Calcinosis Cutis Universalis: A Review of Therapeutic Strategies and Surgical Management
Emma Giacometti, Jérôme Martineau, Ilias G. Petrou, Daniel F. Kalbermatten, Matteo Scampa

TL;DR
This review discusses treatment options for calcinosis cutis universalis, a rare condition causing calcium deposits in the skin, and proposes a stepwise approach combining medical and surgical strategies.
Contribution
The paper proposes a stepwise therapeutic algorithm integrating medical, minimally invasive, and surgical approaches for managing calcinosis cutis universalis.
Findings
Pharmacological treatments show variable and often partial efficacy, especially in early or localized disease.
Surgical interventions provide meaningful relief in selected patients but are associated with risks.
A multimodal and individualized strategy is essential for managing this condition.
Abstract
Background/Objectives: Calcinosis cutis universalis is a rare and severe manifestation of dystrophic calcification, most associated with connective tissue diseases such as dermatomyositis, systemic sclerosis, and systemic lupus erythematosus. It is characterized by widespread deposition of calcium salts throughout the soft tissues, leading to pain, recurrent infections, restricted mobility, and significant impairment in daily functioning and quality of life. Management remains challenging due to the absence of standardized treatment guidelines with risks including delayed wound healing and recurrence. Adjunctive therapies may support symptom control in refractory cases. Conclusions: Management of calcinosis cutis universalis requires an individualized, multimodal strategy. Based on available evidence and expert opinion, a stepwise therapeutic decision-making algorithm integrating…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
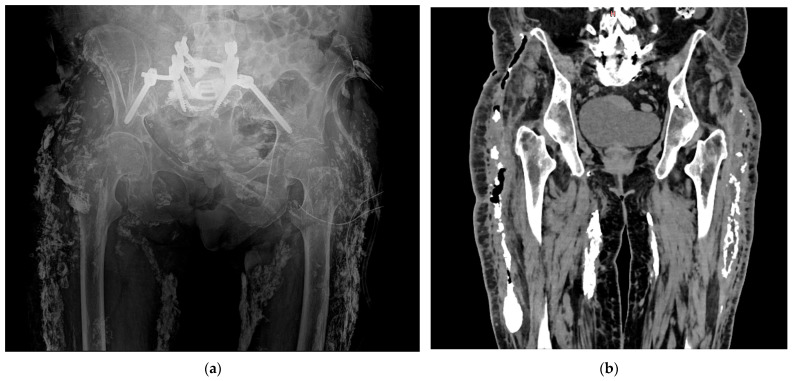 Figure 1
Figure 1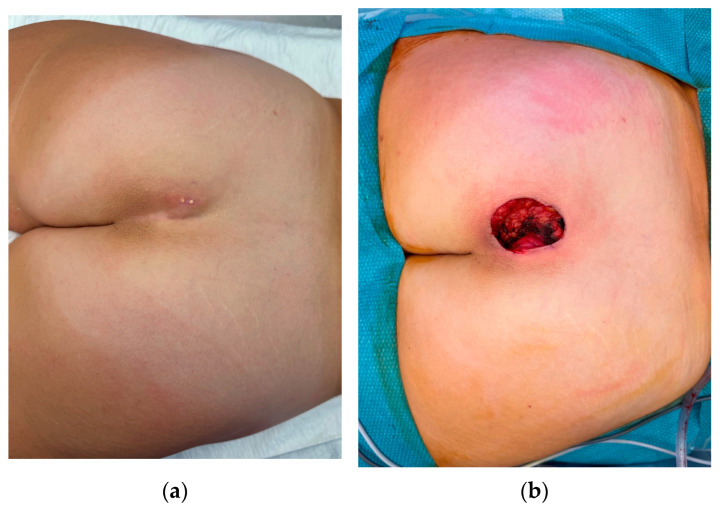 Figure 2
Figure 2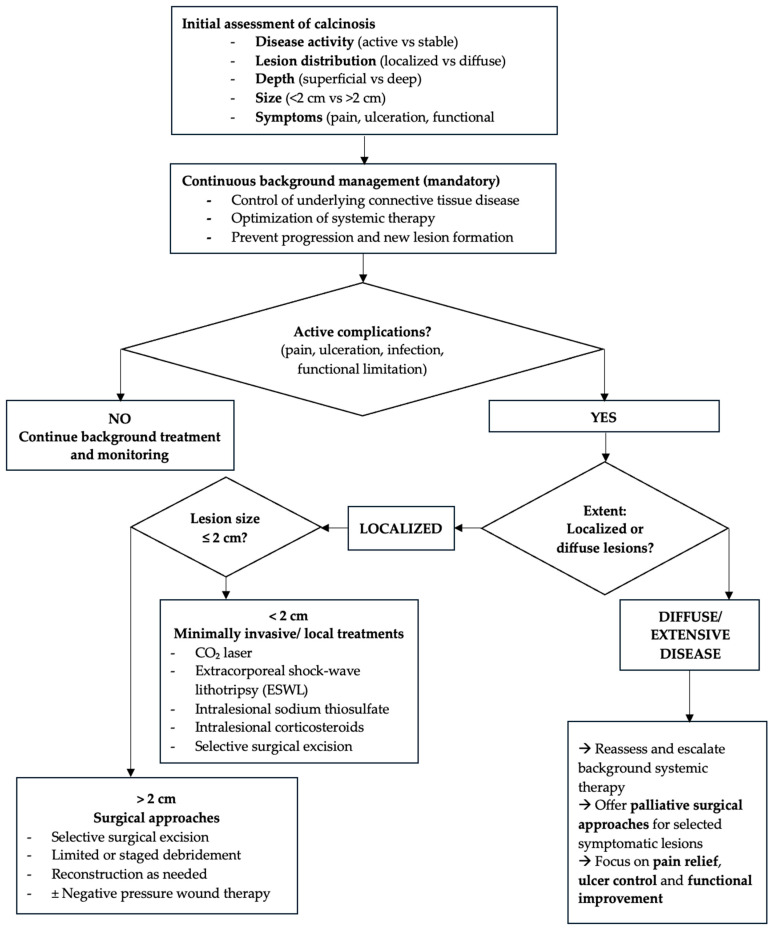 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory Myopathies and Dermatomyositis · Heterotopic Ossification and Related Conditions · Systemic Sclerosis and Related Diseases
1. Introduction
First described by Virchow in 1855, calcinosis cutis may present either in a localized form, known as calcinosis cutis circumscripta, or in a more generalized and disseminated pattern called calcinosis cutis universalis (Figure 1) [1]. Calcinosis cutis universalis is characterized by widespread deposition of calcium salts in subcutaneous tissues, fibrous muscle structures, fascial planes, and tendons [2]. There is currently no consensus on how to classify calcinosis cutis by size, but across the literature small lesions are typically defined as less than 1 cm and confined to superficial layers, while large or deep lesions are generally considered those with a diameter greater than 2 cm and/or extension into deeper tissues such as tendon or muscle [3].
