Investigation of the relationship between pain, fear of movement and falling in geriatric patients
Ümmühan Meltem Öztürk, Mümin Polat

TL;DR
This study explores how pain, fear of movement, and fear of falling are connected in older adults and how they impact daily life.
Contribution
The study provides empirical evidence of the interrelationship between pain, kinesiophobia, and fear of falling in geriatric patients.
Findings
Women reported higher pain levels than men, with statistically significant differences.
A strong positive correlation was found between kinesiophobia and fear of falling.
Pain, fear of movement, and fear of falling collectively hinder daily functioning in older adults.
Abstract
Falls among older adults represent a major public health concern and are strongly associated with pain, fear of falling, and fear of movement. Pain may increase fall risk in a dose-response manner, while fear of falling can limit mobility, further enhancing vulnerability. This study aimed to investigate the interrelationship between pain, kinesiophobia, and fear of falling in geriatric patients. A descriptive cross-sectional study was conducted in the Physical Therapy Unit of Burdur State Hospital, Turkey, between March 2022 and March 2023. A total of 100 participants aged ≥65 years were recruited by random sampling. Data collection included sociodemographic characteristics, fall history, chronic diseases, and regular medication use. Pain was assessed using the Visual Analog Scale (VAS) and Verbal Category Scale, kinesiophobia using the Tampa Kinesiophobia Scale, and fear of falling…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
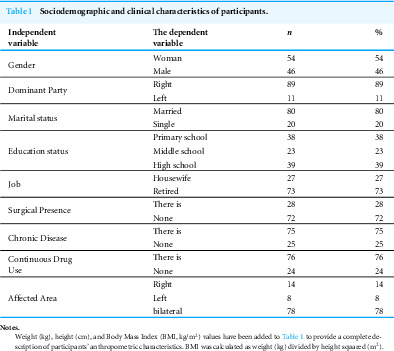 Figure 1
Figure 1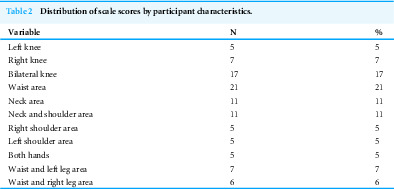 Figure 2
Figure 2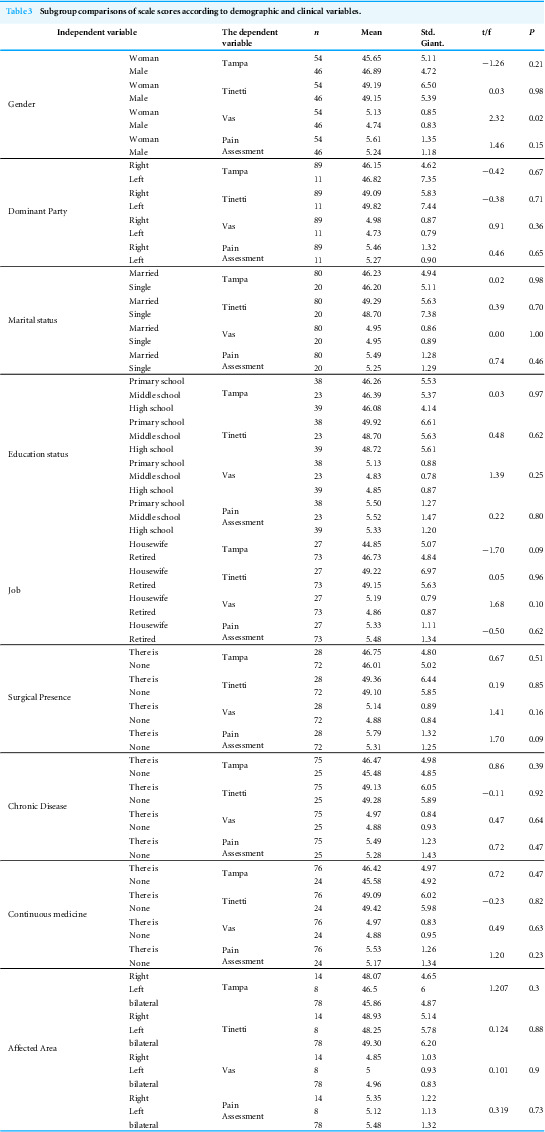 Figure 3
Figure 3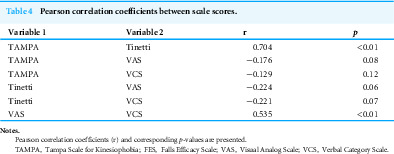 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBalance, Gait, and Falls Prevention · Musculoskeletal pain and rehabilitation · Injury Epidemiology and Prevention
Introduction
Aging encompasses progressive, irreversible structural and functional changes that occur at the system, organ, tissue, and cellular levels. The World Health Organization (WHO) defines it as a decreased ability to adapt to environmental stressors, with old age beginning at 65 years of age (Tümerdem, 2006). Increasing life expectancy worldwide has made active aging a global health priority, emphasizing independence in daily activities, preservation of physical function, and prevention of age-related complications (Tambağ, 2013; Howcroft et al., 2017).
