surgeries, likely mediated by reactivation of inflammatory pathways as local blockade subsides [26,27].
From a clinical perspective, these findings highlight the importance of a risk-based, time-sensitive analgesic approach during the immediate postoperative period following MIRPE. Male patients, those with higher BMI, and individuals undergoing longer procedures should be identified before surgery as high-risk groups for postoperative pain and managed with tailored multimodal strategies. In such cases, extending local or regional analgesic coverage beyond 24 h—by using prolonged CWIS infusions or scheduled regional blocks—may mitigate late pain rebound. Additionally, opioid doses based on lean or adjusted body weight rather than total body weight could enhance pharmacologic accuracy in heavier adults [28]. Lastly, patients requiring three or more bars need intensified pain management and close monitoring during the first six hours after surgery to avoid breakthrough pain. Implementing individualized multimodal interventions during the early postoperative phase may improve pain control after MIRPE.
This study has several limitations. First, its retrospective design may have introduced selection and information bias. Second, as a single-center study, the findings may not be generalizable to institutions with different perioperative practices or patient populations. Third, pain assessment relied solely on the VAS measured at predefined time intervals, without incorporating multidimensional outcomes such as patient satisfaction or functional recovery. Finally, the follow-up period was limited to 48 h; therefore, the identified risk factors should not be extrapolated to the entire postoperative course or long-term pain outcomes. Nevertheless, the relatively large and homogeneous adult cohort, combined with standardized surgical techniques and consistent pain documentation, supports the internal validity of the findings and provides clinically meaningful insights into early postoperative pain management after MIRPE. Future prospective studies are warranted to validate these findings with an extended follow-up period and to explore optimized CWIS duration, adjunctive regional techniques, and individualized analgesic protocols for adult MIRPE.
5. Conclusions
In conclusion, early postoperative pain and opioid requirements after adult MIRPE during the first 48 h after surgery were associated with male sex, higher BMI, longer operation duration, and multiple-bar insertion, rather than with deformity severity. Pain showed a secondary increase around 24–48 h, coinciding with CWIS removal. These findings highlight the need for personalized and time-specific multimodal analgesic strategies to provide adequate pain control.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Biavati M. Kozlitina J. Alder A.C. Foglia R. Mc Coll R.W. Peshock R.M. Kelly R.E.Jr. Kim Garcia C. Prevalence of pectus excavatum in an adult population-based cohort estimated from radiographic indices of chest wall shape P Lo S ONE 202015 e 023257510.1371/journal.pone.023257532379835 PMC 7205298 · doi ↗ · pubmed ↗
- 2Viggiano D. Bongiolatti S. Borgianni S. Lo Piccolo R. Voltolini L. Gonfiotti A. Nuss Technique for Pectus Excavatum in Adult Patients: Cosmetic Satisfaction and Improvement of Quality of Life in a Single-Center Experience Front. Surg.2022990379110.3389/fsurg.2022.90379135722532 PMC 9198457 · doi ↗ · pubmed ↗
- 3Potaczek T. Duda S. Adamczyk J. Jasiewicz B. Tęsiorowski M. Daszkiewicz E. Comparison of Postoperative Period in Patients with Pectus Excavatum Treated with Nuss Technique and Ravitch Technique Ortop. Traumatol. Rehabil.20151757768610.5604/15093492.119301027053389 · doi ↗ · pubmed ↗
- 4Huerta C.T. Alligood D.M. Davis J.K. Ramsey W.A. Cobler-Lichter M.D. Shagabayeva L. Delamater J.M. Hernandez A.E. Parreco J.P. Perez E.A. Outcomes After Pectus Excavatum Repair: A Nationwide Comparison of Nuss Versus Ravitch Operations J. Surg. Res.202430338138910.1016/j.jss.2024.09.02539418960 · doi ↗ · pubmed ↗
- 5de Loos E.R. Pennings A.J. van Roozendaal L.M. Daemen J.H.T. van Gool M.H. Lenderink T. van Horck M. HulsewéK.W.E. Vissers Y.L.J. Nuss Procedure for Pectus Excavatum: A Comparison of Complications Between Young and Adult Patients Ann. Thorac. Surg.202111290591110.1016/j.athoracsur.2020.10.01733181130 · doi ↗ · pubmed ↗
- 6Grosen K. Pfeiffer-Jensen M. Pilegaard H.K. Postoperative consumption of opioid analgesics following correction of pectus excavatum is influenced by pectus severity: A single-centre study of 236 patients undergoing minimally invasive correction of pectus excavatum Eur. J. Cardiothorac. Surg.20103783383910.1016/j.ejcts.2009.09.03519853467 · doi ↗ · pubmed ↗
- 7Sesia S.B. Heitzelmann M. Schaedelin S. Magerkurth O. Kocher G.J. Schmid R.A. Haecker F.M. Standardized Haller and Asymmetry Index Combined for a More Accurate Assessment of Pectus Excavatum Ann. Thorac. Surg.201910727127610.1016/j.athoracsur.2018.07.08630278167 · doi ↗ · pubmed ↗
- 8Fagelman K.M. Methratta S. Cilley R.E. Wilson M.Z. Hollenbeak C.S. The Depression Index: An objective measure of the severity of pectus excavatum based on vertebral diameter, a morphometric correlate to patient size J. Pediatr. Surg.2015501130113310.1016/j.jpedsurg.2014.11.04325783321 · doi ↗ · pubmed ↗