Calcinosis cutis is classified into five subtypes based on the distinct underlying pathophysiological mechanisms: metastatic, dystrophic, idiopathic, iatrogenic and calciphylaxis [4]. Among patients with connective tissue diseases, the dystrophic subtype is the most frequent, occurring despite normal serum calcium and phosphate levels [5]. Calcinosis cutis universalis is a rare manifestation within this dystrophic category and is distinct from calciphylaxis, a severe and often fatal condition [6].
While calcinosis cutis universalis involves diffuse calcium deposits in soft tissues without vascular involvement, calciphylaxis is characterized by calcification of small- and medium-sized dermal arteries, leading to ischemia, painful skin ulcers, and necrosis. It primarily affects patients with end-stage renal disease and carries a high risk of sepsis and death [7].
The pathogenesis of dystrophic calcification involves cellular injury, due to connective tissue diseases or multiple traumas, inducing the release of phosphate-binding proteins from necrotic cells [8]. These proteins bind to free phosphate, facilitating the formation and deposition of insoluble calcium salts. In addition, the ongoing tissue damage provokes chronic inflammation and vascular hypoxia, worsening local tissue stress and calcific deposition. The resulting deposits are primarily composed of hydroxyapatite and amorphous calcium phosphate [4].
Multiple theories have been proposed to explain the development of dystrophic calcinosis, though its exact cause remains unclear. It is commonly believed to be linked to skin that is damaged, inflamed or necrotic [5]. Calcinosis cutis universalis typically arises secondary to connective tissue diseases such as dermatomyositis, systemic sclerosis, systemic lupus erythematosus, or Sjögren’s syndrome, all causing chronic tissue injury that can lead to pathological calcification [4]. Onset typically occurs within the first two decades of life, most commonly before the age of 20, and predominantly affects females [9].
Clinically, calcium deposits most often appear as subcutaneous nodules in areas exposed to repeated minor trauma, particularly the fingers, elbows, knees, and buttocks [10]. Symptoms can range from mild arthralgia to significant movement restriction, depending on the location and volume of calcium deposits [11]. Dystrophic calcifications are often painful, especially when located near joints or in cases of ulceration [12]. In contrast, muscle calcifications tend to be asymptomatic and are typically discovered incidentally through imaging studies [5]. Chronic ulceration may occur, leading to the drainage of calcific material, which can become secondarily infected or colonized by bacteria, resulting in persistent or recurrent infections [13].