Pain, fear of falling, and fear of movement (kinesiophobia) are interrelated problems frequently observed in the geriatric population. Pain has been shown to have a dose–response relationship with falls, whereby higher pain intensity is associated with increased fall risk (Stubbs et al., 2014; Gell & Patel, 2019). Fear of falling, even in the absence of previous falls, is prevalent among older adults and can lead to activity restriction, functional decline, and increased frailty (Legters, 2002; Zijlstra et al., 2007; Scheffer et al., 2008). Similarly, kinesiophobia may result in avoidance of movement due to fear of pain or re-injury, which in turn perpetuates inactivity, muscle weakness, and reduced balance (Tunca Yılmaz et al., 2011; Vincent et al., 2013; Merchant et al., 2022). These behavioral responses contribute to a vicious cycle that exacerbates fall risk and diminishes quality of life in older adults.
Recent peer-reviewed evidence further emphasizes the multidimensional nature of pain-related movement fear. A comprehensive scoping review published in PeerJ identified key conceptual and methodological trends regarding kinesiophobia among health professionals, highlighting its clinical relevance across diverse practice settings (Doutre et al., 2024). Consistently, Ertem (2025) demonstrated that individuals with ankylosing spondylitis exhibit significantly higher levels of kinesiophobia, which are closely associated with greater pain intensity and functional impairment. Moreover, Chantanachai et al. (2022) examined fall risk factors among community-dwelling older adults with mild cognitive impairment, reporting that both psychological and physical domains jointly contribute to fall susceptibility. Together, these recent studies reinforce the interrelationship between pain, fear of movement, and fall risk in geriatric populations.
Given the complexity of fall risk, recent research highlights the need for personalized preventive approaches that address not only physical but also psychological and behavioral factors (Delbaere et al., 2004; Todd & Skelton, 2004). Despite the recognition of these associations, the combined relationship between pain, fear of falling, and fear of movement in older adults remains underexplored, particularly in community-dwelling populations in Turkey.
Therefore, the present study aimed to investigate the interrelationships between pain, kinesiophobia, and fear of falling in individuals aged 65 years and older. By identifying how these factors interact, we sought to contribute to the development of targeted strategies for fall prevention and quality-of-life improvement in the geriatric population.
Materials & Methods
Study design and setting
This study was designed as a descriptive cross-sectional study and was conducted between March 2022 and March 2023 in the Physical Therapy Unit of Burdur State Hospital, located in southwestern Turkey. The study was to evaluate the interrelationship between pain, kinesiophobia, and fear of falling in geriatric patients.
Participant sampling
A total of 213 patients aged 65 years and above who applied to the physical therapy outpatient clinic were evaluated for eligibility. Participants were selected using a simple random sampling method. The required sample size was estimated using G*Power version 3.1, with an effect size of 0.40, α = 0.05, and power (1–β) = 0.90. The calculation was based on an analysis of variance (ANOVA) fixed effects model. The estimated sample size was 102, considering 20% attrition; the final sample included 100 participants after exclusions due to incomplete data.
Inclusion and exclusion criteria
Participants were included in the study if they were aged 65 years or older, were able to walk independently or with the use of assistive devices, had no diagnosed cognitive impairment or neurological disorders such as Alzheimer’s disease or Parkinson’s disease, and voluntarily agreed to participate. Individuals were excluded from the study if they had an acute illness during the data collection period, had severe visual or hearing impairments that could hinder questionnaire completion, or refused to provide informed consent.
