Likelihood of Blood Culture Positivity Using SeptiCyte RAPID
Krupa A. Navalkar, Alyse Wheelock, Melissa Gregory, Danielle V. Clark, Hannah Kibuuka, Stephen Okello, Sharon Atukunda, Abdullah Wailagala, Peter Waitt, Francis Kakooza, George Oduro, Nehkonti Adams, Maximilian Dietrich, Maik von der Forst, Marcus J. Schultz, Neil R. Aggarwal

TL;DR
A new test called SeptiCyte RAPID can predict blood culture positivity in sepsis patients, potentially improving diagnostic efficiency in resource-limited settings.
Contribution
The study demonstrates that SeptiScores can predict blood culture positivity before results are available, offering a novel diagnostic aid.
Findings
SeptiScores show a strong correlation with blood culture positivity (ROC AUC of 0.91 for BC+ cases).
A SeptiScore above 10 increases the likelihood of a positive blood culture result.
The test may improve blood culture efficiency in low-resource and emergency settings.
Abstract
Background: Early diagnosis and identification of causative pathogens using blood culture in patients suspected of blood stream infection (BSI) and sepsis are critical for improving patient outcomes through earlier and more targeted treatment. There is a need for tools that can guide the use of microbiologic diagnostics, especially where resources are limited, such as in lower- and middle-income countries (LMICs), pandemic and mass-casualty scenarios, and prolonged field care settings during military operations. Methods: Post hoc retrospective analysis of individual patient data from three prospective clinical studies, conducted in North America, Europe and Africa, to investigate the association between SeptiCyte RAPID test results (SeptiScores) and blood culture (BC) results. Hypothesis: that a significant correlation exists between elevated SeptiScores and positive blood culture…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
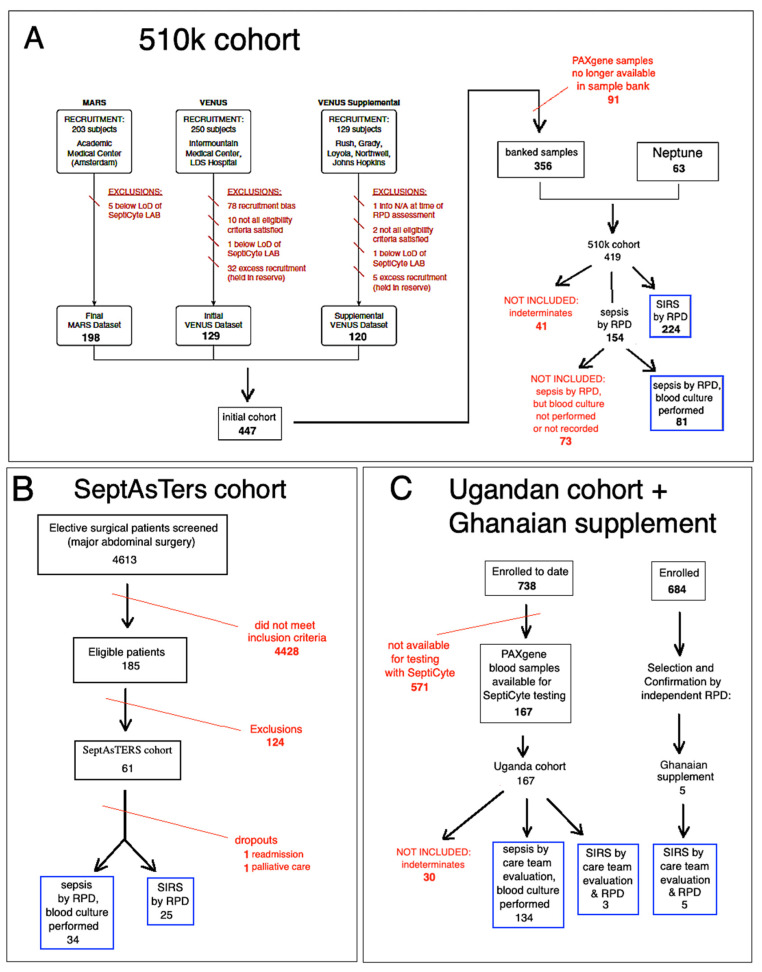 Figure 1
Figure 1 Figure 2
Figure 2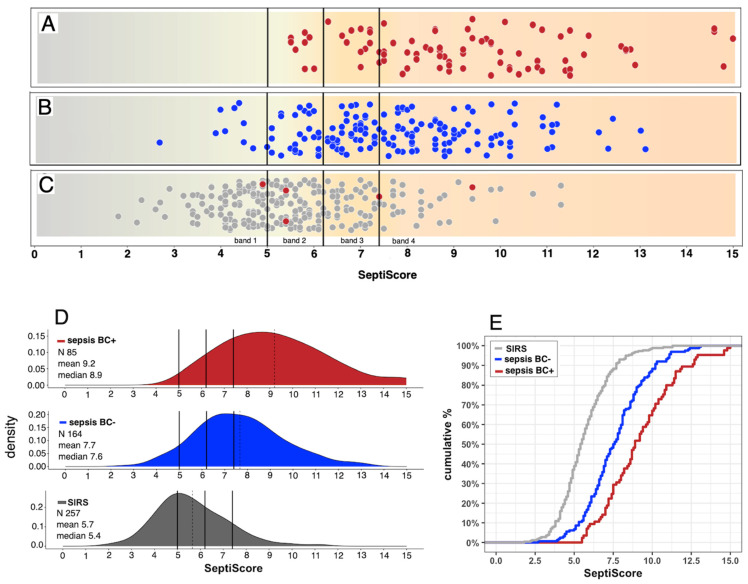 Figure 3
Figure 3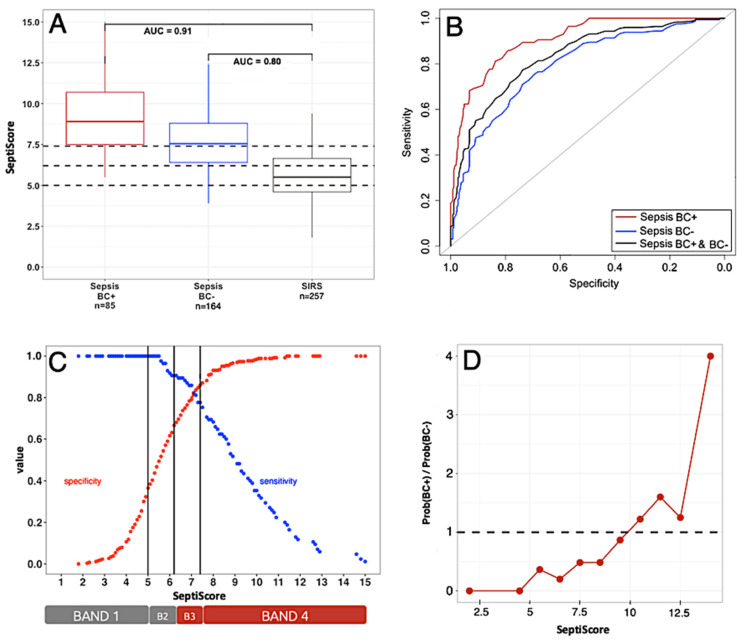 Figure 4
Figure 4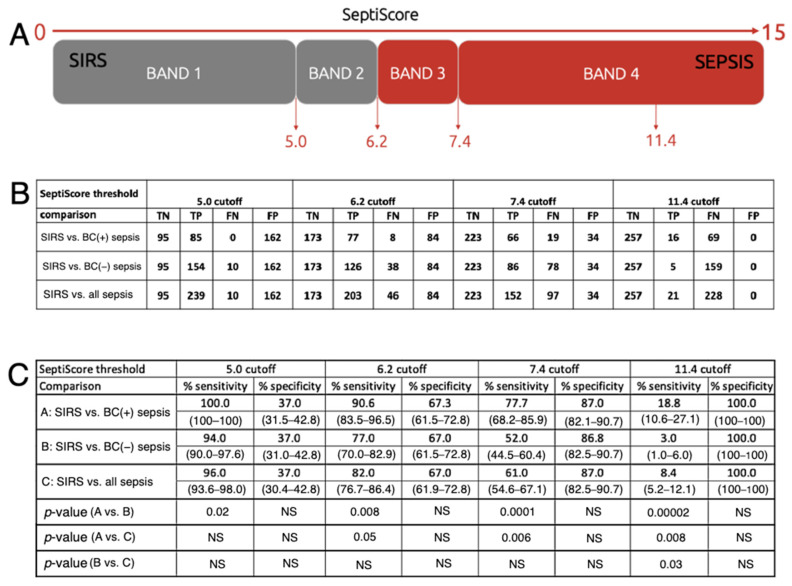 Figure 5
Figure 5- —Immunexpress, Inc.
- —the DRIVe Solving Sepsis program of the Biomedical Advanced Research and Development Authority (BARDA), a branch of the US HHS Office of the Assistant Secretary for Preparedness and Response
- —the Joint Program Executive Office for Chemical, Biological, Radiological and Nuclear Defense’s (JPEO-CBRND) Joint Project Lead for CBRND Enabling Biotechnologies (JPEO CBRND JPL EB) on behalf of the
- —the Defense Health Agency (DHA) COVID funding initiative for The Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc.
- —the Defense Health Agency’s Joint Program Committee-2/Military Infectious Diseases Research Program
- —the HJF- (DoD-Navy) Cooperative Agreement
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Identification and Susceptibility Testing · Sepsis Diagnosis and Treatment · Neonatal and Maternal Infections
1. Introduction
Bloodstream infections (BSI) are a major cause of morbidity and mortality in both hospital and community settings worldwide [1,2,3]. Early diagnosis and identification of causative pathogens in patients suspected of BSI and sepsis are critical for improving patient outcomes through earlier and more targeted treatment. This unmet need is most acute in poorly resourced environments, which include not just healthcare settings throughout lower- and middle-income countries (LMICs) [4,5], but also pandemic [6,7] and mass-casualty scenarios [8,9,10], and prolonged field care settings during military operations [11,12].