The management of calcinosis cutis remains a considerable challenge and typically requires a multifaceted approach [4]. Most therapeutic recommendations stem from isolated case reports and small series, while randomized controlled trials are notably lacking. A wide range of pharmacologic agents has been proposed with the aim of reducing calcium deposition or preventing further progression of the disease [14]. Given the marked interindividual variability in treatment response, sequential and individualized therapeutic strategies are likely to offer the best chance of clinical benefit [8]. Alongside pharmaceutical therapies, supportive strategies, such as minimizing local trauma, smoking cessation, stress reduction, and avoidance of cold exposure, help improve peripheral blood flow and play an important role in disease management [4].
This narrative review outlines current treatments for calcinosis cutis, covering both surgical and nonsurgical options. Due to the limited literature on calcinosis universalis specifically, we included studies on all forms of calcinosis cutis to provide a comprehensive overview.
2. Methods
This narrative review was conducted through a literature search of PubMed and Google Scholar. Search terms included combinations of “calcinosis cutis universalis”, “connective tissue disease”, “treatment”, “surgery”, and “management”, using Boolean operators. Additional relevant publications were identified through manual screening of the reference lists of selected articles. Given the rarity of calcinosis cutis universalis and the predominance of case reports and small case series, a narrative approach was chosen to synthesize available evidence.
3. Treatments
3.1. Pharmacological Treatments
3.1.1. Vitamin K Antagonists
Warfarin, a vitamin K antagonist, has been investigated for its potential to reduce calcinosis by inhibiting vitamin K-dependent gamma-carboxylation of matrix Gla protein, thereby preventing calcification [14]. Clinical benefit has been observed primarily in patients with small, recent lesions. Cukierman et al. reported improvement in two of three systemic sclerosis patients treated with low-dose warfarin (1 mg/day), and Yoshida & Torikai described radiographic improvement in fingertip calcinosis [15,16]. In contrast, Lassoued et al. found no benefit in patients with long-standing diffuse calcinosis [17]. Overall, warfarin has shown inconsistent and generally limited efficacy in calcinosis cutis, including severe and extensive forms [18]. Overall, low-dose warfarin appears safe and well tolerated, without bleeding complications, but efficacy is limited to early or localized disease [19] (see Table A1).
Evidence supporting the use of low-dose warfarin in calcinosis cutis is limited to isolated case reports and very small case series, with conflicting results, and therefore represents a low level of evidence.
3.1.2. Bisphosphonates
Bisphosphonates target macrophages and reduce calcium turnover, potentially stabilizing or regressing calcified lesions [14]. Clinical outcomes are heterogeneous, with Rauch et al. reporting subjective and radiographic improvement with intravenous pamidronate, while Mukamel et al. observed complete resolution of calcinosis in juvenile dermatomyositis with alendronate [20,21]. Although generally well tolerated, bisphosphonates can cause osteonecrosis of the jaw, gastrointestinal symptoms, and electrolyte disturbances. Their use is most appropriate in refractory, painful, or functionally limiting cases [21].
Overall, evidence supporting the use of bisphosphonates in calcinosis cutis remains limited to retrospective observational studies—including a study of 7 patients—and isolated case reports, corresponding to a low level of evidence (see Table A2).
3.1.3. Antibiotics
Tetracycline antibiotics, particularly minocycline, have been investigated in calcinosis for their therapeutic effects beyond antimicrobial activity, including calcium chelation, matrix metalloproteinase inhibition, and anti-inflammatory actions [22]. Robertson et al. reported clinical improvement in 8 of 9 patients with limited systemic sclerosis [23]. Nevertheless, efficacy has not been consistently reproduced [24]. Minocycline is generally well tolerated, with minor gastrointestinal side effects and occasional pigmentation of calcified lesions or teeth [23]. Importantly, long-term tetracycline treatment increases the risk of antibiotic resistance by selecting resistant strains and promoting resistant genes emergence, potentially persisting even after antibiotic discontinuation [25] (see Table A3).
In contrast, evidence for cephalosporins is minimal. A single case report described marked improvement of calcinosis cutis in a patient with morphea profunda after a 20-day course of intravenous ceftriaxone, possibly related to calcium binding and matrix metalloproteinase inhibition [26]. However, the role of ceftriaxone remains uncertain, and potential adverse effects include antibiotic resistance, biliary sludge and nephrolithiasis due to calcium-ceftriaxone precipitation [14] (see Table A4).
Evidence for antibiotic use in calcinosis cutis universalis is low, mainly extrapolated from low-level data from connective tissue disease–associated subtypes, such as systemic sclerosis and juvenile dermatomyositis, and isolated case reports.
3.1.4. Calcium Channel Blockers
Diltiazem, a non-dihydropyridine calcium channel blocker, has been widely used for calcinosis, particularly in systemic sclerosis [24]. It is hypothesized to reduce intracellular calcium in macrophages and improve tissue oxygenation, thereby mitigating calcification [8]. Case reports describe partial to significant improvement [27,28,29]. A larger observational study on 47 patients with systemic sclerosis have failed to confirm consistent efficacy [30]. Effective doses typically range from 240 to 480 mg/day [27]. Hypotension and edema are the main adverse effects [19].