Participant demographics
The sample consisted of 100 individuals (mean age: 70.58 ± 4.54 years). Sociodemographic data collected included gender, age, marital status, education level, occupation, dominant body side, history of surgery, presence of chronic diseases, and regular use of medication. Body mass index (BMI) was calculated using reported height and weight.
Data collection procedure
Data were collected through face-to-face structured interviews conducted by the lead researcher in a private consultation room within the hospital. The survey tools were administered in the same order for all participants to ensure consistency. Each session lasted approximately 20–30 min. Participants were encouraged to ask questions if they did not understand any items.
Measurement instruments
Fear of falling was assessed using the Tinetti Falls Efficacy Scale (FES), a validated instrument widely used in older populations. Fear of movement was evaluated with the Tampa Scale for Kinesiophobia (TAMPA), for which the Turkish validity and reliability have previously been established. Pain intensity was measured using two standardized tools: the Visual Analog Scale (VAS) and the Verbal Category Scale (VCS), both of which are commonly used in geriatric populations. In addition, a sociodemographic data form was used to collect information on age, gender, marital status, education level, occupation, fall history, comorbidities, and regular medication use.
Ethical considerations
Ethical approval was obtained from the Burdur Mehmet Akif Ersoy University Clinical Research Ethics Committee (Approval No: YL21-486). Institutional permission was granted by the Burdur State Hospital administration. All participants provided written informed consent prior to inclusion in the study. Participation was voluntary, and individuals could withdraw at any stage without any consequences.
Statistical analysis
Data were analyzed using Statistical Package for the Social Sciences (SPSS) version 23. Normality was assessed with the Kolmogorov–Smirnov test. Descriptive statistics were calculated as mean ± standard deviation and frequency (%). Group comparisons were performed using Student’s t-test and one-way ANOVA with Tukey’s post-hoc tests. Bivariate associations among scale scores were examined with Pearson correlation coefficients. A two-sided p < 0.05 was considered statistically significant. Multivariable regression was not conducted in the present study.
Results
Detailed descriptive statistics are presented in Tables 1–3; below we summarize only the key findings. A total of 100 individuals participated in the study. The mean age was 70.58 ± 4.54 years. The mean height was 165.09 ± 0.6 cm, and the mean weight was 77.62 ± 7.03 kg. The average symptom duration was 3.79 ± 1.09 years (Table 1).
Table 1: Sociodemographic and clinical characteristics of participants.
Group comparisons showed that female participants reported higher VAS pain scores than males (p < 0.05), whereas Tinetti, TAMPA/TSK, and VCS scores did not differ significantly by sex (p > 0.05). No significant differences were observed across dominant side, marital status, education, occupation, chronic disease, or medication use. Participants with a history of surgery had higher mean values across scales, but these did not reach statistical significance. See Table 2 for full estimates. These subgroup comparisons (Table 2) align with the study’s main objective by illustrating how demographic and clinical factors may influence the interplay between pain, fear of movement, and fear of falling in older adults.
Table 2: Distribution of scale scores by participant characteristics.
Table 3: Subgroup comparisons of scale scores according to demographic and clinical variables.
The distribution of affected regions is shown in Table 3. The distribution of affected regions was as follows: left knee, right knee, both knees, lower back, neck, neck and shoulder, right shoulder, left shoulder, both hands, lower back and left leg, and lower back and right leg (Table 3).
When the gender variable was evaluated, the mean TAMPA score was higher among male participants, while the mean scores of the Tinetti, VAS, and Pain Assessment scales were higher among female participants. While the differences in TAMPA, Tinetti, and Pain Assessment scores were statistically insignificant (p > 0.05), the difference in VAS scores was statistically significant (p < 0.05).
When the dominant side variable was assessed, the mean VAS and Pain Assessment scores were higher on the right side, whereas TAMPA and Tinetti scores were higher on the left side. The differences in the scale scores based on dominant side were statistically insignificant (p > 0.05).
