Hip Joint Synovial Cavity Thickness in Early Juvenile Idiopathic Arthritis Without Effusion: A Cross-Sectional Ultrasound Study
Zbigniew Żuber, Wojciech Kmiecik, Krzysztof Batko, Elżbieta Mężyk, Joanna Ożga, Magdalena Krajewska-Włodarczyk, Tomasz Madej, Bogdan Batko

TL;DR
This study finds that hip joint synovial cavity thickness in children without fluid buildup is similar in those with early juvenile arthritis and healthy controls, suggesting it's not a reliable disease marker.
Contribution
The study provides new evidence that synovial cavity thickness is not a distinct marker for early juvenile idiopathic arthritis when no effusion is present.
Findings
HJSCT showed high left-right agreement and was strongly associated with age but not with JIA status.
Predicted HJSCT increases rapidly in childhood and stabilizes in adolescence, indicating a physiological pattern.
HJSCT did not significantly differ between JIA patients and healthy controls in adjusted models.
Abstract
Background: The clinical meaning of hip joint synovial cavity thickness (HJSCT) on ultrasound (US) in juvenile idiopathic arthritis (JIA) without effusion is uncertain. Methods: In this cross-sectional study, we analyzed 369 children (187 JIA; 182 controls) undergoing hip US at a referral center in Kraków, Poland. JIA examinations were performed upon initial referral, early in the care pathway. We excluded patients with hip effusion and pre-existing inflammatory, traumatic or degenerative hip pathology. HJSCT was defined as the distance from the outer capsule margin to the femoral neck cortex. We used a Toshiba Aplio 400 system with a 12 MHz probe to measure and derive mean bilateral HJSCT. Bilateral concordance was assessed. Iterative multivariable linear regression modeling was used to compare groups, adjusting for non-linear age effects (natural splines) and WHO height-for-age…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