Evidence supporting the use of diltiazem in calcinosis cutis universalis is limited to observational data, primarily derived from case reports and small observational studies in connective tissue disease-associated calcinosis—most commonly systemic sclerosis with localized digital involvement—with inconsistent efficacy reported (see Table A5).
3.1.5. Phosphate Binders
Aluminum hydroxide, an antacid with phosphate-binding properties, has been employed in dystrophic calcinosis, particularly in juvenile dermatomyositis, systemic lupus erythematosus, and idiopathic forms. By reducing intestinal phosphate absorption, it decreases calcium-phosphate precipitation [31,32]. The therapy is generally well tolerated, though caution is advised in renal insufficiency due to the risk of aluminum accumulation [14].
Available evidence remains limited to isolated case reports and small series, which describe regression of calcifications and improvement in mobility (see Table A6).
3.1.6. Uricosuric Agents
Probenecid, a sulfonamide derivative with uricosuric properties, increases renal phosphate clearance by inhibiting tubular phosphate reabsorption, thereby lowering serum phosphorus and reducing the calcium–phosphorus product [33]. This mechanism is thought to both prevent new calcification and promote regression of existing deposits. Clinical experience, mainly from case reports, has shown promising results in juvenile dermatomyositis (JDM) and calcinosis universalis. Harel et al. reported dramatic improvement in JDM with normalization of phosphorus and reduction in calcified deposits, while additional reports described regression of subcutaneous and intermuscular calcinosis and functional recovery in calcinosis universalis [33,34]. Nakamura et al. further demonstrated efficacy in resistant JDM, with restoration of joint mobility after prolonged treatment [35]. The drug is generally well tolerated, with only occasional rash or diarrhea reported [19]. Given its safety and oral use, probenecid represents a useful adjunct treatment when standard therapies fail.
Overall, evidence for probenecid in calcinosis cutis universalis is limited to low-level observational data derived from isolated case reports, mainly in juvenile dermatomyositis and rare cases of calcinosis cutis universalis, with no controlled studies available (see Table A7).
3.1.7. Intravenous Immunoglobulin (IVIG)
IVIG, an immunomodulatory preparation of pooled antibodies, modulates inflammation through multiple pathways, including macrophage suppression, cytokine regulation, and complement inhibition [36]. It has been used in refractory cases of dystrophic calcinosis cutis, calcinosis universalis, and ulcerated forms [37]. Clinical outcomes vary: marked regression and ulcer healing have been reported [36,37,38], while no benefit was observed in long-standing disease [39]. IVIG is generally well tolerated, with only mild side effects such as headache noted [38]. Despite high cost and variable efficacy, IVIG may benefit patients with severe, refractory, or steroid-resistant calcinosis, unresponsive to immunosuppressive regimens [38,40].
Evidence for intravenous immunoglobulin in calcinosis cutis universalis is also limited to low-level observational data from isolated case reports and small case series, mainly in dermatomyositis-associated calcinosis and occasional cases of calcinosis cutis universalis, with heterogeneous clinical outcomes reported (see Table A8).
3.1.8. Intralesional Corticosteroids
Intralesional corticosteroid injections, most often with triamcinolone, have been explored in localized calcinosis cutis. Their proposed benefit derives from suppression of local inflammatory responses and inhibition of fibroblast activity [8]. Several reports describe regression of nodules, improved mobility, pain relief, and ulcer healing [41]. While intralesional therapy is generally well tolerated, rare paradoxical induction of calcinosis has been documented [42], probably due to local tissue damage [43]. This approach provides targeted anti-inflammatory benefit with minimal systemic exposure, making it a practical option for accessible and symptomatic lesions unresponsive to systemic treatment [44].
Evidence for intralesional corticosteroids in calcinosis cutis universalis is limited to low-level observational data from isolated case reports, mainly in localized disease (see Table A9).
3.1.9. Calcium-Chelating Agents
Sodium thiosulfate (STS), an inorganic salt with calcium-chelating and antioxidant properties, has been widely studied in calcinosis cutis [8,22]. Topical STS has shown good effectiveness in case series, with reported improvement rates ranging from 68% to 78%, including cases of complete resolution [45,46]. Intralesional injections show partial benefit in small lesions: lesions measuring up to 0.2 cm respond best to topical treatment, whereas those up to 2 cm are more effectively managed with intradermal injections [47]. Intravenous STS has yielded disappointing outcomes in advanced or widespread calcinosis [48]. Tolerance is excellent with topical or localized administration, while systemic delivery carries more side effects, such as moderate gastrointestinal disturbance [48]. Overall, STS is best suited for mild-to-moderate localized lesions.
Evidence supporting the use of STS in calcinosis cutis universalis is derived from low- to moderate-level observational data, including case series and retrospective cohorts—primarily involving disease-associated connective tissue—with consistent benefit reported for topical and intralesional administration (see Table A10).