A lack of early BSI diagnosis has led to more patients receiving inappropriate empirical therapy and to an increase in overall mortality and antimicrobial resistance [13]. Diagnosis of BSI largely relies on culture-based methods that have evolved little in decades [14]. Some challenges associated with traditional culture-based methods for diagnosing BSI include lack of timeliness [15], reduced sensitivity associated with prior antibiotic use (false negatives), and contamination (false positives).
Empirical data indicate that >90% of all blood cultures (BC) taken are negative [16,17,18], and only ~50% of patients retrospectively diagnosed with sepsis have positive blood culture results [19]. Of those blood cultures that are positive, a contamination frequency as high as 16–23% has been reported [18]. Blood culture contamination is known to lead to increased pharmacy and laboratory costs, increased length of hospital stays, and unnecessary antibiotic use [18,20]. In addition, the interpretation of blood culture results (pathogen or contaminant) is not always straightforward and may depend on the background and experience of the clinician [21,22,23,24,25]. These clinical conundrums are often even more complex in the context of war-related polytrauma and burn injuries [10].
Thus, shortcomings in clinical practice related to testing for BSI are evident and have been noted previously [25]. Various recommendations have been proposed, aimed at decreasing the frequency of unnecessary blood cultures, for taking blood cultures of optimum volumes at optimum times, and for optimized phlebotomy techniques to decrease the frequency of contaminants [26]. The suggestion has also been made to take blood cultures only when certain leading indicators are positive (Fabre et al. 2020) [27]. On this point, temperature spikes alone appear to be insufficient as a predictor of when blood cultures should be taken (Riedel 2008 [28] and references therein).
SeptiCyte RAPID is an FDA-cleared, host-immune-response test with a one-hour turnaround time that provides a likelihood of sepsis on a scale of 0–15 (SeptiScore) (Balk et al., 2024a, 2024b) [29,30]. The test is based on quantitative analysis of the ratio of the mRNA expression levels of two single-copy genes, PLAC8 and PLA2G7. These genes were first identified as informative for sepsis diagnosis through an unbiased bioinformatic screen of microarray data that did not incorporate any assumptions about their biological function (McHugh et al., 2015) [31]. PLAC8 (also known as Onzin) is a small, highly conserved protein involved in regulating cell differentiation, innate immune responses, and autophagy. It has been linked to functions in placental development as well as roles in cancer cell proliferation and metabolic stress responses [32]. PLA2G7 encodes lipoprotein-associated phospholipase A2 (Lp-PLA2), an enzyme that hydrolyzes oxidized phospholipids in LDL particles to produce pro-inflammatory mediators. It plays key roles in vascular inflammation and has been widely studied as a biomarker and potential therapeutic target in cardiovascular disease [33]. The specific roles of these two genes in biological processes directly linked to sepsis are still under investigation in multiple laboratories (e.g., Zhang et al., 2024; Jin et al., 2024) [34,35].