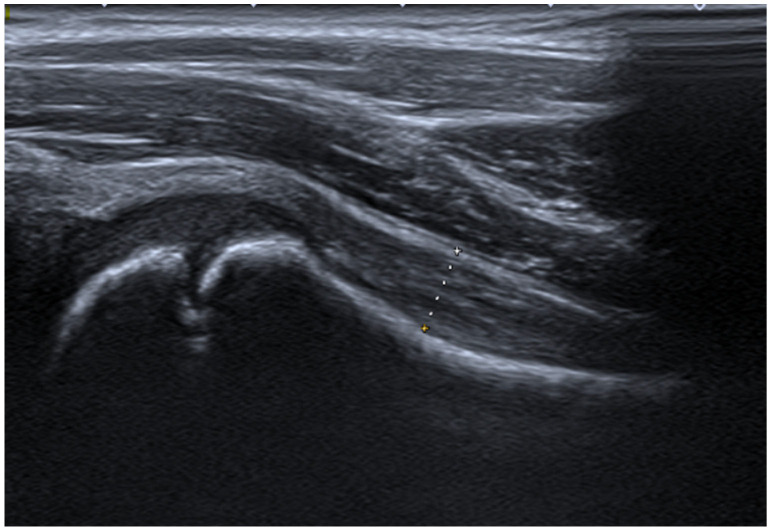 Figure 1
Figure 1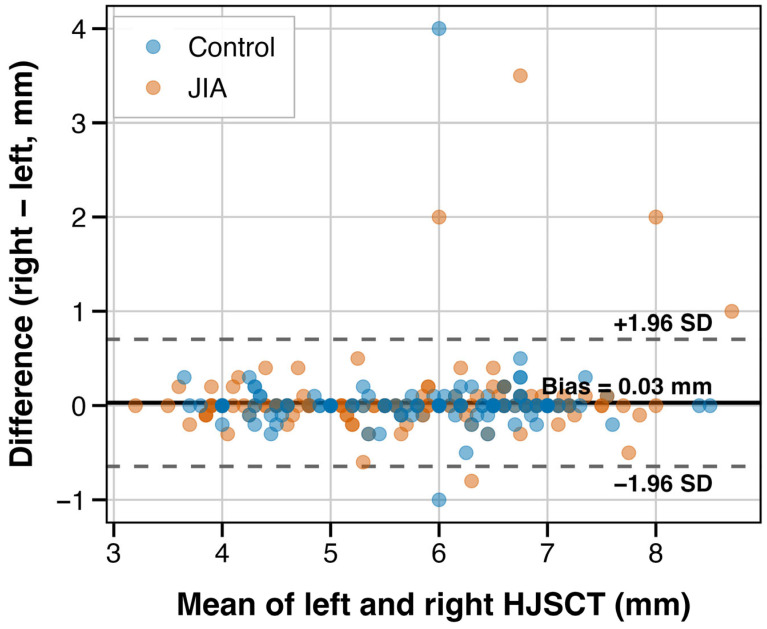 Figure 2
Figure 2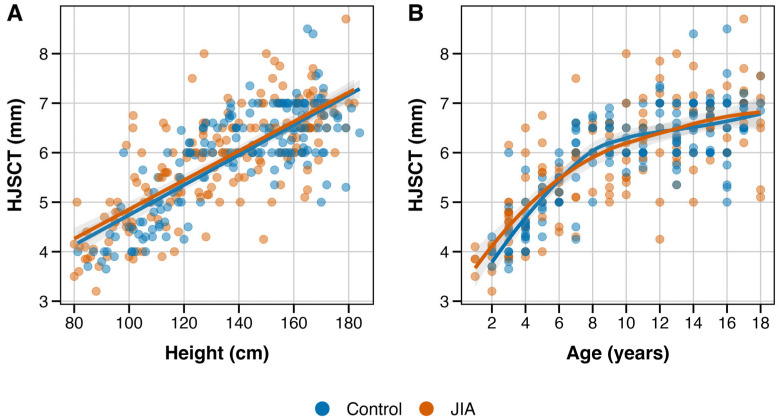 Figure 3
Figure 3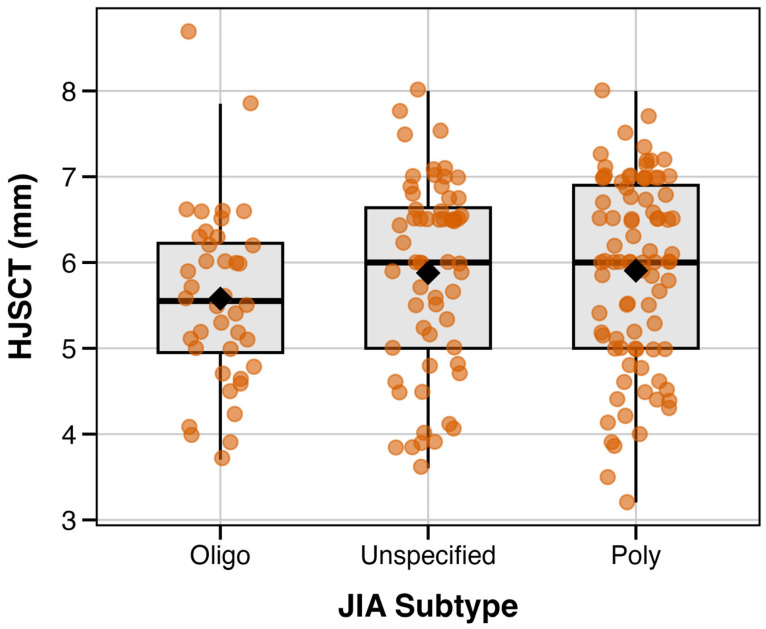 Figure 4
Figure 4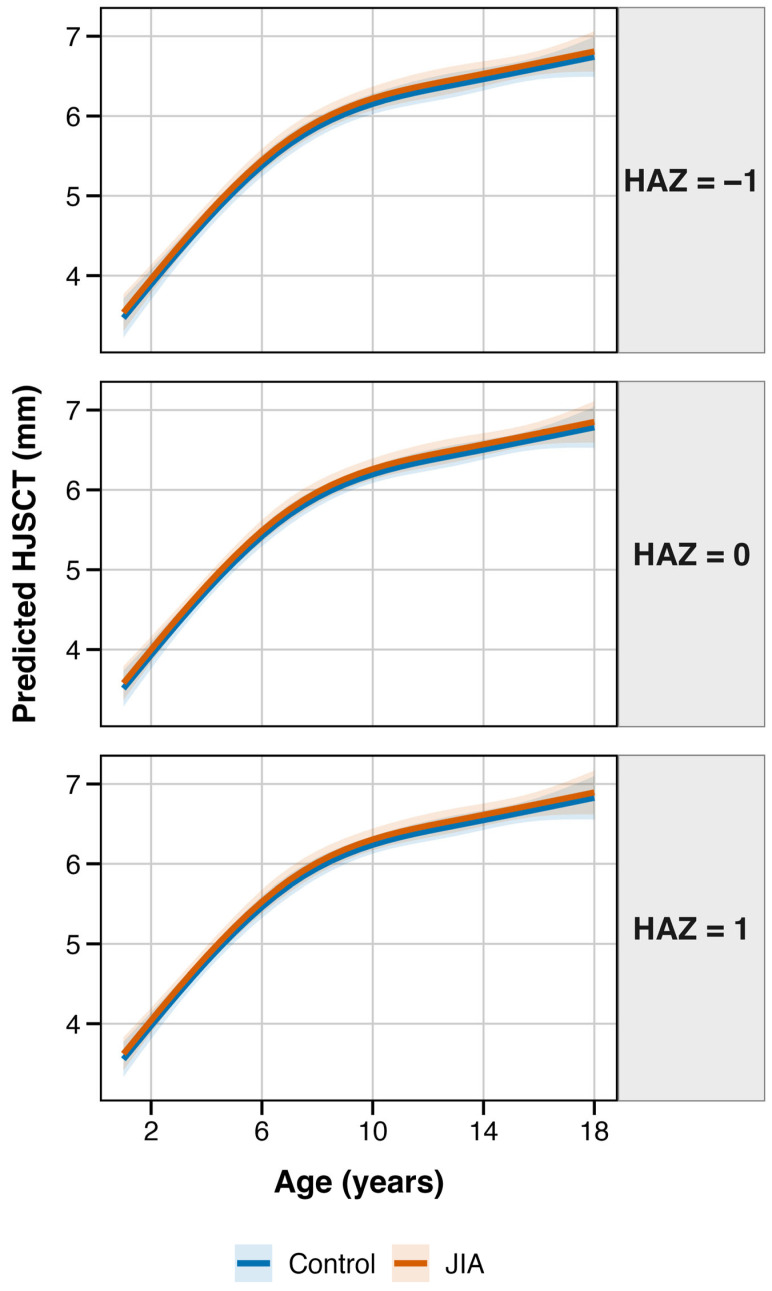 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune and Inflammatory Disorders Research · Hip disorders and treatments · Orthopedic Infections and Treatments
1. Introduction
Musculoskeletal disorders carry high socioeconomic and healthcare burden, with a range of geographic disparities [1]. Juvenile idiopathic arthritis (JIA) is a chronic immune-mediated disease that begins at an early age and impairs physical function [2,3]. It is also one of the most common rheumatic diseases in childhood, with pooled prevalence estimated at 70 cases per 100,000 persons in Europe [4]. Hip joint involvement is relatively common and estimated to occur in about 30–50% of JIA cases [5,6]. Even when the hip is uninvolved at diagnosis, it can often be affected later on during the course of JIA. Moreover, this may occur despite appropriate treatment [7]. In a cohort of newly diagnosed JIA patients, hip joint involvement changed from 6% to 19% within 5 years [7]. Recently, the ILAR [8] subtype classification was reappraised in a data-driven, pattern recognition approach that highlighted the importance of hip involvement as a poor prognostic factor [5]. Polyarticular