The Significance of Hypophosphatemia in Deciding on an Optimal Clinical Choice of Parenteral Iron Therapy in Patients with Chronic Inflammatory Bowel Disease in Slovenia: An Umbrella Review and Economic Evaluation
Rok Hren, Tamás Dóczi, Erika Országh, Tomaž Kocjan

TL;DR
This study evaluates the cost-effectiveness of different IV iron therapies for IBD patients in Slovenia, considering hypophosphatemia risks and treatment costs.
Contribution
The study integrates an umbrella review and economic modeling to assess IV iron therapies in Slovenia's unique healthcare context.
Findings
FDI required fewer infusions than FCM but had higher drug costs and similar savings due to low infusion tariffs.
FDI showed better cost-effectiveness when considering hypophosphatemia-related QALYs.
Hypophosphatemia incidence was significantly higher with FCM compared to other IV iron formulations.
Abstract
Background/Objectives: Iron-deficiency anemia (IDA) is a common extraintestinal complication of inflammatory bowel disease (IBD). Among high-dose intravenous (IV) iron options, ferric carboxymaltose (FCM) carries a higher risk of treatment-emergent hypophosphatemia than ferric derisomaltose (FDI), with potential clinical consequences. Slovenia’s healthcare setting, characterized by very low IV iron infusion tariffs and recent pricing in which FCM is substantially less expensive than FDI, warrants a setting-specific cost effectiveness evaluation. Methods: We integrated two methodological components: (i) a payer-perspective cost-effectiveness analysis using a patient-level microsimulation model with (ii) an umbrella review of systematic reviews and a targeted search of expert consensus statements on IV-iron-associated hypophosphatemia. Results: In the base case, FDI required fewer…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
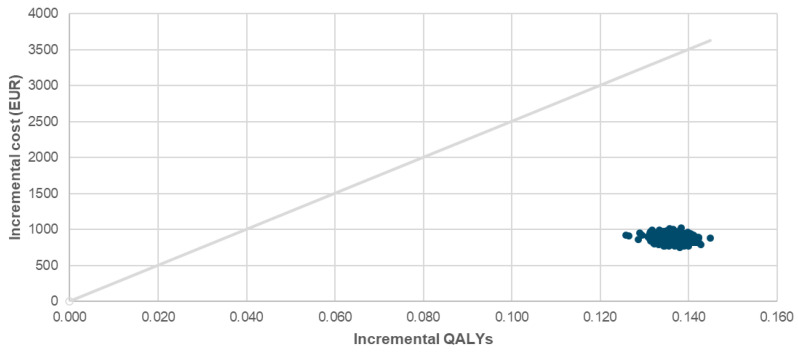 Figure 1
Figure 1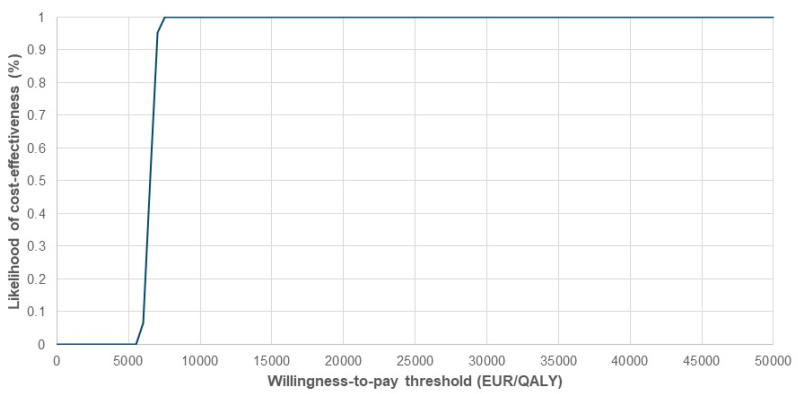 Figure 2
Figure 2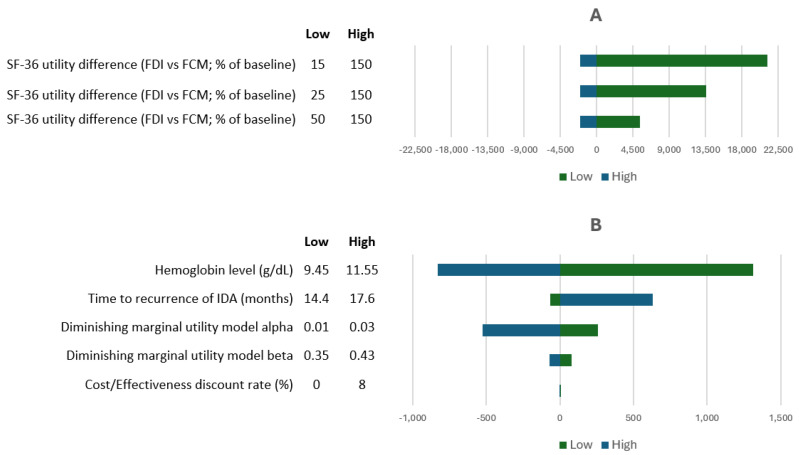 Figure 3
Figure 3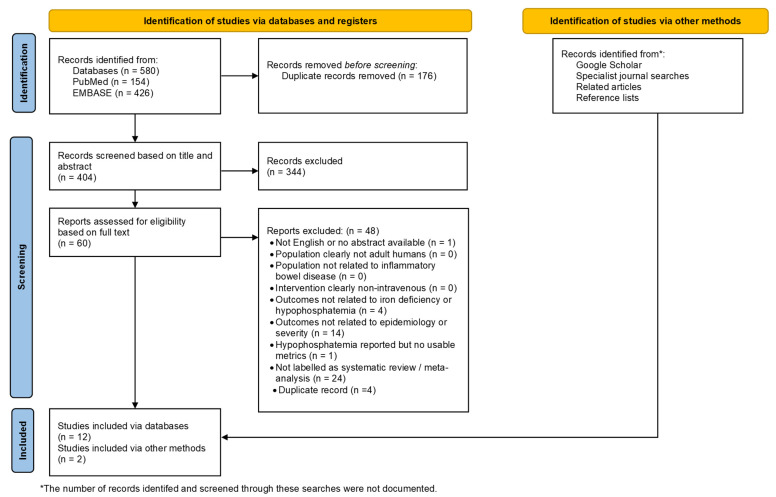 Figure 4
Figure 4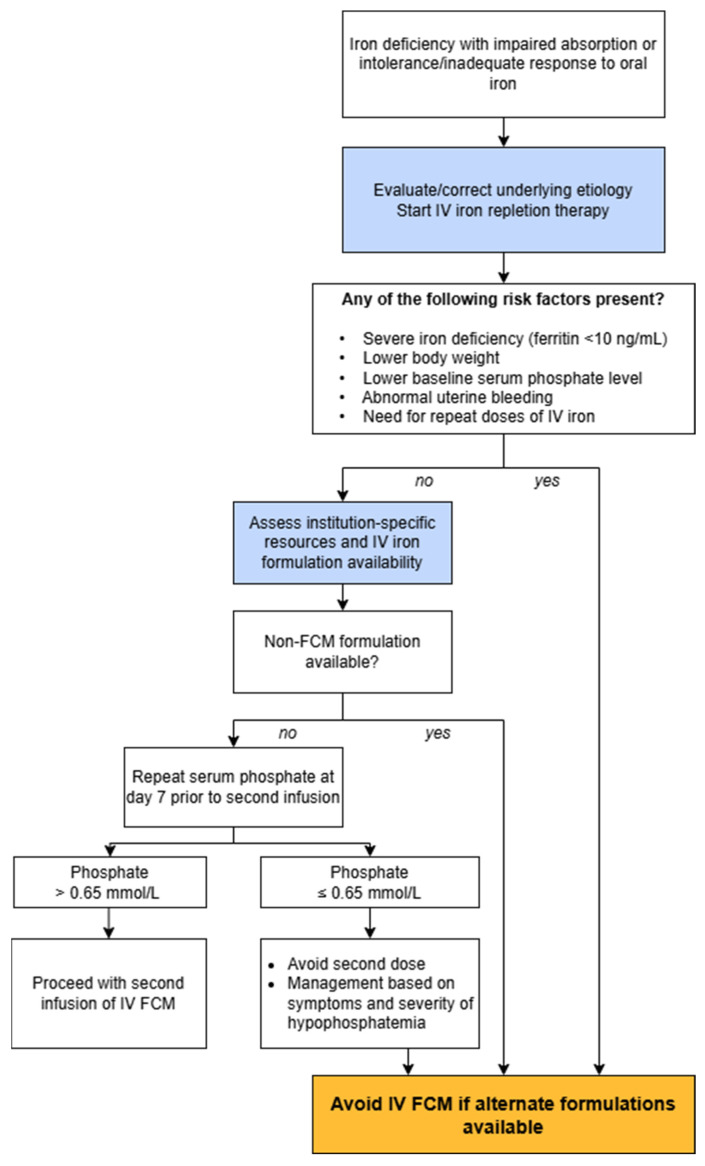 Figure 5
Figure 5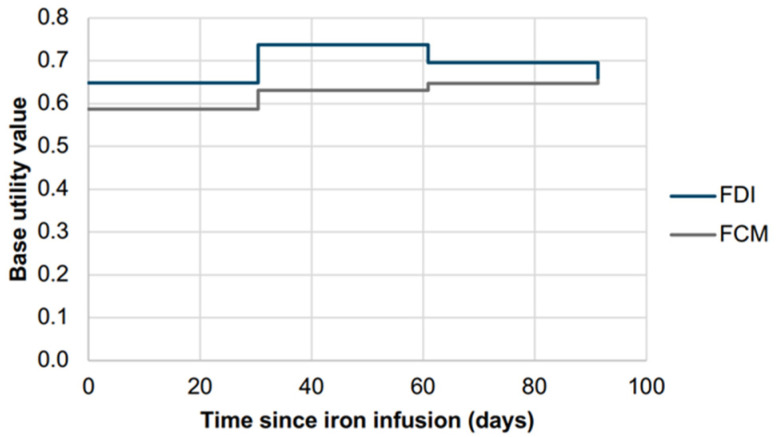 Figure 6
Figure 6- —Ewopharma d.o.o., Ljubljana, Slovenia
- —Slovenian Research and Innovation Agency
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIron Metabolism and Disorders · Erythropoietin and Anemia Treatment · Inflammatory Bowel Disease