We hypothesized that a significant correlation exists between elevated SeptiScores and positive blood culture results, and between low SeptiScores and negative blood culture results. To evaluate this hypothesis, we conducted a retrospective statistical analysis of data from three independent observational clinical studies. While recognizing that such correlations may be imperfect—and that low SeptiScores should not provide unwarranted reassurance in isolation—data supporting the hypothesis would nonetheless suggest that SeptiScores could help improve the efficiency of blood culture practice, for example, by informing patient selection for initial or repeat blood culturing.
2. Materials and Methods
2.1. Study Cohorts
Patients were derived from three independent observational clinical studies, herein called “510k”, “SeptAsTERS”, and “UGANDA”. The design of these clinical studies has been described in detail elsewhere (respectively, Miller et al., 2018; von der Forst et al., 2024; Blair et al., 2023) [36,37,38]. Figure 1 shows a flow diagram that describes the selection of patients included in this study.
Patient classification as “sepsis” versus “SIRS” was determined using one of two approaches, depending on study site and available resources. Method 1: In the 510k and SeptAsTERS studies, sepsis and non-infectious systemic inflammatory response syndrome (SIRS) were adjudicated via Retrospective Physician Diagnosis (RPD) [36], in which an external panel of physicians, independent of patient care, reviewed clinical data. This method aimed to minimize inter-site bias and to standardize diagnostic criteria, but may be constrained by incomplete documentation, absence of bedside context, and variability among panelists. Method 2: In the Ugandan study, diagnoses were based on attending physicians’ assessments at multiple time points. This approach leveraged direct clinical knowledge of patients, which enabled the detection of subtle features, although it carried a greater risk of site-specific bias.
2.1.1. The “510k” Study
The “510k” study, conducted at multiple sites in the USA and Europe, enrolled a total of 419 patients from the intensive care unit (ICU) who displayed SIRS and were suspected of sepsis. By consensus RPD, 154 (36.8%) of these patients were determined to have sepsis, and 224 (53.5%) were determined to have SIRS. There were 41 patients (9.8% of the total) who could not be classified unambiguously as sepsis or SIRS. These were considered “indeterminates” and are not included in the present analysis. Blood cultures were ordered on the basis of clinical judgment and accordingly were only taken if deemed necessary by the care team. Of the 154 patients classified as septic, 81 had blood cultures taken, and of these, 48 (59.3%) were blood culture-positive (see Figure 1). The comparator for classification as SIRS or sepsis in this study was consensus-based clinical adjudication by an external three-member panel of expert clinicians. The adjudication process has been described in detail in the online data supplement Part 3, in Miller et al., 2018 [36]. The RPD process generally conformed to the conceptual framework provided by the Sepsis-2 definition (Levy et al., 2003) [39]. The adjudicators did not have access to the SeptiCyte RAPID test results.
2.1.2. The “SeptAsTERS” Study
The “SeptAsTERS” study, conducted at a single hospital in Germany, enrolled 59 post-surgical ICU patients with SIRS and showing signs of clinical deterioration. A total of 34 (57.6%) were retrospectively determined to have sepsis, and 25 (42.4%) were determined to have SIRS (see Table 1). Blood cultures were ordered on the basis of clinical judgment and accordingly were only taken if deemed necessary by the care team. Of the 34 septic patients, 15 (44.1%) were blood culture-positive. The comparator for classification as SIRS or sepsis in this study was a post hoc assessment of all patients by three independent intensive care professionals, who were not involved in the study. The process followed a model similar to the one described in the online data supplement Part 3 by Miller et al. (2018) [36], based on FDA Guidance, and on publications by Klein Klouwenberg et al. [40,41]. Details of the post hoc assessment process are provided in von der Forst et al. (2024) [32]. The RPD process adhered largely to the conceptual framework of the Sepsis-2 definition (Levy et al., 2003) [39]. Nevertheless, the incorporation of organ-dysfunction criteria means that the resulting assessments also shared features with the Sepsis-3 framework [42]. The adjudicators did not have access to the SeptiCyte RAPID test results.
2.1.3. The “UGANDA” Study
The “UGANDA” study, performed at Fort Portal Regional Referral Hospital, Kabarole District, Western Uganda and ACESO Uganda (Makerere University, Walter Reed Program and Infectious Disease Institute), Kampala, Uganda, comprises a subset of a larger study which is described in Blair et al. (2023) [38]. The 167 adult patients considered here presented initially to hospital with clinical signs of SIRS and a suspicion of sepsis, and ultimately were recruited from the emergency department (ED) and from medical wards (as opposed to the ICU, as was the case for patients in the 510k and SeptAsTERS studies). Patients were excluded if they were aged < 18, weighed less than 40 kg, or were on chemotherapy, asplenic, immunosuppressed, or pregnant. As dictated by protocol, blood cultures were taken for every patient. The comparator for classification as SIRS or sepsis in this study was based on the sepsis-2 criteria (Levy et al., 2003) [39]. Patient evaluation was conducted by the on-site care team at multiple timepoints (screening, 0 h, 6 h, 24 h, and in some cases, 72 h). Of the 167 patients enrolled in this study, 134 (80.2%) were evaluated as sepsis/severe sepsis at presentation, and 3 (1.8%), although evaluated as sepsis/severe sepsis at presentation, were later retrospectively adjudicated as SIRS by an independent clinician. A total of 30 patients (18.0%) could not be classified as SIRS or sepsis, and therefore were designated “indeterminate” and not included in subsequent analyses. The adjudicators did not have access to the SeptiCyte RAPID test results.
2.1.4. The Ghanaian Supplement
To supplement the number of SIRS patients from Uganda and to include SIRS cases from a distinct African site, five additional SIRS patients from Ghana were added to the study. These patients were selected from “discovery cohort” participants in “An Observational Study of Sepsis in Kumasi, Ghana”, protocol number NMRC.2016.0004-GHA [43,44]. These patients had previously been adjudicated under the Sepsis-2 framework by an external physician panel and were determined to have non-infectious etiologies (i.e., not sepsis, and thus classified as SIRS under the definition used here). The adjudicators did not have access to the SeptiCyte RAPID test results. Aggregated clinical data for these five patients are provided in Supplement S1. However, a data use agreement did not permit the sharing of individual-level data for the Ghanaian participants, so their clinical values are not included in Table 1. Their SeptiScores, however, were available individually and are included in all figures.