and enthesitis-related subtypes are also more frequently tied to hip manifestations and have been associated with the general severity of joint arthritis [9]. While the knee, ankle, elbow and wrist are the most common joints affected upon first manifestation of JIA [7], all of these locations are easily accessible in physical examination. Meanwhile, reliable assessment of hip involvement is only possible through various imaging modalities. Early identification of transient or structural hip abnormalities remains of high clinical importance. It has been shown that hip involvement severity is tied to the burden of physical disability and is associated with arthritis duration [9]. The weight-bearing function of the hip joint is also critical in the adequate development of adult stature and physical fitness.
Despite years of research and emerging machine learning tools, there is no single biomarker or model that can predict JIA incidence or rate of progression [5,10]. JIA category alone is a poor predictor of short-term outcomes [11]. Prior studies have shown that age, gender, serostatus, microbiome, symmetry and extent of joint involvement, age at onset and disease duration affect prognosis in JIA, though these relationships are variable across studies [2,12,13,14]. Comprehensive analyses have shown that although numerous soluble molecules were investigated as prognostic/diagnostic aids, very few validation studies were conducted [15]. From a clinical standpoint, the current therapeutic approach remains focused on timely diagnosis and control of JIA activity using disease-modifying antirheumatic drugs. Other supportive treatment options are also emerging [16].