1. Introduction
Anemia is a common extraintestinal complication of inflammatory bowel disease (IBD), with its main causes being iron deficiency due to chronic blood loss, dietary adaptations among patients with IBD, and chronic inflammation that reduces iron absorption from the gastrointestinal tract [1]. IBD-associated anemia has a significant impact on patients’ physical and cognitive functioning, increases hospitalization rates, and reduces quality of life [2,3,4,5,6]. The European Crohn’s and Colitis Organization (ECCO) recommends intravenous (IV) iron as the first-line treatment for, inter alia, patients with clinically active IBD and iron-deficiency anemia [4,5], since the absorption of oral iron is limited in patients with intestinal inflammation [7]. Historically, IV iron is considered a safe medication, with an estimated rate of serious adverse reactions of approximately one per 200,000 administrations [8,9].
Among the available high-dose IV iron preparations used for the treatment of iron deficiency, there are two commonly used and clinically comparable agents: ferric carboxymaltose (FCM) and ferric derisomaltose (FDI), previously known as iron ferric isomaltoside. Safety distinction in clinical practice is hypophosphatemia, which occurs frequently with FCM (in up to 92% of cases) and saccharated ferric oxide (SFO), but rarely with other iron preparations like ferumoxytol, low-molecular-weight iron dextran (LMWID), or FDI (in 2–8% of cases) [10,11,12,13,14,15,16,17,18]. The mechanism is not fully understood; however, it is most likely related to the increase in intact fibroblast growth factor 23 (FGF-23), a phosphatonin that enhances renal phosphate excretion [13,19,20,21,22] after use of FCM.
Hypophosphatemia [23,24] may in approximately 10% become severe (phosphate < 0.32 mmol/L or 1 mg/dL) [25], symptomatic, or persistent for up to six months, leading to disturbances in bone and mineral metabolism and the development of osteomalacia [26,27,28,29,30,31,32]; in one case, even burosumab, a therapeutic monoclonal antibody against FGF-23, was proposed as an off-label treatment option [33]. Severe hypophosphatemia has been documented after both single and repeated FCM infusions, particularly in individuals with normal renal function and high cumulative iron doses [27,34,35,36,37,38,39,40,41,42,43,44].