2.2. SeptiCyte RAPID
SeptiCyte RAPID is a cartridge-based reverse transcription—quantitative polymerase chain reaction (RT-qPCR) test that quantifies the relative amounts of two mRNA transcripts (PLAC8, PLA2G7) from human blood samples. The test has regulatory clearances for use in adults in the USA and Europe, and for adults and children in Australia. The test was validated and shown to display consistent performance in a heterogeneous patient population of 419 ICU patients from the Netherlands and the U.S.A. (Balk et al., 2024a, 2024b) [29,30]. The validation cohort included immunosuppressed patients and patients with low white cell counts. SeptiCyte RAPID is run on the Idylla hardware platform, using version 1.2 of the test-specific software (Biocartis NV, Mechelen, Belgium). The test is performed by pipetting 0.9 mL of PAXgene-stabilized blood (corresponding to 0.24 mL of drawn blood), or 0.24 mL of EDTA anti-coagulated whole blood, into a custom cartridge, which performs all assay steps, including sample extraction/purification and RT-qPCR, for the detection and relative quantification of the PLAC8 and PLA2G7 mRNA transcripts. The SeptiCyte RAPID test results are calculated and presented automatically through a software-generated report, which includes a quantitative score (SeptiScore, range 0–15, see Figure 2). The SeptiScore is calculated as the difference between the RT-qPCR Cq values for PLA2G7 and PLAC8, and is positively correlated with sepsis probability. The test has a hands-on time of ~2 min and a turnaround time of ~1 h. In Supplement S13, we indicate the various combinations of Idylla console software version, SeptiCyte RAPID test software version, and SeptiCyte RAPID cartridge lots that were used in this study. The aggregate rate of invalid and failed runs (cases for which no results were generated for either PLAC8, PLA2G7, or the internal control) conformed to the test design specifications (<5% of runs).
2.3. Statistical Analysis
As this is a post hoc retrospective analysis of data from three independent studies, it has not been possible to define a ‘primary endpoint’. Instead, we test the hypothesis that a significant correlation exists between elevated SeptiScores and positive blood culture results, and between low SeptiScores and negative blood culture results.
2.3.1. Conventional Statistical Tests
Conventional statistical tests were mainly conducted with the ‘stats’ package, version 4.3.1 in R [45]. For simple two-group comparisons, p-values were calculated using a proportions test, and for multiple-group comparisons, p-values were calculated with Pearson’s chi-squared test (Table 1). Point bi-serial correlations were calculated using the ‘ltm’ package, version 1.2–0 in R [46].
2.3.2. Receiver Operating Characteristic (ROC) Curve Analysis
Receiver Operating Characteristic (ROC) curve analysis with calculation of area under the curve (AUC) values [47] was performed using the pROC package, version 1.19.0.1 in R [48]. Confidence intervals for AUC were calculated by the method of DeLong et al. [49] as implemented in pROC [43]. A conventional interpretation of ROC curves was used, in which AUC 0.70–0.80 was considered acceptable, 0.80–0.90 was considered good, and AUC 0.90–1.00 was considered excellent (see, e.g., Table 4 of Elkahwagy & Kiriacos, 2024) [50].
2.3.3. SeptiScore Binary Cutoffs
Figure 2 presents the accepted 4-band framework for interpreting SeptiCyte RAPID test results. We also performed binary analyses, in which a single cutoff at a predefined SeptiScore boundary (5.0, 6.2, 7.4, 11.4) is used to generate 2 × 2 tables and sensitivity/specificity tables. This is most useful for understanding the behavior of the SeptiCyte RAPID test at extreme values of the SeptiScore, such as in a high sensitivity regime with binary cutoff = 5.0, or a high specificity regime with binary cutoff = 11.4. In the binary analyses, the 95% confidence intervals (CI) for sensitivity and specificity were estimated by bootstrapping (Carpenter & Bithell, 2000) [51]. A two-sample proportion test was used to determine if differences between pairs of sensitivity values or specificity values were significant at the p < 0.05 level.
2.3.4. Probability Ratio Analysis
This study was conducted under the hypothesis that a significant correlation exists between elevated SeptiScores and positive blood culture results, and between low SeptiScores and negative blood culture results. A prediction that follows from this hypothesis is that the ratio of probabilities of BC(+) sepsis/BC(−) sepsis should increase in a monotonic fashion with increasing SeptiScore. This prediction was tested quantitatively in the following way.
From the pooled data, the numbers of BC(+) sepsis, BC(−) sepsis, and SIRS were counted in eleven adjacent SeptiScore intervals: 0–4, 4.1–5, 5.1–6, 6.1–7, 7.1–8, 8.1–9, 9.1–10, 10.1–11, 11.1–12, 12.1–13, 13.1–15. In each interval the probabilities of BC(+) sepsis and BC(−) sepsis were then calculated as follows:
The ratio R of these two quantities was computed and plotted as a function of SeptiScore. A monotonic increase in this ratio is indicated by R_i+1_/R_i_ > 1 where i is the index variable for the intervals defined above. To test if a trend of monotonic increase in R_i+1_/R_i_ was statistically significant, the Jonckheere–Terpstra Test [46] was used, with a web applet available at www.metricgate.com
3. Results
3.1. Patient Demographic, Clinical, and Laboratory Characteristics
Table 1 presents the demographic and clinical characteristics of the patients analyzed in the present study. As described in the flow diagram of Figure 1, a total of 652 patients suspected of sepsis were originally considered, comprising 419, 167, and 61 patients from the 510k, UGANDA, and SeptAsTERS studies, respectively, plus an extra five patients from a Ghanaian cohort that were added to supplement the number of available SIRS patients from the UGANDA study. For 41/419 (9.8%) of patients from the 510k study and 30/167 (18.0%) of patients from the UGANDA study, no unambiguous call of sepsis or SIRS could be made; these patients were therefore deemed “indeterminate” and excluded from further analysis. Of the 322 patients deemed septic, 73 were excluded because blood cultures were either not taken or blood culture results were not recorded (73/322 = 22.7%). A total of 506 patients were ultimately analyzed in the present study (blue boxes in Figure 1), comprising 249 with sepsis (consensus or site-adjudicated) and available blood culture results, and 257 with SIRS (consensus or adjudicated).