The optimal diagnostic approach for JIA is still not established, though recommendations are emerging [17,18,19]. Conventional radiography remains in use as a reference measure for peripheral joint destruction, with several validated scoring methods available [20]. Expert guidelines have also been published [21]. While US examination offers the promise of fast, noninvasive and low-cost imaging, no standardized approach has been agreed upon [22,23]. In part, this relates to operator dependency and limited validation of imaging findings that constrain widespread use and agreement. While US is increasingly used for peripheral joint evaluation in JIA, its application in hip imaging has largely focused on screening for joint effusion, synovitis or structural abnormalities often associated with established or later-stage disease [19,24]. In contrast, quantitative assessment of hip joint capsule measures in the absence of effusion (particularly in early-stage JIA) remains poorly described. The clinical significance of abnormalities in these measurements in early JIA has yet to be elucidated.
The frequent involvement of the hip in inflammatory conditions, coupled with the limited utility of physical examination and nonspecific nature of symptoms, makes this a location of high clinical importance (for an overview see Table 1). A retrospective study of 86 cases of pediatric post-infectious arthritis reported hip involvement in close to 50% of cases [25]. For JIA, hip abnormalities have been reported to affect between 30 and 50% of children [26]. US is viewed as a tool that should ideally exclude the presence of effusion [27]. Although the sensitivity for detecting effusion is reported to be over 90% in some studies [28], the type of fluid and temporal character (i.e., dynamics of the acute setting; sufficient time needs to pass for fluid to accumulate and become detectable) need to be considered [29]. However, aside from screening for effusion, US is also utilized to track physiological structural changes. Abnormalities in the rate or degree of growth may be relevant for differential of pathology.
Taken together, the aim of the present study was to describe hip joint synovial cavity thickness (HJSCT) in early JIA patients and healthy controls, and to evaluate its relationship with age, height, sex and disease status. By focusing on a population of patients without joint effusion in early JIA, the goal of this report is to characterize the inter-relationships between arthritis and anthropometric factors, which will extend the current evidence supporting application of reference charts for healthy children within the JIA population.
2. Materials and Methods
2.1. Study Overview
This observational cross-sectional study is based on US records of the pediatric hip joint among 369 children and adolescents. We extracted data on hip joint synovial cavity thickness (HJSCT) based on patient assessments at St. Ludwig’s Hospital, which is a reference pediatric rheumatology center in Kraków, Poland. We excluded patients with any of the following: (i) detectable joint effusion or (ii) history of pre-existing inflammatory, traumatic or degenerative hip pathology.
US examinations in the JIA patients were performed after referral to our center, early in the care pathway. However, due to inconsistent documentation, we were unable to reliably determine treatment naïvety or symptom duration prior to diagnosis; this limitation should be considered when interpreting the results.
Control participants were recruited from consecutive outpatients presenting for hip US imaging, without a final diagnosis of a specific disorder (the most frequent indication was exclusion of rheumatic disease, as per center specifics). Exclusion criteria in the control group were analogous, with the additional exclusion of growth abnormalities or relevant genetic conditions. Prior to study enrollment, we obtained written informed consent from parents or legal guardians. The study was granted approval by the local Bioethics Committee (Decision No. 99/KBL/OIL/2010).
2.2. Examination Protocol
Hip joint US was performed in all patients according to an internal protocol developed at our center (for a detailed description of our model approach, please see Appendix A.1). To reduce probe placement error, measurements of HJSCT were performed three times, bilaterally, with the recording of mean values as the final measure. The bilateral mean HJSCT was selected as the primary outcome to minimize random measurement variability and to provide a stable, bilaterally sensitive quantitative metric.
All examinations were conducted with a TOSHIBA Aplio 400 system with a 12 MHz linear transducer. There were three unblinded physicians who performed US assessments. Reproducibility of the adopted US approach to hip joint assessment was determined in a prior study; the intra- and inter-rater coefficients of variation were 0.5% and 12.4%, respectively [38].