In recognition of these risks, the UK Medicines and Healthcare products Regulatory Agency (MHRA) issued a 2020 Drug Safety Update advising serum phosphate monitoring in patients receiving multiple or long-term FCM treatments or those with predisposing factors for hypophosphatemia such as IBD [22,45]. Early identification and management are crucial to prevent chronic complications like osteomalacia and fractures, including those requiring surgery [45]. The ECCO 2024 guidelines have also addressed the risks in relation to FCM use in IBD patients [5], and the Summary of Product Characteristics (SmPC) for FCM now includes a special subsection under Section 4.4 specifically related to hypophosphatemic osteomalacia.
Moreover, there is growing perception that differences in the incidence and consequences of hypophosphatemia between IV iron formulations may also have important economic implications. Several pharmacoeconomic cost–utility (CU) analyses conducted across diverse healthcare settings, including China [46,47], the United Kingdom [48], Norway [49], and Sweden [50], have consistently shown FDI to be the dominant strategy, being both more effective and less costly than FCM. However, these evaluations were performed for pricing conditions where FDI and FCM were of comparable cost, and where iron infusion expenses were relatively high compared to the drug cost itself.
In Slovenia, by contrast, the cost structure differs substantially; iron infusion costs are exceptionally low (under €40 per infusion), and as of summer 2025, the price of FCM has decreased to 42% of the cost of FDI. These two parameters together justify a new economic evaluation to determine the potential consequences of this significant pricing shift. Moreover, Slovenia provides a representative model for Central and Eastern European (CEE) healthcare systems [51,52,53,54], with a well-developed and transparent pharmaceutical framework [55].
The objectives of the present study are therefore twofold: (i) to extend previous pharmacoeconomic evaluations by incorporating the current Slovenian cost environment, and (ii) to place these economic findings within the context of the latest clinical evidence, including recent systematic reviews and expert consensus statements. In doing so, this study aims to provide a comprehensive assessment of both the economic and clinical implications of FCM and FDI in the management of iron deficiency anemia (IDA) among patients with IBD.
2. Materials and Methods
Our methodological approach integrated pharmacoeconomic modeling (Section 2.1) with an umbrella review synthesizing evidence from systematic reviews and targeted search of consensus statements (Section 2.2).
2.1. Pharmacoeconomic Modeling
2.1.1. Model Structure
A cost-effectiveness analysis was conducted to evaluate FDI compared to FCM for patients with IDA and IBD in Slovenia. We conducted our analysis using the CU-IDA Model [48] to estimate the incremental costs and health benefits of a treatment of IDA in patients with IBD. The CU-IDA Model is a patient-level microsimulation model that simulates individual iron requirements and the number of infusions per treatment cycle according to the product characteristics of each IV iron formulation. Baseline characteristics were derived from the PHOSPHARE-IBD randomized controlled clinical trial (RCT), which enrolled patients from 20 outpatient hospital clinics across Austria, Denmark, Germany, Sweden, and the UK [12,38]. We used the CU-IDA Model as it was previously applied across multiple jurisdictions [46,47,48,49,50], while the PHOSPHARE-IBD study is pivotal, as it provided the first high-quality prospective evidence in an IBD population demonstrating that hypophosphatemia is a formulation-specific and clinically relevant adverse effect of IV iron therapy. The analysis assumed equivalent hematological responses and hemoglobin increases between FDI and FCM, consistent with findings from PHOSPHARE-IBD [12]. The key difference captured by the model related to the incidence of hypophosphatemia. Although other adverse events could have been considered, the analysis was deliberately conservative and focused solely on hypophosphatemia. For example, Pollock and Biggar [56] reported a lower risk of serious or severe hypersensitivity reactions with FDI compared with FCM and iron sucrose; however, this difference was not incorporated into the model. In the Slovenian adaptation of the model, as in prior versions [47,48,49,50], fractures were excluded to ensure a scientifically rigorous approach; while emerging data shows an increased fracture risk, no peer-reviewed data documenting the risk in clinical practice has been published so far. Data on quality-of-life differences between patients receiving FDI and FCM were based on the PHOSPHARE-IBD study [12,57], which assessed health status using the SF-36v2 questionnaire (36-Item Short Form, second version) [58]. This approach also allowed us to quantify the negative effects of symptomatic hypophosphatemia, such as general weakness and fatigue (baseline utility values for FDI and FCM can be found in Figure A1 of Appendix A [48]). The modeling structure, treatment sequencing, and decision rules followed those described previously [47,48,49,50], with all parameters, except those explicitly detailed below, remaining consistent with the reference model [48]; model parameters are summarized in Table 1. Simulations were performed from the payer perspective, including 2000 virtual patients with IBD treated for IDA. Indirect costs were excluded, consistent with Slovenian payer guidelines. Additional details of the health economic model are provided in Appendix A.
The analysis adhered to Slovenian pharmacoeconomic guidelines, applying a willingness-to-pay (WTP) threshold of €25,000 per QALY [61] and discount rate of 3.5% for both costs and outcomes. The incremental cost-effectiveness ratio (ICER) was calculated to assess the value of FDI relative to FCM over a 10-year time horizon.
2.1.2. Payer Perspective Costing
Drug acquisition costs were derived from the most recent hospital procurement data and publicly available price listings. The cost for FDI was obtained from recent tenders in 2025 (€0.19 per mg), while the cost for FCM was based on the Slovenian official list price (€0.08 per mg). These unit costs were assumed to apply both in the initial treatment year and in subsequent years. Administration costs for iron infusions were obtained from the Slovenian payer tariff list for 2025, using the code APL022 (€35.06), which covers all non-pharmaceutical costs associated with iron infusion, including nursing time, consumables, patient observation, and proportional overheads such as utilities, facility maintenance, and capital depreciation.
The model also accounted for adverse events. For patients treated with FCM, the model assumed serum phosphate measurement after the first IV administration. If hypophosphatemia was detected, the patient would receive phosphate replacement therapy—either oral [22] or intravenous [62], depending on severity—and undergo an additional follow-up measurement. If a second iron infusion was required, phosphate levels were again checked afterward. For the costs of IV phosphate administration, we used the tariff APL005 of €134.78 from the Slovenian payer price list for 2025. The cost of serum phosphate measurement was calculated based on the price of the test (€1.30) and the sample collection fee (€2.50), as specified in the Synlab laboratory price list (https://www.synevo.si/images/Medicover/Cenik_Synevo_Adria_lab.pdf; accessed on 28 January 2026). For patients receiving FDI, phosphate monitoring was not included in the model, as this requirement is absent from the product information, and the PHOSPHARE-IBD clinical trial reported no severe cases of hypophosphatemia [12].
