Strain Analysis from Transverse CMR Cine Imaging in Congenital Heart Disease: Feasibility, Reproducibility, and Comparison to Global Longitudinal Strain
Victoria Zieschang, Peter Kramer, Collin Götze, Sebastian Kelle, Regina Stegherr, Alireza Khasheei, Felix Berger, Johannes Nordmeyer, Titus Kühne, Sarah Nordmeyer, Marie Schafstedde

TL;DR
This study explores a new way to measure heart muscle strain using transverse CMR images, finding it reliable and potentially useful for patients with congenital heart disease.
Contribution
The study introduces transverse strain (TrS) as a novel, reproducible method for strain assessment in congenital heart disease patients.
Findings
TrS showed high intra- and interobserver reproducibility in patients with congenital heart disease.
TrS had strong agreement with GLS in Fontan patients and ToF patients' right ventricles.
TrS showed a positive bias compared to GLS in left ventricles of ToF patients and healthy controls.
Abstract
Background: Global longitudinal strain (GLS), derived from long-axis cine images (LAX), is a sensitive marker for myocardial dysfunction and a strong predictor for clinical events and future ventricular deterioration. In patients with complex congenital heart disease (CHD) transverse-oriented cine imaging is part of the standard cardiac magnetic resonance (CMR) protocol. We aimed to study the feasibility and reproducibility of strain measurements derived from transverse-oriented cine images (Transverse Strain (TrS)) and compare them with standard GLS. Methods: We retrospectively analyzed CMR cine images from 40 patients (n = 20 Fontan, n = 20 Tetralogy of Fallot (ToF)) and 10 healthy controls. Strain analysis was performed in every subject using both the conventional GLS and the TrS approach. Results: TrS showed high intra- and interobserver reproducibility in patients with CHD…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
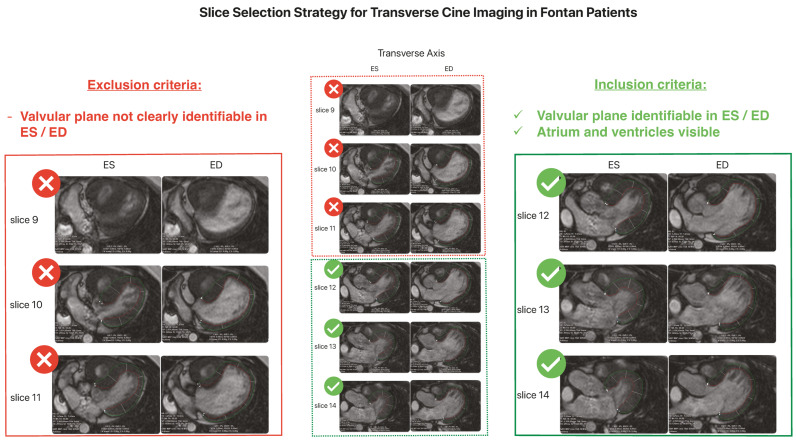 Figure 1
Figure 1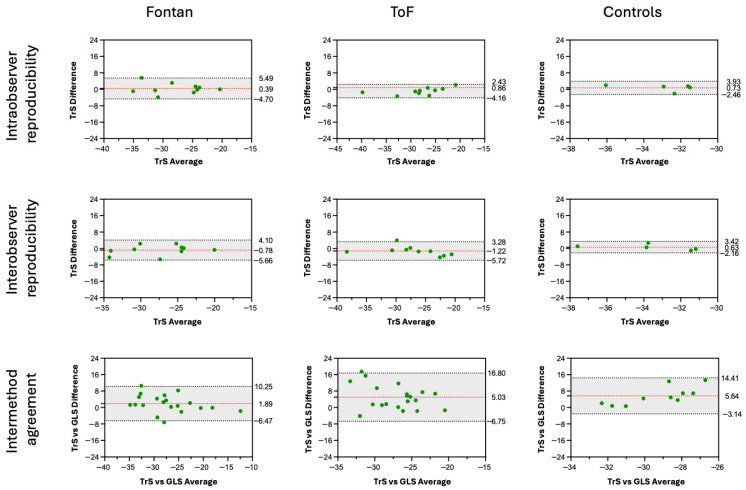 Figure 2
Figure 2- —Charité—Universitätsmedizin Berlin
- —Berlin Institute of Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Function and Risk Factors · Congenital Heart Disease Studies · Cardiac Valve Diseases and Treatments
1. Introduction
Global longitudinal strain (GLS) derived from feature-tracking in cardiac magnetic resonance (CMR) imaging is a sensitive marker for subclinical myocardial dysfunction and an established predictor of adverse outcomes across various cardiac diseases [1,2,3,4]. In line with this, the large prospective HERZCHECK trial further highlighted the clinical relevance of CMR-derived GLS by using it as the central imaging parameter for screening and risk stratification of asymptomatic individuals at risk for heart failure [5]. Standardized GLS quantification is typically performed from left ventricular (LV) long-axis (LAX) cine views (2-, 3-, and 4-chamber), while right ventricular (RV) strain is conventionally derived from the 4-chamber view [6,7,8].