3.1.10. Colchicine
Colchicine, an antigout drug with anti-inflammatory activity through microtubule inhibition [8], has been reported in isolated cases of calcinosis cutis. Colchicine has been reported in isolated case reports of calcinosis cutis, where it appears to reduce inflammation and pain and promote healing of ulcerated lesions, without consistent effects on calcified deposits. Evidence remains limited to observational studies [49,50,51] (see Table A11).
3.1.11. Biologic Therapies
Anti-CD20 Monoclonal Antibody
Rituximab, an anti-CD20 monoclonal antibody, depletes B cells through antibody-dependent and complement-mediated cytotoxicity, therefore reducing autoantibody production. Its efficacy in calcinosis cutis is mixed: partial responses have been reported in JDM [52], whereas patients with systemic sclerosis or CREST syndrome experienced more significant regression of calcinosis [53,54]. Rituximab is generally well tolerated, though mild infections at calcinosis sites have been described [52]. Rituximab may be considered in refractory calcinosis associated with autoimmune connective tissue disease, particularly when other immunosuppressants fail.
Evidence for rituximab in calcinosis cutis universalis is limited to low-level observational data from small case series and isolated case reports, with variable efficacy across disease subtypes (see Table A12).
Anti-TNF-α Monoclonal Antibody
Infliximab, a TNF-α inhibitor, has been explored in refractory calcinosis associated with juvenile dermatomyositis and overlap syndromes, though evidence remains confined to isolated case reports and very small series [55,56]. Intravenously is the route of administration described in the medical literature and case reports for infliximab when used to treat calcinosis cutis, Riley et al. reported clinical benefit with systemic dosing at 6 mg/kg every four weeks, leading to improved muscle strength, pain relief, and regression of calcinosis [55]. More recently, Shiari et al. described an alternative approach using intralesional injections of 25 mg once weekly for six weeks, directly targeting calcified lesions [56]. Treatment was generally well tolerated in these reports, with infections rarely observed [55]. Despite promising clinical outcomes, infliximab use is limited by its high cost, an issue common to all biologic therapies and long-term treatment requirements. It may be especially valuable in aggressive or treatment-resistant cases.
Overall, available evidence supporting the use of infliximab in calcinosis cutis unviersalis remains limited to low-level observational data and small uncontrolled studies, with reported benefit mainly in refractory, autoimmune-associated cases (see Table A13).
3.1.12. Immunomodulatory Agents
Thalidomide, an immunomodulatory drug that reduces TNF-α and IL-6 production, has been reported in a single case of severe, treatment-refractory JDM with calcinosis. Therapy led to resolution of systemic inflammation, pain, and fever, although calcific deposits persisted. The treatment was well tolerated in this case [57].
Evidence for thalidomide in calcinosis cutis universalis remains anecdotal, limited to one case report; nevertheless, despite important safety considerations, it may represent an option worth considering in highly selected, treatment-resistant cases (see Table A14).
3.1.13. JAK Inhibitors
Janus kinase (JAK) inhibitors are targeted small-molecule immunomodulators that block JAK–STAT–mediated cytokine and interferon signaling. In dermatomyositis, this pathway is implicated in disease activity and may contribute to calcification through altered calcium handling [58]. Clinical experience with JAK inhibitors in calcinosis cutis remains limited but encouraging, primarily in refractory dermatomyositis (DM) and juvenile dermatomyositis (JDM).
Tofacitinib has been reported in two adult DM patients with extensive calcifications, showing rapid and sustained clinical response, stabilization or regression of lesions, absence of new calcifications over 28 weeks, and functional improvement [58]. Ruxolitinib has been described in a pediatric patient with severe MDA5-positive JDM, with resolution of skin lesions and disappearance of clinical signs of calcinosis in the affected region [59]. Baricitinib has also been reported in a child with refractory JDM, where progressive softening of calcium deposits and functional improvement occurred after its introduction within a combined therapeutic regimen [60].
Overall tolerance was acceptable in reported cases, with no major safety concerns, although all uses were off-label and involved very small patient numbers [58,59,60]. JAK inhibitors may represent a promising option for severe, refractory calcinosis associated with DM or JDM; however, evidence is limited to isolated case reports and very small case series, and their role in calcinosis cutis universalis remains unestablished (see Table A15).
3.2. Surgical Treatments
Excision of calcium deposits can be technically demanding, especially when complicated by lesion location, extension or underlying connective tissue disease [61]. Proper evaluation is essential, as calcinosis is occurring in up to 10% of patients with systemic sclerosis, 20% in adult patients with dermatomyositis and 10–40% of those with JDM, but is less frequent in systemic lupus erythematosus [62,63]. A comprehensive connective tissue disease workup is recommended, as these conditions represent the most common etiologies and directly influence prognosis, therapeutic choices, and surgical risk, given that underlying disease activity can impair wound healing and postoperative outcomes [64].