2.1.3. Uncertainty Analysis
To explore the impact of parameter uncertainty, we conducted probabilistic sensitivity analysis (PSA). In this approach, model input parameters were simultaneously varied within their assigned probability distributions, generating outcome distributions that reflect overall model uncertainty. The PSA comprised 1000 Monte Carlo simulations per virtual patient.
In addition to the base case scenario, which assumed a lower number of IV infusions for FDI compared with FCM (reflecting the maximum weekly cumulative dose of 1000 mg for FCM), a scenario analysis was conducted in which FCM was offered at zero cost.
As part of the sensitivity analysis, we also incorporated alternative IV iron administration costs based on Danish data. In Denmark, the cost of IV iron administration in 2023 was 1529 DKK (drop from 2855 DKK in 2018 [63]), which, after adjustment for gross domestic product in purchasing power parity and conversion to euros at the prevailing exchange rate, corresponded to €146.80 (compared with €35.06 in the base case scenario). The purpose of this particular scenario was to assess cost-effectiveness under conditions reflecting IV iron administration costs typical of developed healthcare systems; for reference, the corresponding infusion cost in another high-income setting was 3656 NOK (around €310) in Norway [49]. Denmark was selected because, similar to Slovenia, IV iron therapy is reimbursed using a split tariff structure, with the cost of administration and the cost of the iron product reimbursed separately. In contrast, in countries such as the United Kingdom, IV iron therapy is reimbursed as a bundled, per-infusion price [48].
2.2. Umbrella Review of Systematic Literature Reviews and Targeted Search of Consensus Statements
A comprehensive literature search was conducted on 1 September 2025 using PubMed and EMBASE, with no limitations on publication date and with restrictions on the publication/study type. The umbrella literature review was conducted and reported in compliance with the PRISMA 2020 Statement [64]. Any peer-reviewed systematic review or meta-analysis reporting on hypophosphatemia during IV iron treatment of IDA were eligible. Duplicate records were removed both within and across databases. When identical work was published first in conference proceedings and later in a peer-reviewed journal, the proceedings version was treated as a secondary report and discarded. We adopted the format of a narrative review. Records that did not meet any exclusion criteria at the full-text screening stage were included. A more detailed description of the methodology, including PICOS, search strings, and exclusion criteria during title/abstract and full-text screening, is reported in Appendix B. In addition to the umbrella review, a targeted search was conducted to identify recommendations and consensus statements on hypophosphatemia during IV iron treatment of IDA.
3. Results
3.1. Pharmacoeconomic Modeling
Table 2 summarizes the results of the cost-effectiveness analysis, showing that in the base-case scenario for treating IDA in patients with IBD, ICER comparing FDI and FCM was €6590/QALY. Patients receiving FDI required on average 11.1 iron infusions per patient over ten years, compared with 14.2 infusions for those treated with FCM, 3.1 fewer infusions per patient. This implies that in an infusion service with fixed capacity, for every 100 patients treated with FDI, about 78 patients with comparable iron requirements could be treated using FCM.
However, because of the low cost of IV iron administration in Slovenia, this reduction translated into only €95 in savings. In contrast, iron procurement costs were substantially higher for FDI, resulting in an incremental cost of €1166 over ten years, which more than offset the modest savings in IV iron administration costs and additional costs (€176) associated with hypophosphatemia in the FCM arm.
Figure 1 presents the cost-effectiveness plane comparing FDI and FCM. The PSA demonstrated a mean incremental QALY gain of 0.136, the same as in the deterministic base case, and a mean incremental cost of €875, closely matching the deterministic base case estimate of €895. This resulted in a mean ICER of €6198/QALY, compared to €6590/QALY in the deterministic base case. As shown in Figure 1, all iterations in PSA fell within the northeast quadrant of the cost-effectiveness plane but under WTP threshold of €25,000/QALY, confirming consistent cost-effectiveness. The cost-effectiveness acceptability curve (Figure 2) showed a 100% probability of cost-effectiveness at €8000/QALY. When FCM was modeled at zero acquisition cost, the ICER increased to €12,669/QALY (Table 2), yet remained below the Slovenian WTP threshold of €25,000/QALY, indicating the surprising robustness of the findings across cost settings. A sensitivity analysis using adjusted Danish IV iron administration costs (Table 2) further supported these findings, yielding an ICER of €4358/QALY. Results of a one-way sensitivity analysis are presented in Figure 3. When the clinical relevance of hypophosphatemia was minimized by applying a substantially reduced quality-of-life impact (15–50% of the baseline utility difference between FDI and FCM derived from SF-36 data), the resulting ICERs ranged from €11,938 to €27,719 per QALY. Under this scenario, the pharmacoeconomic advantage of FDI was attenuated, providing a lower-bound estimate of its cost-effectiveness.
3.2. Umbrella Review of Systematic Literature Reviews and Targeted Search of Consensus Statements
This review had two main objectives: (1) to identify systematic reviews reporting data on IV iron-induced hypophosphatemia and (2) to identify recommendations or consensus statements on its management. A comprehensive literature review was conducted to find potentially relevant articles from MEDLINE/PubMed and EMBASE databases (see Appendix B). A total of 580 records were identified (PubMed: 154, EMBASE: 426). After removing 176 duplicates, 404 records were screened by title and abstract. Of these, 344 were excluded as irrelevant, leaving 60 articles for full-text assessment, of which 12 met the inclusion criteria and were selected for data extraction. To ensure that no recently published or poorly indexed studies were missed, a brief, targeted supplementary search was performed after the primary PubMed and EMBASE search. During this search we identified two additional reviews [22,63] that were included in this umbrella review. Exclusion of two studies deserves a special note. One study [65] was excluded because it focused exclusively on trials directly comparing FCM with iron sucrose, while another study [66] examined only studies comparing oral versus IV iron during gastrointestinal bleeding; both were considered too narrowly scoped for the purposes of our analysis.
In total, 14 studies (12 from database searches and 2 from supplementary database sources) [10,11,19,24,31,67,68,69,70,71,72,73,74,75] constitute the evidence base of this umbrella review. The process of study identification, screening, and inclusion is illustrated in the PRISMA flow chart (Figure 4). This diagram provides a step-by-step summary of the number of records retrieved, screened, excluded, and finally included in the evidence base.