In CMR protocols for patients with complex congenital heart disease (CHD), such as those with univentricular physiology, standardized LAX cine acquisitions for GLS can be technically challenging or suboptimal to perform due to the presence of a morphologic right systemic ventricle, abnormal ventricular orientation, atypical looping, and non-standard atrioventricular alignment [9,10,11]. As a result, consistent and reproducible LAX planes are often difficult to obtain, limiting the applicability of conventional GLS analysis. Although consensus recommendations outline disease-specific CMR protocols in CHD, including long-axis views for tetralogy of Fallot (ToF) and Fontan patients [9] protocols vary between centers and are frequently adapted to local expertise in CMR techniques, patients’ anatomy, surgical history, and clinical indication [12], which can lead to incomplete or absent LAX datasets. For example, in patients with ToF, imaging typically focuses on right-ventricular size, function, and the right-ventricular outflow tract [13], so dedicated LAX acquisitions are often not included in standard protocols.
These anatomical and protocol-related limitations are also reflected in the literature, where the absence of suitable long-axis datasets has led Strodka et al. [14] to rely on transverse cine stacks for strain estimation. The group used axial cine images as substitutes for missing four-chamber views in Fontan patients, highlighting the broader clinical need for an alternative, anatomy-independent orientation for myocardial strain assessment in CHD.
Transverse-oriented cine images, however, are routinely acquired as part of standard CMR protocols across all CHD subtypes [9]. This imaging plane provides full ventricular coverage independent of cardiac orientation and allows for comprehensive assessment of both ventricles and adjacent vascular structures within a single stack [10]. In patients with ToF, transverse-oriented cine images capture the entire right ventricle and outflow tract, which are critical for postoperative evaluation, whereas in patients with Fontan circulation, they enable visualization of the complex systemic and pulmonary venous pathways and extracardiac conduits within one continuous anatomical dataset [11,15,16].
Since transverse-oriented cine images have been—and continue to be—routinely acquired in CMR examinations of patients with CHD, whereas LAX images have not necessarily been, it is of interest to determine whether strain derived from transverse-oriented cine images (Transverse Strain (TrS)) may also serve as a feasible and reliable marker for myocardial contractility.
Accordingly, the aim of this study was to evaluate left- and right-ventricular strain derived from transverse-oriented cine images and, for the first time, to assess its reproducibility and compare it with conventional GLS in patients with CHD (including univentricular anatomy and ToF) as well as in healthy controls.
2. Materials and Methods
2.1. Study Population and Design
This retrospective study included 50 subjects who underwent CMR at our institution between 2015 and 2021, with CMR protocols that included LAX cine images and cine images in transverse slice orientation suitable for strain analysis. The study population consisted of three groups: 20 patients after Fontan operation (12 female, 8 male), 20 patients after ToF repair (11 female, 9 male), and 10 healthy controls (6 female, 4 male) without known cardiovascular disease. Healthy controls were selected from individuals referred for CMR to exclude structural heart disease and who showed normal cardiac anatomy and function.
All patients or their legal guardians gave informed consent by signing the institution’s broad consent form for retrospective analysis of clinical and imaging data.
Inclusion criteria were the availability of transverse-oriented cine images and LAX (2-, 3-, and 4-chamber views) cine acquisitions of sufficient quality for feature-tracking strain analysis. Exclusion criteria included incomplete cine datasets, poor image quality (e.g., severe artifacts such as motion artifacts or device-related artifacts in patients with pacemakers or implantable cardioverter-defibrillators), or CHD diagnoses that did not fit the predefined groups. Mean age was 16 ± 6.5 years in the Fontan group, 26 ± 13.4 years in the ToF group, and 15 ± 5.1 years in the control group. In the Fontan group, 75% of patients had a systemic left ventricle, 25% a systemic right ventricle. An overview of the patient characteristics, including sex, age, volumetric parameters, ejection fraction, and cardiac index, is provided in Table 1. Additional detailed clinical characteristics of the Fontan cohort are provided in the Supplementary Material (Table S1).