3.2.1. Surgical Indications
Surgical intervention in calcinosis cutis is primarily indicated in cases of painful masses, recurrent infections, ulcerations, functional impairment, limited range of motion, discomfort, or cosmetic concerns [65]. Across connective tissue diseases, including systemic sclerosis, dermatomyositis, JDM, systemic lupus erythematosus, and idiopathic forms, surgery is often pursued when conservative medical treatments fail to provide relief. Although not curative, surgery is particularly justified when lesion-related symptoms significantly interfere with daily function or pose a risk of systemic infection. Reviews further confirm that well-selected surgical cases, especially those with localized deposits and manageable wound healing risk, often result in rapid pain relief, improved function, and reduced infection burden [15,66,67]. Surgical trauma may provoke additional inflammation and tissue injury, stimulating further calcium deposition, so excision should be reserved for select, symptomatic cases when alternatives are limited, given the risk of lesion worsening and high recurrence [32].
3.2.2. Surgical Contraindications
Despite its benefits, surgical management is not without limitations. Several contraindications and precautions must be considered. Deep-seated calcifications involving vital structures, such as vessels, nerves or tendons, pose a higher surgical risk, particularly in functionally critical areas like the fingers [8]. Radical excision may compromise tissue viability or result in significant loss of function. Recalcification at previously treated sites is also a concern, potentially reducing the long-term success of surgery. In systemic diseases like scleroderma, microvascular pathology increases the risk of poor wound healing, as noted by Melone et al. [68], leading some clinicians to avoid surgery unless absolutely necessary. In general, small calcified deposits like plaques or nodules (<2 cm) or larger but localized lesions (deep deposits or calcinosis universalis) respond best to surgical intervention [14,22].
3.2.3. Surgical Techniques
Several surgical techniques have been described for the management of calcinosis cutis, chosen according to lesion size, depth, and anatomical constraints. Excision and debridement remain the most common approach, offering rapid symptom relief for localized lesions, although the ability of this approach in halting disease progression remains uncertain (Figure 2a,b) [66,69,70]. However, when deposits are large, deep, or close to critical structures such as tendons, vessels, or nerves, the priority is to preserve both function, tissue integrity and avoid exposure [66]. In these situations, reconstructive techniques are essential. In more limited lesions, simple outpatient debridement can be sufficient [71]. Minimally invasive methods such as CO_2_ laser excision, curettage, or high-speed burr debridement have also been recommended to reduce trauma and promote faster healing in patients with compromised vascularity [14,22,63]. An additional refinement is the use of pulsed irrigation fluid, which facilitates the removal of calcific debris while minimizing dermal trauma and preserving microvascular circulation, thereby decreasing the risk of wound complications [69]. In JDM, techniques such as incision and drainage or broaching have been successfully employed to relieve pain and restore mobility, even when complete removal was not feasible [67,72]. Overall, the choice of surgical technique should balance radical removal of calcifications with preservation of function and tissue viability, tailoring the approach to lesion location and systemic disease context. Building on concepts described in other similar conditions, future research should investigate staged surgical excision combined with dermal substitutes and carefully planned reconstructive strategies using concealed donor sites, aiming to improve functional outcomes, reduce recurrence, and address the often-overlooked aesthetic burden of calcinosis cutis [73]. Emerging evidence suggests that combining surgery with adjunctive measures, such as negative pressure wound therapy, may further enhance postoperative healing, reduce infection risk, and minimize recurrence in complex or refractory cases [74].
3.2.4. Complications
Surgical management of calcinosis cutis carries risk of complications that must be carefully considered before surgery, including local tissue damage, particularly involving digital neurovascular bundles, recurrence of calcific deposits and wound-related issues such as infection and hematoma formation [65,69]. Patients with widespread disease who are receiving long-term corticosteroids are at increased risk of wound healing issues, necessitating prolonged immobilization and elevation; staged excisions may be preferable [69]. Additional complications reported in the literature include skin necrosis and reduced joint mobility following wide excisions, particularly in systemic sclerosis patients with poor vascular supply [75]. When calcifications are deep and involve critical structures such as nerves, blood vessels, or tendons, excision may lead to functional impairment or significant tissue loss [66]. Importantly, recurrence of deposits is a well-recognized long-term issue, particularly in systemic diseases such as scleroderma or dermatomyositis, where ongoing disease activity promotes recalcification [14,63]. These complications can be mitigated by proper patient selection and meticulous surgical technique, including gentle handling of skin flaps, excision of devascularized edges, complete hemostasis with adequate drainage, tension-free closure, and protective splinting to reduce wound stress [69]. Despite these challenges, carefully planned surgery remains a valuable option, offering pain relief and functional improvement.