US examination was performed in supine position, with the hip extended, in mild external rotation. First, the probe was placed in the sagittal position, parallel to the anatomical location of the femoral neck, at an angle of ~20° (see Figure 1). Assessments were performed following the anterior longitudinal approach, in which the HJSCT distance is measured as maximum of external joint capsule margin to the cortical edge of the femoral neck surface. Age-related reference values have been published previously by our team [38] and other groups [39].
2.3. Statistical Analysis
Analysis was performed in R version 4.5.2 (R Core Team, 2025; R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were summarized using mean (standard deviation; SD) or median (interquartile range; IQR), as deemed appropriate. Categorical variables were reported as counts and percentages. Cross-group comparisons were reported using the Wilcoxon rank-sum test for continuous and chi-square test for categorical variables.
This exploratory study relied on a convenience sample of consecutive, eligible patients, with no a priori sample size calculation performed. Our findings should be interpreted cautiously, as this report may be underpowered to detect small-to-moderate interaction effects.
Bilateral concordance of left and right HJSCT measurements was quantified using intraclass correlation coefficient (ICC) and assessed using Bland–Altman analysis.
For iterative regression modeling, bilateral mean HJSCT was the primary outcome. We aimed to evaluate whether JIA status was associated with HJSCT measurements after accounting for growth describing factors. Different multivariable linear regression models were fitted with the aim of adjusting for (i) potential non-linearity using different transformation and (ii) relative height, as quantified using a height-for-age z-score (HAZ). Model comparison was based on changes in Akaike Information Criterion (AIC) and likelihood ratio tests for nested models.
Due to the exploratory nature of this study, we also examined interaction effects between JIA status and growth-related factors. To account for heteroscedasticity, models were fitted with robust HC3 standard errors. We calculated 95% confidence intervals (CIs) based on 1000 bootstrap replicates. The effect of JIA subtype was another supplemental analysis.
All tests were two-tailed and p value < 0.05 was statistically significant.
3. Results
3.1. Description of the Study Cohort
We examined measurements of HJSCT using data for 369 pediatric patients, including 187 children with early JIA and 182 controls. Both groups were comparable in age, with medians (IQR) of 9 (5–14) vs. 11 (6–14) years (p = 0.079). Sex distribution was also similar (male gender; 36.4% vs. 39.6%, p = 0.59). Patients with JIA were characterized by a lower absolute height (mean (SD); 132.9 (28.2) vs. 140.0 (25.5) cm, p = 0.013), which is consistent with their younger age distribution. Given the above, and due to strong collinearity between age and height (r = 0.95, VIF > 9), we calculated height-for-age z-scores (thereafter referred to as HAZ) using the WHO Chart Reference (WHO 2006–7 [40,41,42]). Additionally, supplemental analyses with internal sex-specific spline models based on control group data were performed but showed greater instability. Our approach suggests reduced collinearity with VIF below 2.5, with mild age–HAZ correlation (r = −0.13). Importantly, we did not observe significant differences in HAZ scores across the JIA and control groups (mean (SD); 0.07 (1.38) vs. 0.28 (1.09), p = 0.11).
3.2. Characteristics of Sonographic Measurements
Left and right HJSCT measurements showed very high bilateral agreement (ICC(2,1) 0.947, 95% CI 0.935–0.956). In Bland–Altman analysis, we also did not observe evidence of systematic bias, with a mean difference of 0.03 mm (95% limits of agreement [LoA] −0.64–0.70 mm; see Figure 2).
3.3. Hip Joint Synovial Cavity Thickness in JIA and Controls
We examined the relationships between anthropometric variables and HJSCT assessments (see Figure 3). HJSCT increased with age in a non-linear pattern, with larger increments during early childhood. HJSCT was also linearly (positively) associated with height. In unadjusted comparison, mean HJSCT was highly comparable between groups (JIA 5.83 (1.09) vs. controls: 5.95 (0.99) mm; difference −0.12 mm, p = 0.25). This minimal crude difference (i.e., equivalent to 0.11 SD) illustrates the importance of adjusted analyses to account for the influence of growth-related factors.
Thereafter, we compared several multivariable models with varying functional forms for age and different covariate terms (see Table 2). Based on AIC comparison, we identified Model 7 (natural splines for age with df = 3, with adjustment for HAZ and JIA status; adj. R^2^ = 0.656) as the best. We also tested whether the JIA effect varied with age based on nested model comparison. We did not observe a significant interaction (F(3, 360) 1.01, p = 0.39), which suggests that the JIA effect (or lack thereof) may be interpreted as consistent across age groups.