In addition to the umbrella review, a targeted literature search was also conducted to identify papers about the clinical management of hypophosphatemia associated with FCM. This search was intentionally restricted to consensus statements, clinical recommendations, and expert guidance documents, using predefined terms related to “FCM”, “hypophosphatemia”, “monitoring”, and “clinical management”. Primary studies and case reports were excluded to ensure a focus on clinical guidance. Eight recommendations and consensus papers were identified [22,29,32,76,77,78,79,80]. The selected studies were systematically organized based on whether they were systematic reviews or recommendations/consensus statements (Table 3). We report the results in the form of a narrative summary.
3.2.1. Systematic Reviews
Early reviews primarily addressed the efficacy of IV iron therapy and either did not mention hypophosphatemia [81,82,83,84] or only mentioned it in passing [85]. Avni et al. [67] quantified IV iron use with increased risk of hypophosphatemia, while both Rognoni et al. [68] and Aksan et al. [69] offered only scanty evidence on incidence of hypophosphatemia in patients treated with IV iron.
Zoller et al. [24] provided one of the earliest overviews of IV-iron-induced hypophosphatemia as a clinically relevant and potentially long-term complication. Across 17 analyzed studies, hypophosphatemia occurred in 58% (95% confidence interval 42–74%; based on three studies) of FCM-treated patients with normal kidney function, higher than with other IV iron formulations. The authors also summarized 29 documented clinical cases linking FCM, iron polymaltose, and saccharated iron oxide to severe complications, such as osteomalacia and fractures.
Glaspy et al. [10] identified 40 studies (19 RCTs, 10 retrospective or observational studies, and 11 case reports) that investigated hypophosphatemia associated with IV iron therapies for IDA. Reported incidence varied widely across formulations, ranging from 0 to 92% with FCM, 0–40% with iron sucrose, 0.4% with ferumoxytol, and none with LMWID. Case reports described severe and chronic hypophosphatemia leading to fatigue, bone pain, osteomalacia, and fractures, particularly after repeated FCM dosing.
Bellos et al. [11] conducted a Bayesian network meta-analysis of eight randomized controlled trials (n = 5989) to compare the risk of hypophosphatemia among IV iron formulations used for treating IDA. The analysis showed that FCM was associated with higher incidence of hypophosphatemia than FDI (RR 7.9), iron sucrose (RR 9.4), LMWID (RR 6.6), and ferumoxytol (RR 24.0). FCM ranked worst overall, with a surface under the cumulative ranking curve (SUCRA) of 99.1%, indicating the highest likelihood of causing hypophosphatemia. Median incidence across studies was 45% for FCM versus <5% for other agents. Severe (serum phosphate < 0.42 mmol/L or 1.3 mg/dL) and persistent hypophosphatemia (serum phosphate < 0.65 mmol/L or 2 mg/dL ≥ 2 weeks post-treatment) occurred mainly after FCM administration.
Rosano et al. [70] performed a post hoc pooled analysis of 45 interventional trials (n = 15,080; 8245 received FCM) to evaluate the frequency, duration, and clinical relevance of hypophosphatemia following FCM treatment. This pooled analysis confirmed that FCM is associated with an increased rate of serum phosphate reduction. Among 6879 patients receiving FCM therapy, 41.4% experienced phosphate levels < 0.81 mmol/L (2.5 mg/dL) and 0.7% dropped below 0.32 mmol/L (1 mg/dL). Serum phosphate declined most markedly at 2 weeks post-infusion (mean −0.4 mmol/L or −1.24 mg/dL) and generally normalized by week 8–12. Hypophosphatemia was more frequent in gastroenterology and women’s health populations and among those receiving multiple or higher cumulative FCM doses (>1000 mg).
Schaefer et al. [71] conducted a systematic review and meta-analysis of 42 prospective clinical trials to compare the incidence, severity, and duration of hypophosphatemia following treatment with FCM versus FDI. The pooled analysis showed higher risk of hypophosphatemia with FCM (47%, 95% CI 36–58%) compared with FDI (4%, 95% CI 2–5%), and a greater mean serum phosphate reduction (−0.40 vs. −0.06 mmol/L). Hypophosphatemia persisted for up to three months in 45% of FCM-treated patients. Meta-regression identified low baseline ferritin, low transferrin saturation, and normal kidney function as predictors of hypophosphatemia.
In 2021, Glaspy et al. [31] built upon their earlier review [10], identifying 20 RCTs published between 2008 and 2020 that reported serum phosphate outcomes, 19 of which involved FCM. Across these studies, the incidence of hypophosphatemia ranged from 40% to 70%, with moderate and severe cases (phosphate < 2.0 mg/dL or <0.65 mmol/L), occurring in roughly up to half of FCM-treated patients, and severe cases (<1 mg/dL or 0.32 mmol/L) up to roughly 10%. The review indicated that hypophosphatemia often persists for weeks to months, occasionally leading to osteomalacia and fractures, especially after repeated dosing. The authors also summarized 15 newly reported clinical cases of symptomatic iron-induced hypophosphatemia published since the 2017 review by Zoller et al. [24], most involving patients with IDA repeatedly treated with FCM, although a few received iron polymaltose or iron sucrose. About half of the cases involved long-term FCM exposure (up to 4 years), with several developing osteomalacia and multiple fractures, especially among patients with Crohn’s disease.
The systematic review by Vilaca et al. [72] examined 28 case reports (30 cases total) of osteomalacia linked to repeated IV iron infusions. Most patients (n = 18) received FCM, with others given SFO (n = 8) or iron polymaltose (n = 3); in one patient the iron therapy was not reported. The majority had underlying gastrointestinal disorders, often requiring prolonged iron therapy. Across cases, persistent hypophosphatemia (median 0.36 mmol/L) and elevated FGF-23 were consistently observed, accompanied by high alkaline phosphatase, bone pain, and fractures or pseudofractures. Imaging typically revealed focal isotope uptake consistent with osteomalacia. Symptoms improved primarily after discontinuing or switching iron formulations, whereas vitamin D or phosphate supplementation offered limited benefit.