3.2.5. Recurrence After Surgical Treatment
Although surgical excision is often effective for symptom relief, recurrence of calcium deposits remains a concern [14]. Mendelson et al. observed that while most patients experienced symptom relief following excision, minor recurrences were common, though they did not typically impair the overall functional gains achieved [69]. In Mendelson et al. series, most patients benefited from excision, but recurrence sometimes required reoperation, as in one case where new calcified nodules reappeared within three months, necessitating further surgery. Merlino et al. acknowledged the risk of recurrence in digital calcinosis but emphasized that careful surgical planning, particularly using flap reconstruction, may reduce this likelihood and obviate the need for further procedures [66]. In idiopathic cases, Guermazi et al. noted that local recurrence is not uncommon, yet surgery still provided significant symptom relief [76]. Different reviews corroborate that recurrence is a frequent concern, especially in systemic conditions like scleroderma or dermatomyositis, where ongoing disease activity may drive re-calcification [14,63,65]. Nonetheless, authors mention that recurrence risk does not preclude surgery or re-excision, and repeated debridement remain appropriate options when recurrence leads to renewed pain or functional impairment.
3.2.6. Postoperative Outcomes
Postoperative outcomes following surgical excision of calcinosis cutis are generally favorable in terms of symptom control, though the long-term results remain variable. Mendelson et al. reported that most patients experienced significant symptomatic relief, with improved hand function and quality of life, even though surgery did not alter the underlying disease or the tendency to form new calcifications [69]. Merlino et al. similarly observed that radical debridement with vascularized flap reconstruction, particularly using Foucher’s kite flap, restored thumb mobility and grip strength with complete resolution of pain, although no data on recurrence was provided [66]. However, the literature agrees that surgery typically provides palliative rather than curative benefit, as recurrence is frequent and outcomes depend heavily on the disease context [14,63,65]. Nonetheless, even when relapse occurs, excision often translates into periods of pain-free function and improved daily activity, underscoring its value as a management option in selected patients.
3.3. Alternatives to Systemic Treatment and Surgical Excision
3.3.1. Extracorporeal Shock-Wave Lithotripsy (ESWL)
ESWL a technique long used for kidney stones, has shown promising results in treating calcinosis cutis, primarily by reducing pain and improving quality of life [61]. According to Sultan-Bichat et al., ESWL significantly decreased pain scores and analgesic use in patients with refractory calcinosis, particularly in small (<2 cm), ulcerated, radiopaque lesions [61]. Grechin et al. observed long-term remission, reduced infections, and improved patient well-being over five years of treatment [77]. Nowaczyk et al., in a systematic review, confirmed ESWL’s potential but highlighted the limited evidence base, mostly from small, uncontrolled studies [70]. Current evidence supports ESWL as a safe, well-tolerated, non-invasive palliative option for pain control in treatment-resistant calcinosis cutis lesions ≤ 2 cm, particularly as an opioid-sparing strategy. However, larger controlled trials are needed to establish standardized protocols and confirm long-term efficacy.
3.3.2. Laser CO2
CO_2_ laser therapy has been successfully used for superficial, localized calcinosis, offering surgical precision with less bleeding, faster healing, and good cosmetic outcomes [8,70]. Typically, a single session is sufficient to completely remove superficial and small calcifications up to 2 cm [19]. CO_2_ laser carries a lower risk of recurrence compared with conventional excision, specifically based on small lesions up to 2 cm [70]. Chamberlain and Walker reported pain relief and partial remission in CREST syndrome, while Bottomley et al. treated 21 digital lesions in systemic sclerosis with complete relief in 12, partial in 5, no improvement in 2, and only two recurrences, with healing in 4–10 weeks [78,79]. In systemic sclerosis, where wound healing is impaired, Daoussis et al. noted that CO_2_ laser is safer on small lesions than traditional excision, providing symptom control and functional improvement with fewer complications [54]. Compared with surgery, CO_2_ laser is less invasive, quicker, best for superficial symptomatic lesions, while excision is reserved for larger or deeper deposits requiring reconstruction.
4. Discussion
Most available evidence addressing the management of calcinosis cutis is derived from studies on calcinosis cutis in general, while data specifically focusing on calcinosis cutis universalis remain extremely limited. As a result, therapeutic strategies discussed in this review are largely extrapolated from broader calcinosis cutis populations and should be interpreted with caution when applied to the universalis subtype.
The therapeutic approach to calcinosis cutis relies primarily on stabilizing the underlying connective tissue disease, as persistent inflammation is a major driver of progression. Systemic therapies—including bisphosphonates, calcium-channel blockers, tetracyclines, phosphate binders, probenecid, IVIG, colchicine, and sodium thiosulfate—show heterogeneous and often partial efficacy, with responses influenced by lesion size, disease chronicity, and patient-specific factors. Biologic agents such as rituximab and infliximab have demonstrated encouraging results in selected refractory cases, particularly in autoimmune-associated calcinosis, but their use remains limited by cost, potential adverse effects, and low-quality evidence. Overall, medical therapy aims mainly at symptom control and slowing disease progression rather than achieving cure.