2.2. CMR Acquisition and Functional Analysis
All included routine clinical CMR examinations were performed on a 1.5-T scanner (Achieva, Philips Healthcare, Best, The Netherlands). The datasets typically comprised cine steady-state free-precession sequences acquired in short-axis (SAX) orientation for ventricular volumetry, LAX views (2-, 3-, and 4-chamber), and transverse cine image stacks. Typical acquisition parameters showed only minor variations between examinations and included a repetition time (TR) of approximately 3.0 ms, an echo time (TE) of approximately 1.5 ms, an in-plane spatial resolution of about 1.0–1.5 × 1.0–1.5 mm^2^, a slice thickness of 6–8 mm, and approximately 20–30 cardiac phases per cardiac cycle.
Functional analysis was performed using QMass (v1.4.0.158, Medis Medical Imaging Leiden, The Netherlands). End-systolic (ES) and end-diastolic (ED) phases were visually selected on SAX and transverse-oriented cine images. Endocardial and epicardial contours were manually traced from base to apex for volumetric analysis of both ventricles in ToF patients and healthy controls, as well as of the systemic ventricle and—if distinguishable—the hypoplastic ventricle in Fontan patients. Papillary muscles and trabeculae were excluded from ventricular volumes and from ventricular mass calculations. Ventricular end-diastolic volume, end-systolic volume, and mass were derived from SAX stacks as the standard reference for functional assessment. Stroke volume and ejection fraction of the ventricles were calculated automatically. Height and weight were obtained to determine body surface area (BSA), and ventricular volumes and mass were indexed to BSA. Cardiac index was calculated accordingly.
2.3. Strain Analysis/CMR Feature-Tracking
CMR feature-tracking analysis was performed using QStrain (QSTRAIN 1.4.0.158, Medis Medical Imaging Leiden, The Netherlands).
CMR feature-tracking was performed using two methods in every subject:
- GLS, expressed as a negative value, represents base-apex shortening and is derived by averaging the peak strain values of individual segments using the 17-segment model [17]. GLS analysis of the systemic or left ventricle was performed using LAX (2-, 3-, and 4-chamber) cine images, and GLS of the hypoplastic or right ventricle from a single LAX (4-chamber) image. Analysis was conducted automatically and manually by tracing the endocardial and epicardial borders in ES and ED across all required planes.
- TrS was performed using transverse-oriented cine images. For standardizing purposes, we chose to include only images with clearly detectable atria, ventricles, and atrioventricular plane in both ES and ED. The atrioventricular plane served as the anatomical base for contouring. Slices in which the atrioventricular plane was not clearly identifiable in either phase were excluded.
From the available transverse-oriented cine images, up to three slices meeting all criteria were selected independently by two observers. A maximum of three slices was predefined to ensure methodological feasibility and reasonable post-processing time. Depending on individual anatomy and image quality, one to three eligible slices were available. The mean number (±SD) of analyzed slices was 3.0 ± 0 for Fontan patients (median 3), 2.7 ± 0.5 for ToF patients (median 3), and 2.2 ± 0.4 for controls (median 2) for observer 1. Corresponding values for observer 2 were 3.0 ± 0 for Fontan patients (median 3), 2.9 ± 0.3 for ToF patients (median 3), and 2.4 ± 0.8 for controls (median 3).
Endocardial and epicardial borders were manually traced from the atrioventricular plane (base) to the apex in ES and ED using QStrain. In patients with septal defects, an imaginary contour line was drawn across the defect if needed. TrS was calculated as the mean of all strain values from the selected slices.
This process is illustrated in Figure 1, which shows the slice selection strategy from transverse-oriented cine images, including typical inclusion and exclusion criteria.
2.4. Statistical Analysis
All analyses were performed using IBM SPSS Statistics, V29.0.2.0. A p-value < 0.05 was considered statistically significant.