Final model coefficients with HC3 robust standard errors are presented in Table 3. HJSCT showed a non-linear, positive association with age (all spline terms p < 0.001). HAZ was recorded with a numerical trend (beta 0.04, 95% CI −0.01–0.09, p = 0.11). JIA status was not a significant predictor after covariate adjustment (beta 0.07, 95% CI −0.06–0.19, p = 0.30).
Our findings suggest that after accounting for the growth-related factors, HJSCT does not differ significantly between children/adolescents with JIA and the control group. We estimated the JIA effect as 0.07 mm (i.e., equivalent to 0.06 SD), which is clinically negligible.
In supplemental analysis with model bootstrap, we identified Model 7 as the consistently best performer (~80% of 1000 resamples). Of note, patients’ sex was not a significant predictor with addition to the spline model (F(1, 362) 0.00, p = 0.99).
3.4. Relationship Between JIA Subtype and Hip Joint Synovial Cavity Thickness
In additional exploratory analysis, we examined whether HJSCT differed by JIA subtype. Oligoarticular JIA showed numerically lower mean HJSCT, as compared with the polyarticular and undifferentiated subtypes (see Figure 4; Table 4). However, after adjustment for height, JIA subtype was not an independent predictor of HJSCT (p = 0.86). Therefore, crude differences are likely to reflect confounding by age (median 7.5 vs. 10 years in oligoarticular vs. other subtypes) rather than actual subtype-specific effects. With the observed sample size and variability, this analysis is likely underpowered due to observed differences of about ~0.3 mm.
3.5. Predicting Hip Joint Synovial Cavity Thickness
Lastly, we used the final model to derive estimates of age-dependent HJSCT, stratified by HAZ scores (see Figure 5). We observed that HJSCT sharply increases in early childhood (~1.2 mm for 2–5 age group; ~1.1 mm for ages 5–10). As expected, growth rate slowed during adolescence (0.4 mm for ages 10–15; 0.2 mm for ages 15–18). The effects of relative height were additive within the examined age range. Of note, children who were taller-for-age were characterized with ~0.09 mm higher HJSCT assessments than shorter-for-age children (HAZ +1 vs. −1). However, this difference was not statistically significant (p = 0.11). We did not observe major differences in the trajectories for JIA and control groups.
4. Discussion
This pilot, cross-sectional study evaluated HJSCT in children and adolescents with early JIA, as compared with controls presenting for hip US, but without a relevant, formal diagnosis. The salient finding of this report is that growth-related anthropometric factors are major determinants of HJSCT, accounting for about 65% of the variance in our final model. HJSCT is characterized by a strong, non-linear increase with age. Importantly, in this population without detectable joint effusion, we observed no significant difference in mean bilateral HJSCT between both groups. In exploratory analyses, crude differences across JIA subtypes (i.e., lower HJSCT values in oligoarticular JIA) were attenuated after accounting for growth-related factors. Our findings suggest that potential presence of “subclinical” synovial thickening is not a manifestation of early JIA patients, given the absence of effusion.
Although consensus definitions and protocols are emerging (for example, PIUS-Hip), practice remains heterogeneous and widespread adoption of a single pediatric hip US protocol is still evolving [18,19]. One of the earliest descriptions of painful hip US was first reported by Seltzer in 1980 [43]. While the distance between the femoral surface and the anterior capsule is commonly utilized (on average 4.7 mm) [44,45,46], standardization and subsequent comparison across studies remains difficult. Early protocols measured the posterior capsule margin, but differentiation between capsule layers in patients without effusion is often dependent on echogenicity, presence of fluid and technical factors. To reduce associated bias and maximize practicality, we favored measurement of mean bilateral total thickness (i.e., femur to external capsule margin), which was characterized high concordance and narrow limits of agreement. In the literature, modest variability is observed across different positions/techniques of measurement (common positioning differences are ~1 mm) [39,46].