Besides the geographic differences in origin between the Ugandan, 510k, and SeptAsTERS cohorts, there were slight but statistically significant imbalances in the male/female ratio in both the 510k and SeptAsTERS cohorts (p < 0.04 each). A statistically significant difference (p < 0.001) was observed between the three studies for the sequential organ failure assessment (SOFA) score. Patients from the Uganda study had a lower median SOFA score (median 2) vs. patients from the 510k study (median 5) or the SeptAsTERS study (median 5).
Patient laboratory characteristics, based on sepsis/SIRS calls and blood culture status, for the three studies are presented in Supplements S2–S5. The median C-reactive protein (CRP) level was elevated in all three studies and did not differentiate sepsis from SIRS patients. CRP was highest in the SeptAsTERS study, which consisted exclusively of post-abdominal surgery patients. White blood cell (WBC) counts varied widely, from 300 to 57,000 cells/uL (510k study), 2000 to 75,000 cells/uL (UGANDA study), and 1300 to 63,000 cells/uL (SeptAsTERS study). In each study, the highest WBC counts were observed in the sepsis group as opposed to the SIRS group. Median SeptiScores for patients with positive blood cultures fell into SeptiScore Band 4 (>7.4) for all three studies.
Across all three studies, a total of 85 septic patients had positive blood cultures with similar proportions of Gram-positive and Gram-negative bacterial isolates. The 510k study had six patients with mixed culture results, in which both Gram-positive and Gram-negative bacteria were isolated. A detailed breakdown of how the positive blood culture sepsis calls distribute across the SeptiScore bands for each of the study cohorts is presented in Table 2.
3.2. Performance of SeptiCyte RAPID Compared to Blood Culture
We stratified patients on the basis of sepsis/SIRS status, blood culture result, and SeptiScore (Figure 3). In panels A, B, and C of this figure, the four SeptiScore bands are separated by vertical black lines, where Band 1 indicates the lowest risk of sepsis and Band 4 indicates the highest risk of sepsis. Panel A (red points) shows the distribution of SeptiScores (scale of 0–15) for 85 blood culture-positive patients diagnosed with sepsis. An important feature to note is that most (66/85 = 78%) of the patients fell into SeptiScore Band 4, with some patients displaying very high SeptiScores. Further details on the microbiology results for the five patients with the highest SeptiScores (12.9–15.0) are given in Supplement S6.
A second important feature to note about Panel A is that none of the BC(+) sepsis patients fell into SeptiScore Band 1. There were, however, eight (8/85 = 9.4%) such patients with SeptiScores in Band 2. These would be considered “false negatives” for sepsis if evaluated solely on the basis of their relatively low SeptiScores. These eight patients were spread across all three studies. Further details on the microbiology results for these patients can be found in Supplement S7. Both Gram-negative and Gram-positive bacteria were isolated. Four of the patients received antibiotics before the blood sample was drawn for SeptiScore measurement, which might explain their low SeptiScores. Four patients displayed long blood culture times to positivity (3d, 4d, 9d, 10d), arguing for contamination; these might be better placed in the sepsis BC(−) category of Panel B (below). However, two patients had infections (S. anginosus from central catheter, time to positivity 1 day; and K. pneumoniae, time to positivity 41 h) that were not obvious contaminants, were not pre-treated with antibiotics, and fell below the 10th percentile of the SeptiScore cumulative distribution for BC(+) sepsis (see Figure 3D below), and therefore should be flagged for further investigation.
Panel B (blue points) shows the distribution of SeptiScores for 164 sepsis patients who had blood cultures ordered with negative results, or who were positive for cultures other than from blood. Of the 164 patients retrospectively diagnosed with sepsis and with negative blood cultures, 126 (76.8%) had SeptiScores in Bands 3 or 4. Some of the BC(−) sepsis patients had quite extreme Band 4 SeptiScores; the five patients with the highest SeptiScores (12.1–13.1) are detailed in Supplement S8.
Another point to note is that 10 BC(−) sepsis patients had Band 1 SeptiScores. These comprise 6.1% of the 164 patients in the BC(−) sepsis category. Further details on these patients can be found in Supplement S9. Patients of the types represented in this category would seem to require further detailed investigation, because if they were truly septic, they would have been missed by an alert system based on either blood culture or SeptiCyte RAPID.
Panel C shows the distribution of SeptiScores for 252 SIRS patients that were blood culture-negative (gray dots) and for five blood culture-positive SIRS patients (red points). Of note is the high proportion of SIRS patients in Bands 1 and 2 (n = 175/257 = 68.1%). Further details on the microbiology results for the five BC(+) SIRS patients can be found in Supplement S10. The bacteria isolated from two BC(+) SIRS patients with low SeptiScores were considered by the RPD panelists to be not clinically relevant and possibly contaminants: Fusobacterium (8 days to positivity, no antibiotics given, SeptiScore 5.4); and coagulase-negative Staphylococcus aureus (6 days to positivity, no antibiotics given, SeptiScore 5.4).
There were also some BC(−) patients deemed SIRS, but with Band 4 SeptiScores. These are represented by the rightmost gray points in Panel C. Further details on a random selection of these patients are provided in Supplement S11.
Panels D and E present a quantification of the data from Panels A, B, and C in terms of SeptiScore density distributions and cumulative distributions, respectively. There is clearly an offset of the distributions in the direction SIRS < sepsis BC(−) < sepsis BC(+).
Based on the data presented in Figure 3, we next evaluated the diagnostic performance of SeptiCyte RAPID for differentiating patients who were retrospectively diagnosed with sepsis and blood culture-positive from those retrospectively diagnosed with SIRS in a patient population initially suspected of sepsis. Table 3 summarizes the results of this evaluation according to the SeptiScore Band. Of the 342 patients considered in this table, 85 were both septic and blood culture-positive, and 257 were determined to have SIRS. Patients with a SeptiScore falling between 7.4 and 15 (Band 4) had a positive likelihood ratio (LR+) of 5.88 for blood culture-positive sepsis (as compared to SIRS). In contrast, patients with a SeptiScore falling between 0 and 4.9 (Band 1) had an LR+ of 0. Further details, including LR+ calculations, are provided in Supplement S12. A more complete analysis of multi-cohort data in terms of positive and negative likelihood ratios will be presented in a separate publication.