The agreement between strain measurements derived from LAX and transverse cine images, as well as intra- and interobserver reproducibility of TrS analysis, is summarized descriptively for each patient group based on the intraclass correlation coefficient (ICC), mean difference, limits of agreement, and Pearson correlation coefficient (r), visualized using Bland–Altman plots (Figure 2).
The following levels of agreement were used: excellent for ICC > 0.75, good for ICC 0.6–0.74, fair for ICC 0.4–0.59, poor for ICC < 0.4 [18].
Half of each patient group (10 Fontan, 10, ToF, 5 healthy controls) was reanalyzed 6 months after the first analysis by the first observer, blinded to the results of the first analysis. The same dataset (10 Fontan, 10, ToF, 5 healthy controls) was analyzed by a second observer who was blinded to the results of the first observer.
Detailed results are summarized in Section 3. Additional TrS analyses are available in the Supplementary Materials (Tables S2–S4), showing similar trends.
3. Results
3.1. Intra- and Interobserver Reproducibility
Intra- and interobserver reproducibility of TrS analysis was good to excellent across all patient groups, with consistently high reproducibility in Fontan and ToF patients (Table 2 and Table 3). In Fontan patients, reproducibility was excellent for both single ventricle (SV) and hypoplastic ventricle (HV) (all ICC ≥ 0.82). Similarly, ToF patients showed excellent agreement for the LV (intra-/interobserver ICC = 0.95/0.91) and good to excellent agreement for the RV (ICC = 0.81/0.80). In the control group, intraobserver reproducibility was excellent for the RV (ICC = 0.96) and good for the LV (ICC = 0.68, p = 0.08). Interobserver agreement in controls was lower overall, with excellent reproducibility in the LV (ICC = 0.86).
3.2. Intermethod Comparison Between TrS and GLS
Intermethod agreement between TrS and GLS varied across patient groups (Table 4). Mean differences were calculated as GLS − TrS; therefore, positive values indicate more negative TrS values compared with GLS. In Fontan patients, good to excellent agreement between both methods was observed for both ventricles, especially in the systemic ventricle (ICC = 0.75), with only small systematic differences. In ToF patients, agreement between TrS and GLS was excellent for the RV (ICC = 0.78), whereas LV agreement was poor, with TrS values showing a notably more negative strain than GLS (mean difference = 5.03). In healthy controls, agreement between both methods was poor, with weak correlations and consistently more negative TrS values compared to GLS. Bland–Altman plots illustrating these findings are shown in Figure 2, with additional analyses provided in the Supplementary Materials (Figures S1 and S2).
4. Discussion
This study demonstrates that strain measurements derived from transverse cardiac cine images (TrS) offer high intra- and interobserver reproducibility and might be an applicable method for quantifying myocardial contractility and deformation. In Fontan patients with either a morphological left or right systemic ventricle, and in the right ventricle of Fallot patients, TrS values were even comparable to intraindividual GLS values. In the left ventricle of ToF patients and in both ventricles of healthy controls, however, TrS values were significantly more negative than GLS values.
4.1. Reproducibility
TrS measurements demonstrated good to excellent intra- and interobserver reproducibility across all patient groups, reinforcing their reliability for possible clinical evaluation and use. The standardized use of up to three well-defined transverse cine images per subject contributed to this consistency and may serve as a guideline for future application.
4.2. Intermethod Agreement and Systematic Bias
Good agreement was seen between TrS and GLS values in the ventricles of patients with Fontan circulation and in the RV of patients with repaired ToF. This consistent intermethod agreement, although unexpected at first, may be explained by an altered myocyte arrangement in these ventricles resulting from congenital abnormalities and remodeling induced by volume and/or pressure load. In Fallot patients after surgical correction, altered ventricular geometry, RV remodeling due to chronic pressure and/or volume overload, and diffuse, partly asynchronous deformation patterns have been described [19,20,21,22]. Similarly, in Fontan patients, non-uniform and directionally inconsistent myocardial motion of the single ventricle has been reported [23,24]. These abnormalities in myocyte arrangement might lead to a less organized contraction pattern compared with structurally normal ventricles and may explain why strain measurements, although derived from different image orientations (standard LAX cine images vs. transverse-oriented cine images), yield similar values.
Together, these findings suggest that in CHD patients with fundamentally altered myocardial mechanics, strain measurements become less dependent on imaging orientation. This may account for the high intermethod agreement observed in both the RV of ToF patients and in the univentricular hearts of Fontan patients. This interpretation is based on the present findings and should be interpreted as a hypothesis, given that it was not specifically evaluated within the current study design.