When conservative management fails or lesions cause pain, ulceration, infection, or functional impairment, surgical intervention becomes an important therapeutic option. Excision, curettage, CO_2_ laser ablation, and minimally invasive debridement can provide rapid symptomatic relief, although recurrence is common. Surgical risks—including delayed wound healing, neurovascular injury, and functional compromise—are particularly relevant in patients with connective tissue diseases or deep lesions. Surgery should therefore be reserved for carefully selected, symptomatic patients and ideally combined with optimized medical disease control.
4.1. Clinical Decision-Making and Therapeutic Sequencing
In the absence of validated guidelines, management of calcinosis cutis universalis must be pragmatic and individualized. Treatment selection should consider underlying disease activity, lesion size and depth, anatomical location, symptom burden, functional impact, and risk of complications. Early or inflammatory lesions may benefit modestly from medical or localized therapies, whereas long-standing, bulky, or mechanically limiting deposits often require procedural or surgical intervention.
To improve clinical applicability, we propose an expert-opinion–based therapeutic decision-making algorithm (Figure 3) that integrates medical optimization, minimally invasive techniques, and surgery in a stepwise manner. Although based on low-level evidence, this framework reflects current practice and provides practical guidance while acknowledging the predominantly palliative nature of available treatments.
4.2. Limitations of the Existing Evidence
The interpretation of therapeutic outcomes in calcinosis cutis universalis is substantially constrained by the quality of the available evidence. Most published data consist of single case reports or small, uncontrolled case series, frequently involving heterogeneous connective tissue diseases, variable disease durations, and mixed calcinosis subtypes. Outcome measures are inconsistently reported and often rely on subjective clinical improvement rather than standardized radiologic or functional endpoints.
Another important limitation is publication bias, as positive outcomes are more likely to be reported than treatment failures. Comparative studies between different medical or surgical strategies are lacking, and long-term follow-up data addressing recurrence, durability of response, and quality-of-life outcomes remain scarce. As a result, current therapeutic recommendations are largely based on expert opinion rather than high-level evidence, underscoring the urgent need for prospective registries and collaborative multicenter studies. Furthermore, most of the available data concern other subtypes of calcinosis cutis; therefore, the recommendations for calcinosis cutis universalis are largely extrapolated from treatments used for these other subtypes.
5. Conclusions
Calcinosis cutis remains challenging to manage, with treatment decisions largely individualized due to the absence of standardized guidelines. Conventional medical therapies may help stabilize the disease or reduce symptoms, but their benefits are often limited. Biologic agents show promising results but at the cost of potentially severe adverse effects. Surgery remains a valuable option for symptomatic, complicated or localized lesions. Further research is required to define clearer treatment algorithms and achieve more durable disease control.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Suleman F.E. Ally M.M.T.M. Calcinosis Cutis Universalis—A Rare Manifestation of Systemic Lupus Erthymatosus S. Afr. J. Radiol.201216222310.4102/sajr.v 16i 1.228 · doi ↗
- 2Stewart V.L. Herling P. Dalinka K. Calcification in Soft Tissues JAMA 1983250788110.1001/jama.1983.033400100600326854888 · doi ↗ · pubmed ↗
- 3Zanatta E. Desportes M. Do H.H. Avouac J. Doria A. Feydy A. Allanore Y. Pseudotumoral Calcinosis in Systemic Sclerosis: Data from Systematic Literature Review and Case Series from Two Referral Centres Semin. Arthritis Rheum.2020501339134710.1016/j.semarthrit.2020.03.00932336495 · doi ↗ · pubmed ↗
- 4Le C. Bedocs P.M. Calcinosis Cutis Stat Pearls Stat Pearls Publishing Treasure Island, FL, USA 202528846311 · pubmed ↗
- 5Lobo I.M.M. Machado S. Teixeira M. Selores M. Calcinosis Cutis: A Rare Feature of Adult Dermatomyositis Dermatol. Online J.2008141010.5070/D 387C 2F 37M 18319027 · doi ↗ · pubmed ↗
- 6Wilmer W.A. Magro C.M. Calciphylaxis: Emerging Concepts in Prevention, Diagnosis, and Treatment Semin. Dial.20021517218610.1046/j.1525-139X.2002.00052.x 12100455 · doi ↗ · pubmed ↗
- 7Jiménez-Gallo D. Ossorio-García L. Linares-Barrios M. Calcinosis cutis y calcifilaxis Actas Dermosifiliogr.201510678579410.1016/j.ad.2015.09.00126394755 · doi ↗ · pubmed ↗
- 8Bienvenu B. Traitement des calcinoses sous-cutanées des connectivites Rev. Med. Interne 20143544445210.1016/j.revmed.2014.04.01824880741 · doi ↗ · pubmed ↗