Note that the LR+ values for BC(+) sepsis depend upon the composition of the group to which BC(+) sepsis is being compared. In our analysis, the comparator is the BC(−) SIRS group [patients of Figure 3C], consistent with the Intended Use of the SeptiCyte RAPID test (discrimination of sepsis vs. SIRS). Understandably, the LR+ values for BC(+) sepsis would be decreased if the BC(−) comparator group were expanded to include BC(−) sepsis patients [i.e., Figure 3B patients mixed in with Figure 3C patients]. However, in practice, this would not be a meaningful comparison because clinicians would be expected to use SeptiCyte to discriminate between sepsis and SIRS in accordance with the test’s Intended Use, not to discriminate between BC(+) sepsis and BC(−) sepsis.
We next performed additional analyses of SeptiCyte RAPID performance, including calculations of area under the receiver operating characteristic curve (ROC AUC), sensitivity, specificity, and Youden’s index, using data from the combined study cohorts. Figure 4A reproduces the data of Figure 3 in the form of box–whisker plots. Figure 4B presents three ROC curves for SeptiCyte RAPID performance for sepsis vs. SIRS discrimination depending on the septic patients’ blood culture results. The red curve represents BC(+) sepsis versus SIRS (AUC = 0.91). The blue curve represents BC(−) sepsis versus SIRS (AUC = 0.80). Finally, the black curve represents sepsis irrespective of blood culture results versus SIRS (AUC = 0.84). Figure 4C shows sensitivity (blue) and specificity (red) curves as a function of the SeptiScore, for the BC(+) versus SIRS patients. The two curves cross at a SeptiScore of 7.0 (Youden’s index). Band boundaries at 5.0, 6.2, and 7.4 are shown as vertical black lines. Figure 4D presents a plot of 11 incremental calculations of the relative probabilities of BC(+) sepsis/BC(−) sepsis, as a function of SeptiScore. As the SeptiScore increases, the relative probability of a septic patient being BC(+) as opposed to BC(−) also increases. The correlation between increasing SeptiScore and increasing probability ratio is statistically significant according to the Jonckheere–Terpstra trend test [52] as indicated by test statistic value J = 52.5 and p-value: 9.92 × 10^−5^. At a SeptiScore of 10, the ratio of probabilities increases above 1 (dotted line in figure). That is, septic patients with SeptiScores >10 have a higher probability of being BC(+) compared to BC(−).
Figure 5 presents sensitivity and specificity calculations for BC(+) sepsis and BC(−) sepsis versus SIRS for binarized models with single cutoffs at the predefined SeptiScore Band boundary (5.0, 6.2, 7.4) and also at 11.4. This figure is derived from the more complete ROC curve analysis of Figure 4B. Considering BC(+) sepsis versus SIRS, for a binary cutoff at SeptiScore 5.0 the sensitivity was 100%, and for a binary cutoff at SeptiScore 11.4, the specificity was 100%. That is, based on the patients considered in this study, no patients with SeptiScores less than 5.0 were retrospectively BC(+) sepsis, and no patients with SeptiScores greater than 11.4 were retrospectively SIRS.
4. Discussion
The current reference standard for diagnosing BSI is blood culture. However, blood culture practice and interpretation of results have a number of limitations, including low positive rates, contamination, and a lack of timeliness. Downstream implications from these limitations include unnecessary antibiotic use, an increase in overall mortality and antimicrobial resistance, increased pharmacy and laboratory costs, and length of hospital stays (Butler 2023, Fabre 2025, Dempsey 2019) [13,18,20]. A number of interventions as part of blood culture diagnostic stewardship have been described, including careful patient selection and efforts to keep contamination rates less than or equal to a target rate of 1% of all blood cultures taken (Fabre 2020, Schinkel 2023, Doern 2019, CLSI M47) [27,53,54,55]. Therefore, it can be argued that blood culture practice is currently suboptimal and there is a need for improved BC stewardship (Fabre, 2025) [18].
In this study, we conducted a post hoc retrospective analysis of patients suspected of sepsis, representing diverse populations across multiple continents (North America, Europe, and Africa). We have shown a positive correlation between sepsis likelihood, measured using SeptiCyte RAPID, and the likelihood of blood culture positivity. From our study of 506 patients, of whom 16.8% (n = 85) were blood culture-positive, our results showed that patients with SeptiScores greater than 10 had a higher probability of being BC(+) sepsis than BC(−) sepsis. Further, patients with SeptiScores less than 5.0 had a 0% probability of being BC(+) sepsis (Figure 4C). On the basis of this finding, we hypothesize that positive blood cultures in patients with SeptiScores less than 5.0 are likely to be either contaminants or not relevant to a sepsis diagnosis.
The blood culture positivity rate in our study (16.8%) was higher than the 5.6% to 7.3% recently reported in a large study involving 362,327 blood cultures conducted between 2019 and 2020 in 19 USA hospitals (Fabre 2025) [18]. The higher positivity rate in our study may relate to unintentional bias in patient selection, since the patients in all three cohorts examined here were enrolled on the basis of being critically ill. It might also reflect an unduly high rate of culture contamination. (For comparison, in the 2025 Fabre study [18], the contamination rate was 1.5% of all blood cultures taken, which equates to ~24% contamination rate for positive cultures.) The overall contamination rate in our study could not be accurately calculated because a blood culture was not taken from every patient. However, out of a total of 85 blood culture-positive results, there were three that were retrospectively diagnosed with SIRS that had low SeptiScores and were thus considered to be either contaminants or not relevant to a sepsis diagnosis (3.5% of all positive cultures).
As shown in Figure 4A,B, the ROC AUC for using SeptiScore to distinguish SIRS from BC(+) sepsis was 0.91. The corresponding likelihood ratio (LR) for blood culture positivity among patients with Band 4 SeptiScores was 5.88. Notably, no BC(+) patients retrospectively diagnosed with sepsis had SeptiScores in Band 1. Collectively, these findings indicate that SeptiCyte RAPID demonstrates strong performance for discriminating BC(+) sepsis from SIRS. Although its ability to discriminate BC(–) sepsis from SIRS was lower, it remained diagnostically meaningful (ROC AUC 0.80). In our study, all patients with SeptiScores >11.4 were either BC(+) septic or BC(–) septic. Further inspection of the data revealed four patient subgroups warranting additional consideration.