In contrast, systematic differences with more negative TrS than GLS and poor correlation were observed in the left ventricle of ToF patients and in both ventricles of healthy controls. This indicates that TrS may not be suitable for direct comparison with GLS in structurally normal ventricles and therefore should be regarded as an independent deformation parameter rather than a substitute for GLS. Importantly, agreement estimates in the control group should be interpreted with caution, as the small sample size and the inherently low interindividual variability in healthy subjects may affect ICC calculations and may partly explain the negative ICC values observed.
The consistently more negative strain values observed with TrS likely reflect a combination of factors, including inclusion of myocardial regions with high contractility (e.g., the lateral wall) [25], orientation misalignment of strain vectors relative to fiber direction, and the broader deformation pattern sampled in transverse planes.
Standard longitudinal cine images primarily capture longitudinal deformation, whereas transverse-oriented cine images intersect the ventricular myocardium orthogonally and may capture components of longitudinal, circumferential, and rotational motion. This broader deformation coverage, together with the inclusion of myocardial regions with high contractility, such as the lateral wall, may explain the differences seen between TrS and GLS values [25].
4.3. Clinical Relevance
GLS has demonstrated prognostic significance in various cardiovascular diseases and is known to outperform traditional volumetric parameters like ejection fraction in detecting early myocardial dysfunction [1,2]. Although consensus recommendations provide guidance on disease- and anatomy-specific CMR protocols in congenital heart disease [9], including the recommended long-axis views for ToF or Fontan patients—these guidelines remain recommendations rather than strict standards. In clinical practice, CMR protocols are frequently adapted to the individual patient’s anatomy, surgical history, and clinical questions, and minimized in duration, which can result in incomplete or absent long-axis datasets even when they are formally recommended. Accordingly, Strodka et al. [14] used transverse cine images when long-axis datasets were not available. Such approaches demonstrate that missing LAX images are a practical reality in some CHD cohorts and underline the need for validated alternative strain methods.
By enabling strain measurements in patients for whom conventional methods are limited or unavailable, TrS measurements could enhance risk stratification, monitoring, and treatment planning in CHD and may provide an additional marker of myocardial function, particularly for the early detection of ventricular dysfunction prior to changes in ejection fraction.
Another noteworthy advantage of using TrS analysis instead of or next to GLS in CHD would be the possibility to perform large-scale retrospective longitudinal studies, since transverse cardiac cine images are largely available in multiple sites around the world for multiple years, offering a potential large cohort to study myocardial contractility and clinical outcome [9,26,27].
Thus, TrS provides a novel and practical solution to extend strain-based evaluation to patients who would otherwise be excluded from strain analysis. Further longitudinal studies are required to assess whether TrS values correlate with clinical outcomes and adverse events in this specific population.
4.4. Limitations
This study has several limitations. The relatively small sample size, particularly in the control group, may have limited statistical power and increased the risk of type II error. Moreover, the retrospective single-center design may have introduced selection bias and limited the generalizability of the results.
Methodological limitations are mainly related to the TrS approach. In contrast to the standard 17-segment GLS model, TrS is based on a limited number of transverse slices and does not provide complete ventricular coverage, which may have influenced strain measurements. Although slice selection followed predefined criteria, a certain degree of observer dependence cannot be fully excluded. In addition, strain analysis is software-dependent and therefore not interchangeable across different post-processing platforms.
Finally, all strain values were derived using a feature-tracking approach. Consequently, the present results reflect feature-tracking–based strain and are not directly comparable to strain measurements obtained with other techniques, such as myocardial tagging. Furthermore, the lack of established reference values for TrS currently limits its immediate clinical applicability.
4.5. Validation and Future Directions
While the results are promising, broader validation remains essential. Larger studies across different institutions and patient populations are needed to confirm the method’s reliability and to establish population-specific reference values for TrS. The study also emphasizes the need for tailored software tools, such as specific segmentation models and algorithms optimized for TrS analysis, to improve applicability.
While several studies have established the feasibility and prognostic value of GLS in pediatric and adult CHD [3,23,28,29], to date, no study has evaluated the use of TrS for strain assessment in this population. The present study adds novel evidence, demonstrating that TrS is not only reproducible but also correlates well with the gold standard in selected CHD subgroups. Reported ICC values for reproducibility compare favorably with published LAX-based studies, further supporting the methodological validity of TrS measurements [30,31].