Our multivariable analysis suggests that HJSCT is a physiological metric tied closely to skeletal maturity. Bone growth is stimulated by a complex interface of genetic, metabolic, and mechanical factors [47,48,49]. Due to strong collinearity between age and raw height (r ~0.95), we used height-for-age z-scores to account for growth status independent of a child’s chronological age. The modest improvement in model fit when including HAZ suggests that sonographic interpretation based solely on “calendar age” may be suboptimal, though this association did not reach statistical significance. Sex differences are less pronounced in childhood, potentially reflecting age-dependent hormonal influences, which may explain the lack of association observed with HJSCT at present [50].
The lack of HJSCT enlargement in the early JIA cohort is important when considering hypotheses of a pre-clinical JIA stage. In rheumatic disorders, systemic inflammation is purported to exert deleterious multiorgan effects due to cytokine spillover from inflamed joints [51]. Elevated acute phase reactants are predictors of unfavorable outcomes in JIA patients [2], including requirement for total hip arthroplasty [6]. While aberrant states of immune activation (e.g., cytokine storm, macrophage activation syndrome) are well studied, the cumulative effects of low-grade inflammation have received less attention. We recruited JIA patients at an early stage of the care pathway, in whom potential overgrowth of synovium could represent an early indicator of disease. We did not detect a difference in HJSCT in early, non-effusive JIA. Therefore, if low-grade inflammation affects capsular thickness, we hypothesize the effect is likely to be small, delayed, or not captured by the HJSCT measurement approach.
In the current study, our exploratory interaction models suggested that associations between HJSCT and growth-related factors do not differ by JIA status. However, given the cross-sectional design and limited clinical characterization, these findings require dedicated study. While US is sensitive for the detection of erosions and effusion [52,53,54], HJSCT is not a standalone marker for subclinical synovitis in early JIA.
Despite the high sensitivity of MRI for detecting early inflammatory changes [55], its cost, sedation requirement and limited accessibility restrict its utility for routine surveillance [56,57]. US is the modality of choice for longitudinal patient evaluation due to practicality. Its use for detection of subclinical synovitis has largely entered into daily practice [53,58] and it is increasingly apparent that a proportion of asymptomatic patients can have imaging abnormalities, which has implications for classification, treatment and outcomes in JIA [58,59]. However, for US to be a reliable screening tool, validation of reference values in different clinical subgroups is important. Our results tentatively support the use of HJSCT reference values for early JIA patients in the absence of effusion.
Importantly, the absence of disease activity indices, inflammatory markers or adjunct MRI data precludes inferential conclusions regarding the potential of inflammation-derived HJSCT variations. It remains to be elucidated whether synovial capsule changes below our assessment threshold can reflect low-grade synovial inflammation.
Bony tissue is difficult to evaluate reliably, which makes US a modality for assessment of soft tissue, fluid presence or localization (e.g., aid in injection or aspiration). Interpretation of musculoskeletal US findings is, however, still evolving. For pediatric patients, there is an unmet need for geographically validated reference values. Defining borderline thresholds for growth and development abnormalities is also of interest but requires in-depth characterization of physiological patterns. For example, cartilage vascularization can appear similar to synovitis on US, while it is a finding that is highly prevalent in healthy subjects [23,60]. Hip joint US enables examination of the femur head surface, which may explain contralateral differences in absolute extremity length (e.g., identifying degenerative changes due to pathological conditions such as slipped capital femoral epiphysis, Perthes disease or septic arthritis). In contrast to effusion, it remains unelucidated whether the thickness of a specific capsular layer could reflect a subclinical state of inflammation.
There are several limitations of this pilot study that need to be acknowledged. The heterogeneity of JIA manifestations is well established, which may obscure arthritis-subtype-specific US characteristics. Our methodology of US assessment with averaging of HJSCT values was undertaken to minimize random error, but it may lead to reduced sensitivity regarding unilateral pathology. While this was a relatively large clinical sample, it is likely underpowered for subgroup analyses, unless the expected effect for JIA subtype is large. Furthermore, the enrollment of early JIA patients with an unspecified symptom-to-diagnosis timeframe carries a high degree of potential bias. The extrapolation of findings is likely relevant only to early JIA patients, in whom synovial tissue exposure to a proinflammatory milieu is brief. The cross-sectional design and lack of detailed clinical and biochemical assessments warrant cautious interpretation and preclude inferential conclusions; accordingly, these observations should inform hypothesis generation rather than immediate clinical decision-making. As a single-center report with an internal protocol, operator- and protocol-specific practices are other sources of bias that could limit generalizability. Prospective longitudinal cohorts tracking HJSCT trajectories alongside validated disease activity measures (e.g., JADAS [61]), treatment response and structural outcomes would be necessary to establish whether serial HJSCT measurements carry prognostic value. Specifically, studies examining whether HJSCT changes precede clinical flares or correlate with inflammatory biomarker trajectories could clarify the predictive utility of capsular assessment beyond effusion detection. The consideration of DMARD and non-steroidal anti-inflammatory treatment effects on sequential HJSCT assessments is also of high value.