-
BC(−) sepsis with high SeptiScores: Of the 164 patients classified as septic by RPD with negative blood cultures, 85/164 (51.8%) had SeptiScores in Band 4, and 126/164 (78.6%) had SeptiScores in either Band 3 or Band 4 (Figure 3B). Thus, SeptiScores tended to be elevated even in cases of apparent non-bacteremic sepsis. Cases of culture-negative sepsis are well known and have received significant attention (Phua et al., 2013; Thorndike & Kollef, 2020; Li et al., 2021; Chang et al., 2024) [56,57,58,59]. It is recognized that some septic events may not be bacteremic in nature, and may instead be due to localized (non-bloodborne) bacterial infections, or to infections from other types of pathogens (viral, fungal, parasitic) (Chang et al., 2024; Lee et al., 2024; Xu et al., 2024) [59,60,61]. Given these possibilities, high SeptiScores could potentially help guide diagnostic stewardship by providing motivation for more aggressive attempts to identify causative pathogens, including additional blood cultures, culturing of patient samples other than blood, or use of rapid molecular viral panel tests.
-
BC(+) sepsis with low SeptiScores: Of the 85 patients classified as septic by RPD with positive blood cultures, none had SeptiScores in Band 1, and eight (8/85 = 9.4%) had SeptiScores in Band 2 (Figure 3A). SeptiScores in Band 2 would be considered relatively low values for patients who were truly septic and blood culture-positive. However, closer examination of the microbiology results for these eight patients showed that four had prior antibiotic exposure, which may have influenced the patients’ systemic immune response to bacterial threats. Additionally, four of the patients had long time-to-positivity (3, 4, 9, and 10 days), which may indicate that the positive blood culture results were in fact due to contamination. Such results suggest that many factors need to be taken into consideration when interpreting the clinical relevance of SeptiCyte RAPID and blood culture results, including the timing of blood draws, effect of antibiotics, time to positivity, organism isolated, potential for contamination, other clinical parameters and laboratory results, and patient trajectory (whether the patient is becoming better or worse).
-
BC(−) SIRS with high SeptiScores: Of the 252 patients classified as SIRS by RPD with negative blood cultures, 32 exhibited Band 4 SeptiScores (32/252 = 12.7%) (Figure 3C). This suggests that, in some cases, factors other than sepsis may lead to elevated SeptiScores, consistent with the view that SeptiScores should not be interpreted in isolation, but preferably together with other available clinical data. By way of example (see Supplement S11 for further detail), a patient with a high (Band 4) SeptiScore of 7.7 with no initial confirmed site of infection nonetheless had an RPD call of SIRS. The patient was prescribed a combination of antibiotics for 2.6 days after presentation, but ultimately (at 2.6 days) was diagnosed by PCR as having Epstein–Barr Virus in the blood. A high SeptiScore in this patient, especially if obtained early in a diagnostic workup, may have provided diagnostic stewardship with respect to determining a viral etiology.
-
BC(+) SIRS with low SeptiScores: Of the 257 patients classified as SIRS by RPD, three had SeptiScores in Band 1 or Band 2 and had positive blood cultures (3/257 = 1.2%) (Figure 3C). By way of example (see Supplement S10 for further detail), one patient with a low (Band 2) SeptiScore of 5.4 had a positive blood culture for Staphylococcus aureus. Normally, identification of this known pathogen from blood culture might suggest that the patient had sepsis of a bacterial etiology. However, no site of infection was identified initially, there was a long time-to-positivity (6 days), and no antibiotics were prescribed. The patient was ultimately called SIRS by RPD, and the low SeptiScore was consistent with this diagnosis. Contamination would be the most likely explanation for blood culture positivity in this case.
A practical point to note is that SeptiCyte RAPID results are available within one hour and in the same time frame as WBC data. Such a timeframe is significantly shorter than the reported median time to blood culture positivity of 15.7 h (Lambregts et al., 2019) [15]. Furthermore, SeptiCyte RAPID results are available at least 12 h prior to gaining any blood culture results and within the 3 h period recommended by the Surviving Sepsis Campaign (Evans et al., 2021) [62] for administration of antibiotics for patients suspected of sepsis (without shock).
Some potential clinical uses of SeptiCyte RAPID for informing blood culture practice are presented in Table 4. However, we recognize that the clinical utility of SeptiCyte RAPID for informing blood culture practice still needs to be rigorously demonstrated in a prospective, cluster-randomized stewardship trial, to include safety endpoints such as missed bacteremia, ICU transfer, and 7/30-day mortality.
For patients with high SeptiScores (>7.4, Band 4) and positive blood culture results, SeptiCyte RAPID could potentially be repeated to confirm a diagnosis and to rule out metastatic spread. For patients with high SeptiScores and negative blood culture results, more intense efforts could be made to identify a causative pathogen, including the use of multiple blood culture sets and molecular diagnostic syndromic panels. High SeptiScores might also be an indication that the antibiotic treatment is not effective.
For patients with low SeptiScores (<5.0, Band 1) and positive blood cultures, contamination could be considered, or alternatively, bacteremia in the absence of sepsis. Examples of transient or even persistent bacteremia in the absence of sepsis are well known, e.g., due to periodontitis or periodontal procedures (Everett & Hirschmann, 1977; Takai et al., 2005; Lockhart et al., 2008; Horliana et al., 2014) [63,64,65,66]. For patients with low SeptiScores and negative blood culture results, alternative diagnoses (other than sepsis) should be considered.
Further clinical utility for SeptiCyte RAPID could lie in determining whether follow-up blood cultures (FUBC) are needed. It is likely that, in standard clinical practice, additional blood cultures would be drawn if a patient continued to deteriorate. FUBC are generally also collected after the occurrence of a positive blood culture with a known pathogen that matches the clinical presentation to monitor the persistence or clearance of bacteremia or to determine antibiotic sensitivity or resistance profiles. FUBCs are suggested in the management of Staphylococcus aureus bacteremia, endocarditis, and candidemia (Liu 2011, Baddour 2015, Pappas 2016 [67,68,69]. However, there is controversy as to the utility of FUBC in patients with Gram-negative BSI (Ong et al., 2024) [70]. SeptiCyte RAPID results obtained within 1–2 h of testing could provide guidance on whether, or to what extent, FUBCs are warranted.