Rosano et al. [73] conducted another pooled analysis of 41 clinical trials including 7931 adults treated with FCM, this time to evaluate the risk of hypophosphatemia in heart failure (HF) compared to other conditions. Among the cohort, 14% had HF, and the incidence of moderate or severe hypophosphatemia (serum phosphate < 0.65 mmol/L or 2.0 mg/dL) was 8.1% in HF patients versus much higher rates in other groups, such as 30–55% in women’s health, gastrointestinal, and neurology populations. Only one HF patient (<0.1%) developed severe hypophosphatemia (<0.32 mmol/L or 1.0 mg/dL), compared with 4.8% and 4.0% of the subjects in the neurology and gastrointestinal groups, respectively. Serum phosphate levels typically decreased at weeks 2–4 and returned to baseline by week 8, mirroring findings in other subgroups. Preserved kidney function was identified as the strongest predictor of hypophosphatemia (odds ratio 12.2 for eGFR > 60 vs. <30 mL/min/1.73 m^2^). The study concluded that FCM-associated hypophosphatemia in HF is infrequent, transient, and rarely symptomatic, likely due to coexisting renal impairment limiting phosphate excretion, though monitoring remains advisable in cases of repeated dosing or high cumulative exposure. A recent study [86] though reported a hypophosphatemia incidence of 51% following FCM administration in HF patients. This discrepancy may reflect differences in assessment timing, as patients in Rosano et al. [73] were not systematically monitored and many were evaluated after the 2-week nadir period, when phosphate levels may have already begun to recover.
Malireddi et al. [74] performed a systematic review of 14 studies (five randomized controlled trials and nine observational studies, n = 2493) to assess the safety and efficacy of FCM for treating IDA in IBD patients. The incidence of hypophosphatemia after FCM infusion ranged from 21% to nearly 73% in various trials, typically peaking within two weeks post-infusion, with some patients remaining hypophosphatemic for over a month.
Magagnoli et al. [19] conducted a comprehensive systematic review of clinical trials, observational studies, case reports, and FDA adverse event data to evaluate the incidence, mechanisms, and clinical outcomes of FCM-associated hypophosphatemia. The review found that hypophosphatemia is a clinically significant adverse drug reaction linked to FCM and occurring at higher rates than with other IV iron formulations: 50–92% with FCM compared to 2–8% with other agents. Across 42 clinical trials and real-world datasets, FCM induced a greater and longer-lasting drop in phosphate levels than FDI or ferumoxytol, with up to 45% of affected patients remaining hypophosphatemic for three months or longer. Analysis of FDA’s Adverse Event Reporting System (FAERS) database (2014–2023) identified 1270 reports of FCM-associated hypophosphatemia, with an increasing trend over time, though the authors estimated that <1% of actual cases had been reported.
Galigutta et al. [75] undertook a large pharmacovigilance analysis and systematic review to evaluate serious adverse events associated with FCM. Using data from FAERS and VigiBase between 2003 and 2024, the study found strong disproportionality signal linking FCM to hypophosphatemia (proportional reporting ratio [PRR] of 520.7 in FAERS and 245.1 in VigiBase). The literature review of 11 case reports confirmed these findings, describing cases of prolonged, severe hypophosphatemia, osteomalacia, and fractures, as well as occasional life-threatening hypersensitivity reactions.
3.2.2. Recommendations and Consensus Statements
Kassianides and Bhandari [22] examined IV-iron-induced hypophosphatemia and proposed a practical clinical algorithm to guide IV iron selection and hypophosphatemia management. They concluded that although modern IV iron formulations are generally safe and effective, FCM is associated with a distinct and higher risk of hypophosphatemia, warranting careful patient selection, biochemical monitoring, and consideration of alternative preparations in at-risk patients.
Boots and Quax [29] proposed evidence-based recommendations for the evaluation and management of hypophosphatemia in patients receiving IV iron. Their flowchart emphasized that, when FCM is used, the SmPC advises consideration of serum phosphate monitoring before administration and again after 14 days; however, because the nadir following a single FCM dose typically occurs at around 7 days, earlier monitoring is appropriate. The authors note that even patients deemed low risk may develop severe hypophosphatemia with FCM and suggest careful selection of the iron formulation. If iron deficiency cannot be corrected with a single 1000 mg dose and multiple infusions are expected, FCM may be unsuitable as repeated dosing can deepen and prolong hypophosphatemia and potentially increase the risk of osteomalacia. For patients at elevated risk, clinicians should consider formulations with lower reported hypophosphatemia risk than FCM, like iron sucrose, ferumoxytol, and FDI. Boots and Quax [29] further emphasized that prevention is preferable to treatment and that phosphate supplementation, oral or IV, should be reserved for clinically urgent situations due to its limited effectiveness and its potential adverse effects.
Schaefer et al. [32] provided diagnostic and management recommendations, emphasizing serum phosphate monitoring in patients requiring repeated or high-dose FCM or those with unexplained fatigue, bone pain, or muscular weakness. In affected patients, they recommend assessing calcium, PTH, alkaline phosphatase, and vitamin D metabolites, along with imaging studies to detect osteomalacia (e.g., looser zones on X-ray or scintigraphy). For prevention, clinicians are advised to delay additional FCM doses until recovery, consider switching to iron formulations with lower hypophosphatemia risk, and manage complications with active vitamin D analogs to mitigate secondary hyperparathyroidism.
Martens and Wolf [76] provided an evidence-based mini-review on the incidence, mechanism, and clinical management of IV-iron-induced hypophosphatemia, focusing on FCM as the principal cause. They outlined that FCM uniquely induced hypophosphatemia occurring in up to 75% of recipients through an acute three- to sixfold increase in FGF-23, which causes increased renal phosphate wasting, reduced 1,25-dihydroxyvitamin D synthesis, and secondary hyperparathyroidism. The article identified normal kidney function, severe iron deficiency, need for repeated doses of IV iron, low body weight, low baseline phosphate, and abnormal uterine bleeding as risk factors. Clinical symptoms can include fatigue, myalgia, bone pain, weakness, or “brain fog,” and chronic cases may progress to osteomalacia or fractures with repeated dosing of FCM. The authors provided management and prevention recommendations summarized in the algorithm (Figure 5). They advised avoiding FCM when alternative formulations such as ferumoxytol or FDI are available, particularly in patients requiring repeated infusions. When FCM use is unavoidable, they recommend serum phosphate testing at week 1 before administering a second dose, withholding treatment if phosphate levels are ≤0.65 mmol/L (or ≤2.0 mg/dL), and evaluating for hypophosphatemia in any patient presenting with fatigue, myalgia, or bone pain after infusion. The authors indicate that phosphate and vitamin D supplementation are often limited in effectiveness in the setting of ongoing FGF-23 excess, underscoring prevention and early detection as the most effective strategy.