5. Conclusions
This study demonstrates that TrS is a feasible and reproducible method for myocardial strain analysis in patients with CHD, particularly in those with non-standard anatomy such as Fontan circulation or the right ventricles of patients with corrected ToF. Across all study groups, TrS showed high intra- and interobserver reproducibility, confirming the consistency of the method, thereby underscoring its utility for longitudinal monitoring and its suitability for standardized application in structurally complex anatomies.
Intermethod agreement between TrS and GLS was high in Fontan patients and in the RV of Fallot patients, supporting the use of TrS as a potential alternative to GLS in these subgroups. In contrast, TrS yielded consistently more negative strain values in both ventricles of healthy controls and in the LV of Fallot patients, indicating that in these groups, TrS should not be used interchangeably with GLS and should be instead interpreted as an independent deformation parameter.
To further establish the clinical role of TrS, future studies should define reference values across diverse populations and cardiac pathologies, explore the relationship between TrS and clinical outcomes, and validate the method in larger, multicenter cohorts.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kalam K. Otahal P. Marwick T.H. Prognostic implications of global LV dysfunction: A systematic review and meta-analysis of global longitudinal strain and ejection fraction Heart 20141001673168010.1136/heartjnl-2014-30553824860005 · doi ↗ · pubmed ↗
- 2Romano S. Judd R.M. Kim R.J. Kim H.W. Klem I. Heitner J.F. Shah D.J. Jue J. White B.E. Indorkar R. Feature-Tracking Global Longitudinal Strain Predicts Death in a Multicenter Population of Patients With Ischemic and Nonischemic Dilated Cardiomyopathy Incremental to Ejection Fraction and Late Gadolinium Enhancement JACC Cardiovasc. Imaging 2018111419142910.1016/j.jcmg.2017.10.02429361479 PMC 6043421 · doi ↗ · pubmed ↗
- 3Schäfer M. Mitchell M.B. Frank B.S. Barker A.J. Stone M.L. Jaggers J. von Alvensleben J.C. Hunter K.S. Friesen R.M. Ivy D.D. Myocardial strain-curve deformation patterns after Fontan operation Sci. Rep.2023131191210.1038/s 41598-023-39226-y 37488167 PMC 10366156 · doi ↗ · pubmed ↗
- 4Korosoglou G. Sagris M. AndréF. Steen H. Montenbruck M. Frey N. Kelle S. Korosoglou G. Sagris M. AndréF. Systematic review and meta-analysis for the value of cardiac magnetic resonance strain to predict cardiac outcomes Sci. Rep.202414109410.1038/s 41598-023-50835-538212323 PMC 10784294 · doi ↗ · pubmed ↗
- 5Kelle S. Nolden A.C. Muller M.L. Beyer R.E. Steen H. Remppis B.A. Wieditz J. Kentenich H. Tuit A. Cvetkovic M. Rationale and design of the HERZCHECK trial: Detection of early heart failure using telemedicine and cardiovascular magnetic resonance in structurally weak regions (NCT 05122793)J. Cardiovasc. Magn. Reson.20252710184110.1016/j.jocmr.2025.10184139824461 PMC 11870244 · doi ↗ · pubmed ↗
- 6Scatteia A. Baritussio A. Bucciarelli-Ducci C. Strain imaging using cardiac magnetic resonance Heart Fail. Rev.20172246547610.1007/s 10741-017-9621-828620745 PMC 5487809 · doi ↗ · pubmed ↗
- 7Andre F. Steen H. Matheis P. Westkott M. Breuninger K. Sander Y. Kammerer R. Galuschky C. Giannitsis E. Korosoglou G. Age- and gender-related normal left ventricular deformation assessed by cardiovascular magnetic resonance feature tracking J. Cardiovasc. Magn. Reson.2015172510.1186/s 12968-015-0123-325890093 PMC 4355347 · doi ↗ · pubmed ↗
- 8Taylor R.J. Moody W.E. Umar F. Edwards N.C. Taylor T.J. Stegemann B. Townend J.N. Hor K.N. Steeds R.P. Mazur W. Myocardial strain measurement with feature-tracking cardiovascular magnetic resonance: Normal values Eur. Heart J.—Cardiovasc. Imaging 20151687188110.1093/ehjci/jev 00625711353 · doi ↗ · pubmed ↗