Our study has several limitations. First, despite enrolling over 500 patients, there were only 85 septic patients with confirmed positive blood cultures (85/506 = 16.8% positivity), which may limit the generality of conclusions drawn. However, the study spanned several geographic regions (North America, Europe, Africa) and enrolled patients with diverse comorbidities, and with WBC counts ranging from neutropenic to above normal. Similar blood culture positivity rates, isolated pathogens, and SeptiScore distributions for each of the three separate studies suggest that our results and conclusions could be applied more broadly. It should be recognized, though, that the African cohort was recruited and assessed with a relatively well-controlled clinical trial, which may be atypical of the usual level of care available in this LMIC setting. An in-depth comparison of results from the three geographic areas (North America, Europe, Africa) is ongoing and will be presented in a future publication. A second limitation was that in the 510k study, blood cultures were taken at the discretion of the attending clinician. That is, not every enrolled patient had a blood culture taken. Patients with complicated diagnoses such as pneumonia with possible sepsis may not always have triggered blood culture orders (Kim et al., 2023) [71], and patients with low-level bacteremia may not have undergone extensive enough blood sampling (Lee et al., 2007) [72], and so may have been ‘missed’. Calculations of blood culture positivity and contamination rates are therefore not necessarily accurate for a population of patients merely suspected of sepsis. Third, the exact timing for blood culture and SeptiCyte RAPID sampling was not known for all patients. Therefore, the influence of antibiotics on blood culture and SeptiCyte RAPID results could not be established with certainty, nor could an exact correlation between blood culture and SeptiCyte RAPID results be determined. A fourth limitation was the use of different reference methods to adjudicate sepsis versus SIRS across study sites: the 510k and SeptAsTERS cohorts were assessed via the RPD method, while the Ugandan cohort relied on site-based adjudication. As a result, estimates of SeptiCyte RAPID’s performance for distinguishing BC(+) sepsis from confirmed SIRS may be less certain for the Ugandan cohort than for the 510k and SeptAsTERS cohorts. Fifth, there may have been some selection bias, for example, under the decision to exclude patients with “indeterminate” diagnoses instead of forcing these patients into the sepsis or SIRS categories (Figure 1). Sixth, there is disagreement in the field about the utility of using “SIRS” as a reference category in the diagnosis of sepsis. The 2016 Sepsis-3 consensus reoriented sepsis definitions toward organ-dysfunction-based criteria, thereby reducing the prominence of SIRS in this capacity (Singer et al., 2016) [73]. Nevertheless, many clinicians, specialty societies, and investigators continue to support the use of SIRS criteria for early clinical screening, for maintaining continuity with historical epidemiologic data, or for specific care settings where SIRS retains operational value (Balk, 2014; Simpson, 2018; Schefzik et al., 2023) [74,75,76]. Because the field has not reached a uniform position on the role of SIRS in defining or contextualizing sepsis, some uncertainty is introduced into the quantitative comparisons presented here, and this lack of consensus may limit the degree to which the present analysis attains broad, universal acceptance. Finally, SeptiCyte RAPID provides a likelihood of sepsis based on a SeptiScore range of 0–15 and is pathogen agnostic. In future prospective usage of the test, high SeptiScores could be due to a viral or parasitic infection rather than a bacterial or fungal infection as detected by culture. Therefore, caution would need to be taken with respect to interpreting high SeptiScores, which indicate a higher likelihood of sepsis rather than just culture-positive bacterial or fungal infection.
5. Conclusions
SeptiCyte RAPID test results (SeptiScores) are positively correlated with the likelihood of blood culture positivity. This finding could facilitate diagnostic stewardship with respect to patient selection and interpretation of positive blood culture results. Early diagnosis and identification of causative pathogens in patients suspected of BSI and sepsis is expected to improve patient outcomes through early and more targeted treatment. Significant potential benefits are expected in diverse clinical settings, including in poorly resourced or challenging environments such as LMIC healthcare settings, mass-casualty scenarios, and prolonged field care settings during military operations. Further work could involve determining the generalizability of these results, including whether SeptiScores correlate to the likelihood of different types of infection (e.g., Staphylococcus, endocarditis, Gram-negative BSI, viruses, fungi, malaria). Ultimately, the clinical utility of SeptiCyte RAPID for diagnostic stewardship will be established through interventional studies and measurement of impact on patient outcomes, hospital costs, and antibiotic stewardship.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ziegler M.J. Pellegrini D.C. Safdar N. Attributable mortality of central line associated bloodstream infection: Systematic review and meta-analysis Infection 201543293610.1007/s 15010-014-0689-y 25331552 · doi ↗ · pubmed ↗
- 2Reunes S. Rombaut V. Vogelaers D. Brusselaers N. Lizy C. Cankurtaran M. Labeau S. Petrovic M. Blot S. Risk factors and mortality for nosocomial bloodstream infections in elderly patients Eur. J. Intern. Med.201122 e 39e 4410.1016/j.ejim.2011.02.00421925041 · doi ↗ · pubmed ↗
- 3Stewart A.G. Simos P. Sivabalan P. Escolà-VergéL. Garnham K. Isler B. on behalf of the ESGBIES Study Group An Update on Recent Clinical Trial Data in Bloodstream Infection Antibiotics 202413103510.3390/antibiotics 1311103539596730 PMC 11591257 · doi ↗ · pubmed ↗
- 4Becker J.U. Theodosis C. Jacob S.T. Wira C.R. Groce N.E. Surviving Sepsis in Low-Income and Middle-Income Countries: New Directions for Care and Research Lancet Inf. Dis.2009957758210.1016/S 1473-3099(09)70135-519695494 · doi ↗ · pubmed ↗
- 5Ni P. Le Y. Challenges in the Management of Sepsis in a Resource-Poor Setting Int. J. Clin. Med.2017841242110.4236/ijcm.2017.86039 · doi ↗
- 6Chen Z. Tian Y. Liu J. Ran J. Sun S. Zhao S. Ge Y. Martinez L. Chen X. Cao P. COVID-19 and sepsis-related excess mortality in the US during the first three years: A national-wide time series study Am. J. Epidemiol.20241942219222910.1093/aje/kwae 41139479803 · doi ↗ · pubmed ↗
- 7Shappell C.N. Klompas M. Chan C. Chen T. Kanjilal S. Mc Kenna C. Rhee C. CDC Prevention Epicenters Program Use of Electronic Clinical Data to Track Incidence and Mortality for SARS-Co V-2–Associated Sepsis JAMA Netw. Open.20236 e 233572810.1001/jamanetworkopen.2023.3572837773495 PMC 10543118 · doi ↗ · pubmed ↗
- 8Keven K. Ates K. Sever M.S. Yenicesu M. Canbakan B. Arinsoy T. Ozdemir N. Duranay M. Altun B. Erek E. Infectious complications after mass disasters: The Marmara earthquake experience Scand. J. Infect. Dis.20033511011310.1080/003655402100002701312693561 · doi ↗ · pubmed ↗