Van Doren et al. [77] published an expert consensus guideline on the safe use, administration, and monitoring of IV iron formulations, focusing on the recognition and management of infusion reactions and treatment-emergent hypophosphatemia. With respect to hypophosphatemia, the consensus emphasizes that FCM poses the highest risk, with reported incidence rates between 47% and 75%, while other formulations, such as ferumoxytol, FDI, and LMWID are associated with a substantially lower risk of hypophosphatemia and rarely with clinically significant or persistent phosphate depletion. The authors recommend avoiding FCM in patients requiring repeated infusions or with chronic blood loss or malabsorptive disorders, as prolonged use can lead to osteomalacia and fractures. Routine phosphate monitoring is primarily recommended for FCM users, particularly prior to repeat dosing within three months, whereas other formulations warrant symptom-driven testing. Importantly, phosphate or vitamin D supplementation is largely ineffective, and management should focus on cessation of FCM and prevention of secondary hyperparathyroidism.
Fraser et al. [78] presented a nursing consensus paper that established 16 evidence-based recommendations on the practical management of infusion reactions and hypophosphatemia associated with IV iron therapy. The paper specifically provided recommendations on monitoring and prevention of hypophosphatemia. Nurses are advised to watch for fatigue [87], weakness, and bone pain that may develop days to weeks after infusion and to measure serum phosphate before and after treatment in patients at risk or receiving multiple doses of FCM.
Rosano et al. [79] presented an international multidisciplinary consensus on the risk assessment and management of hypophosphatemia associated with FCM. The expert panel, comprising specialists from cardiology, nephrology, hematology, endocrinology, and molecular biology, concluded that in many clinical settings, particularly cardiology populations, FCM-associated hypophosphatemia is often transient, asymptomatic, and self-limiting, typically resolving within eight weeks without specific intervention. However, the authors also acknowledged that the incidence of hypophosphatemia is higher with FCM than with other IV iron formulations and that recurrent or prolonged hypophosphatemia, especially with repeated dosing, may result in clinically relevant sequelae, including osteomalacia.
Compared with prior recommendations, including those of Martens and Wolf [76] and Van Doren et al. [77], and Rosano et al. [79], adopted a more selective approach to phosphate monitoring. Whereas Martens and Wolf [76] advocated routine serum phosphate testing approximately one week after FCM administration and avoidance of repeat dosing when phosphate levels are ≤0.65 mmol/L (or ≤2.0 mg/dL), Rosano et al. [79] recommended targeted testing primarily in high-risk or symptomatic individuals, and in patients requiring repeated or higher-dose infusions. In contrast to Van Doren et al. [77], who advised avoiding FCM in patients needing recurrent infusions, this consensus did not discourage its use outright but rather emphasized individualized risk assessment and the low incidence of serious sequelae such as osteomalacia. Overall, Rosano et al. [79] frame FCM as an effective therapy in many clinical settings and propose a less prescriptive framework for managing FCM-associated hypophosphatemia.
The Scandinavian expert consensus by Detlie et al. [80] recognized hypophosphatemia as a safety concern associated with IV iron therapy in patients with IDA and IBD. The panel highlighted the higher risk of hypophosphatemia with FCM compared with other formulations and supported consideration of FDI as an alternative, particularly when repeated dosing is anticipated.
4. Discussion
In this study, we evaluated the cost effectiveness of FDI versus FCM for treating IDA in patients with IBD within the Slovenian healthcare system. The pharmacoeconomic model showed that FDI remains cost effective and below the national ICER threshold even under a highly unfavorable pricing scenario in which FCM is priced at 42% of FDI. As described in the Methods section (Section 2), several clinically relevant consequences of hypophosphatemia, such as bone and muscle pain, or osteomalacia with (pseudo)fractures, were not incorporated into the model; their exclusion likely leads to an underestimation of the full clinical and economic impact of hypophosphatemia and therefore renders the analysis conservative.
Beyond the base modeling results, this work integrates pharmacoeconomic modeling with an umbrella review of systematic reviews and expert consensus statements. Together, these elements provide an up-to-date perspective that reflects Slovenia’s current cost environment and evolving clinical guidance on IV-iron-related hypophosphatemia. Slovenia may serve as an informative case example for CEE countries, given its advanced and transparent pharmaceutical reimbursement framework and broad market access to innovative therapies [55]. A similar evaluative approach can also be applied beyond pharmaceuticals, including to medical devices and emerging diagnostic technologies [88,89,90,91,92,93,94].
4.1. Economic Interpretation
The pharmacoeconomic modeling demonstrated that FDI remains cost effective compared with FCM despite Slovenia’s unusually low infusion costs and the recent substantial price reduction in FCM. The base-case ICER of €6590/QALY was below the national WTP threshold of €25,000/QALY, indicating that FDI provides value for money even under conservative modeling assumptions. When FCM was modeled at zero acquisition cost, the ICER increased to €12,669/QALY yet remained cost effective, underscoring the robustness of results across price scenarios. However, it should be acknowledged that the markedly lower price of FCM compared with FDI makes it highly appealing from a short-term hospital budget perspective, where tender decisions are typically driven by unit acquisition price rather than formal cost-effectiveness criteria [95]. In this context, procurement processes emphasize immediate budgetary impact over long-term clinical or economic value, such that lower-cost options are favored even when they entail higher downstream risks or monitoring requirements. This dynamic highlights the value of structured health technology assessment (HTA) approaches within hospital decision-making to ensure that considerations of safety, resource use, and patient outcomes are not overshadowed by unit-price pressures [95].
Our findings contrast with previous analyses in Western Europe [48,49,50,96], where higher infusion costs combined with more comparable pricing of FDI and FCM amplified the economic advantage of FDI. In the Slovenian setting, the substantial cost differential between the two drugs outweighed the minor savings associated with fewer infusions required for FDI. Nevertheless, because the model explicitly incorporated the health-related quality-of-life impact of hypophosphatemia, FDI remained the cost-effective option. An important area for future refinement is the treatment of hypophosphatemia within the model. Hypophosphatemia varies widely in severity and duration, and accounting for the transient nature of the condition and its spectrum of severity would improve the accuracy of the model.