5. Conclusions
Hip involvement in JIA is a risk factor for poor prognosis, including permanent physical disability. Due to latent and non-specific symptoms, associated risk prediction tools for hip joint involvement remain of high interest. We examined US assessments of hip joint using a cross-sectional sample of 187 early JIA cases and 182 control referrals with negative rheumatic diagnosis. In early JIA patients presenting without effusion, we observed that HJSCT was comparable. Given further validation, our findings support the use of pediatric US for hip assessment based on healthy children reference charts. However, prospective longitudinal studies accounting for disease activity, duration and treatment are highly warranted.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1GBD 2019 MSK in Adolescents Collaborators Global Pattern, Trend, and Cross-Country Inequality of Early Musculoskeletal Disorders from 1990 to 2019, with Projection from 2020 to 2050 Med 20245943962.e 610.1016/j.medj.2024.04.00938834074 PMC 11321819 · doi ↗ · pubmed ↗
- 2FlatøB. Lien G. Smerdel A. Vinje O. Dale K. Johnston V. Sørskaar D. Moum T. Ploski R. FørreØ. Prognostic Factors in Juvenile Rheumatoid Arthritis: A Case-Control Study Revealing Early Predictors and Outcome after 14.9 Years J. Rheumatol.20033038639312563700 · pubmed ↗
- 3Romano F. Di Scipio F. Baima G. Franco F. Aimetti M. Berta G.N. Health-Related Quality of Life in Juvenile Idiopathic Arthritis: A Systematic Review of Phase III Clinical Trials J. Clin. Med.20251425410.3390/jcm 1401025439797336 PMC 11721659 · doi ↗ · pubmed ↗
- 4Thierry S. Fautrel B. Lemelle I. Guillemin F. Prevalence and Incidence of Juvenile Idiopathic Arthritis: A Systematic Review Jt. Bone Spine 20148111211710.1016/j.jbspin.2013.09.00324210707 · doi ↗ · pubmed ↗
- 5Eng S.W.M. Aeschlimann F.A. van Veenendaal M. Berard R.A. Rosenberg A.M. Morris Q. Yeung R.S.M. Patterns of Joint Involvement in Juvenile Idiopathic Arthritis and Prediction of Disease Course: A Prospective Study with Multilayer Non-Negative Matrix Factorization P Lo S Med.201916 e 100275010.1371/journal.pmed.100275030807586 PMC 6390994 · doi ↗ · pubmed ↗
- 6Sorokina L.S. Avrusin I.S. Raupov R.K. Lubimova N.A. Khrypov S.V. Kostik M.M. Hip Involvement in Juvenile Idiopathic Arthritis: A Roadmap from Arthritis to Total Hip Arthroplasty or How Can We Prevent Hip Damage?Front. Pediatr.2021974777910.3389/fped.2021.74777934805045 PMC 8604160 · doi ↗ · pubmed ↗
- 7Hemke R. Nusman C.M. van der Heijde D.M.F.M. Doria A.S. Kuijpers T.W. Maas M. van Rossum M.A.J. Frequency of Joint Involvement in Juvenile Idiopathic Arthritis during a 5-Year Follow-up of Newly Diagnosed Patients: Implications for MR Imaging as Outcome Measure Rheumatol. Int.20153535135710.1007/s 00296-014-3108-x 25119829 · doi ↗ · pubmed ↗
- 8Petty R.E. Southwood T.R. Manners P. Baum J. Glass D.N. Goldenberg J. He X. Maldonado-Cocco J. Orozco-Alcala J. Prieur A.-M. International League of Associations for Rheumatology Classification of Juvenile Idiopathic Arthritis: Second Revision, Edmonton, 2001 J. Rheumatol.20043139039214760812 · pubmed ↗