4.2. Clinical Evidence and Recommendations
The umbrella review of systematic literature reviews and consensus statements confirmed marked differences in the incidence of hypophosphatemia between IV iron formulations. According to studies, FCM exhibited the highest reported incidence (up to 92%), whereas other preparations, such as ferumoxytol, LMWID, and FDI generally demonstrated rates below 10%. Severe or persistent hypophosphatemia following FCM has been associated with clinically relevant sequelae, including osteomalacia, fractures, or chronic fatigue, largely attributable to FGF-23-mediated renal phosphate wasting and secondary hyperparathyroidism. While many cases are transient and reversible, prolonged exposure or repeated dosing has been associated with sustained metabolic disturbances. With the exception of the more permissive consensus by Rosano et al. [79], expert recommendations have been broadly consistent over recent years [32,76,77,78,80]. These recommendations generally support routine post-FCM serum phosphate testing, particularly prior to repeat dosing, and the avoidance of additional FCM administration when phosphate levels are ≤0.65 mmol/L (≤2.0 mg/dL), as well as discouraging the use of FCM in patients requiring frequent or long-term infusions.
4.3. Potential Clinical Consideration
A potential clinical consideration is whether patients should undergo baseline serum phosphate testing before IV iron administration. A subset of individuals with IBD, particularly those with active disease or ongoing inflammation, may already have hypophosphatemia prior to infusion and identifying such patients in advance may help prevent exacerbation or prolongation of phosphate depletion following IV iron therapy.
4.4. Comparison with Other Umbrella Reviews
Netzer et al. [97] provided a comprehensive synthesis of evidence on phosphate testing and supplementation in adults outside intensive care settings across a range of clinical conditions, such as X-linked hypophosphatemia, tumor-induced osteomalacia, and post-kidney-transplantation states. Among the 33 publications reviewed (11 guidelines, 19 reviews, 3 consensus statements), only three specifically addressed hypophosphatemia associated with FCM [29,32,72]. All three of these publications were included in the present review.
4.5. Limitations
Several limitations should be acknowledged. Pharmacoeconomic analysis was conducted from the payer perspective and did not include indirect costs, such as productivity loss, to maintain a conservative approach. Similarly, fracture-related outcomes were excluded from the model, likely underestimating the long-term burden of severe hypophosphatemia. Evidence on the long-term clinical consequences of phosphate depletion remains limited, highlighting the need for further prospective and retrospective studies, to refine future cost-effectiveness estimates.
Certain model inputs and assumptions relied exclusively on findings from the PHOSPHARE-IBD study, which may introduce a potential source of bias. In particular, the assumption of equivalent hematological responses and comparable hemoglobin increases between FDI and FCM was derived directly from PHOSPHARE-IBD. The umbrella review also has methodological limitations, as it relied on a narrative synthesis rather than a quantitative meta-analysis. This approach was deliberately chosen to accommodate the umbrella review format, which encompassed both systematic reviews and expert recommendations or consensus statements. This allowed the integration of diverse sources of evidence while maintaining transparency and breadth. It is important to note that all limitations of the studies included in the umbrella review also apply to the present analysis. Finally, patient and public involvement in disease assessment has until recently received limited attention [98]. Systematic inclusion of patient perspectives could further strengthen our study, improve alignment with patient needs, and enhance overall societal relevance.
5. Conclusions
In summary, this modeling study showed that FDI remains a cost-effective alternative to FCM for treating IDA in patients with IBD within the Slovenian healthcare setting, primarily due to its more favorable hypophosphatemia profile within the model. The finding suggests that the risk of hypophosphatemia should be considered when selecting IV iron therapy in routine IBD care.
Our analysis emphasizes that hypophosphatemia remains an underrecognized yet clinically meaningful adverse effect of IV iron therapy. Its symptoms, such as fatigue, muscle weakness, and dyspnea, may closely resemble those of untreated anemia, potentially leading to delayed recognition and management. Particular caution is warranted in patients with osteoporosis, vitamin D deficiency, malabsorptive conditions, or in those requiring repeated or high-dose FCM infusions, as these populations are at increased risk of clinically relevant phosphate depletion. In cases of severe or persistent hypophosphatemia, referral to specialists in bone metabolism may be appropriate to manage complications such as osteomalacia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jimenez K.M. Gasche C. Management of Iron Deficiency Anaemia in Inflammatory Bowel Disease Acta Haematol.2019142303610.1159/00049672830970351 · doi ↗ · pubmed ↗
- 2Pasricha S.-R. Tye-Din J. Muckenthaler M.U. Swinkels D.W. Iron deficiency Lancet 202139723324810.1016/S 0140-6736(20)32594-033285139 · doi ↗ · pubmed ↗
- 3Ershler W.B. Chen K. Reyes E.B. Dubois R. Economic Burden of Patients with Anemia in Selected Diseases Value Health 2005862963810.1111/j.1524-4733.2005.00058.x 16283863 · doi ↗ · pubmed ↗
- 4Dignass A.U. Gasche C. Bettenworth D. Birgegård G. Danese S. Gisbert J.P. Gomollon F. Iqbal T. Katsanos K. Koutroubakis I. European Consensus on the Diagnosis and Management of Iron Deficiency and Anaemia in Inflammatory Bowel Diseases J. Crohn’s Colitis 2015921122210.1093/ecco-jcc/jju 00925518052 · doi ↗ · pubmed ↗
- 5Gordon H. Burisch J. Ellul P. Karmiris K. Katsanos K. Allocca M. Bamias G. Barreiro-de Acosta M. Braithwaite T. Greuter T. ECCO Guidelines on Extraintestinal Manifestations in Inflammatory Bowel Disease J. Crohn’s Colitis 20241813710.1093/ecco-jcc/jjad 10837351850 · doi ↗ · pubmed ↗
- 6Fiorino G. Colombel J.F. Katsanos K. Mearin F. Stein J. Andretta M. Antonacci S. Arenare L. Citraro R. Dell’Orco S. Iron therapy supplementation in inflammatory bowel disease patients with iron deficiency anemia: Findings from a real-world analysis in Italy Eur. J. Gastroenterol. Hepatol.20243656357010.1097/MEG.000000000000274038477856 PMC 10965121 · doi ↗ · pubmed ↗
- 7Erichsen K. Hausken T. Ulvik R.J. Svardal A. Berstad A. Berge R.K. Ferrous Fumarate Deteriorated Plasma Antioxidant Status in Patients with Crohn Disease Scand. J. Gastroenterol.20033854354810.1080/0036552031000077112795468 · doi ↗ · pubmed ↗
- 8Auerbach M. Wolf M. Intravenous Iron Associated Hypophosphatemia: Much More Than a Laboratory Curiosity Am. J. Hematol.202510075275410.1002/ajh.2759939821908 · doi ↗ · pubmed ↗