For the marital status variable, the mean VAS scores were equal in both married and single participants. TAMPA, Tinetti, and Pain Assessment scores were higher on average among married participants. The differences between these scores and marital status were not statistically significant (p > 0.05).
Regarding educational attainment, the mean VAS and Tinetti scores were higher among those with primary school education, while TAMPA and Pain Assessment scores were higher among those with secondary school education. These differences were statistically insignificant (p > 0.05).
In the comparison of occupational status with the dependent variables, TAMPA and Pain Assessment scores were higher among retired participants, while Tinetti and VAS scores were higher among housewives.
For the surgical history variable, those who had undergone surgery had higher mean scores in TAMPA, Tinetti, VAS, and Pain Assessment compared to those who had not.
When chronic disease was evaluated, participants with chronic illness had higher TAMPA, VAS, and Pain Assessment scores, while participants without chronic disease had higher Tinetti scores. These differences were not statistically significant (p > 0.05).
In terms of regular medication use, participants who continuously used medication had higher TAMPA, VAS, and Pain Assessment scores than those who did not. The Tinetti score was higher among those who did not use medication regularly. These differences were statistically insignificant (p > 0.05).
Regarding the affected region, higher TAMPA scores were observed in those with right-side involvement, higher VAS scores in those with left-side involvement, and higher Tinetti and Pain Assessment scores in those with bilateral involvement. These differences were also not statistically significant (p > 0.05).
Scale correlations (Pearson correlation)
A positive correlation was found between TAMPA and Tinetti scores (+0.704). The correlation between TAMPA and VAS scores was negative (−0.176), as was the correlation between TAMPA and Pain Assessment scores (−0.129). The correlation between Tinetti and VAS scores was also negative (−0.224), as was the correlation between Tinetti and Pain Assessment scores (−0.221). A positive correlation was found between VAS and Pain Assessment scores (+0.535) (Table 4). Pearson correlations between scales are provided in Table 4, which summarizes the strength and direction of associations among pain, fear of movement, and fear of falling measures. Significant relationships are highlighted in the text where relevant.
Table 4: Pearson correlation coefficients between scale scores.
Subgroup analyses were conducted for gender, dominant side, marital status, education level, and occupation because these variables are well-documented risk factors for falls in older adults (Todd & Skelton, 2004; Masud & Morris, 2001). However, no significant differences were observed across subgroups (p > 0.05).
Discussion
This study examined the interrelationship between pain, fear of movement, and fear of falling in older adults. Our results indicated that female participants reported significantly higher pain scores compared to males, while no significant differences were observed in Tinetti, TAMPA, or pain assessment scales. These findings are consistent with previous reports that women are more likely to experience chronic pain and falls compared to men (Todd & Skelton, 2004). The relationship between gender and fall risk highlights the need for gender-sensitive prevention strategies.
Pain is a well-established determinant of falls in the elderly. Consistent with previous studies, our results support the notion that pain contributes to reduced activity, balance problems, and higher fall risk (Stubbs et al., 2014; Gell & Patel, 2019). The observed positive correlation between pain severity and fear-related outcomes suggests that pain not only impairs mobility but also exacerbates psychological concerns, reinforcing the cycle of inactivity and vulnerability. Fear of movement (kinesiophobia) and fear of falling are maladaptive responses commonly observed among older adults. In our study, TAMPA scores showed a strong correlation with Tinetti scores, confirming earlier research indicating that fear of movement limits participation in daily activities and increases fall risk (Zijlstra et al., 2007; Scheffer et al., 2008; Tunca Yılmaz et al., 2011). Moreover, avoidance behaviors associated with fear of falling have been shown to contribute to further functional decline, reduced mobility, and frailty. Our findings emphasize that interventions should not only target physical risk factors but also address psychological dimensions. The subgroup analyses presented in Table 2 further support the main objective of our study by demonstrating that sociodemographic and clinical variables, including gender, education level, and chronic disease status, may influence pain and movement-related fear. Although these associations were not statistically significant, the observed tendencies align with the conceptual model linking physical and psychological domains in fall risk among older adults. Interestingly, although both VAS and VCS are validated pain assessment tools, only VAS scores demonstrated statistical significance. This discrepancy may be attributed to the continuous nature and higher sensitivity of the VAS, which allows for finer gradations of pain intensity compared to the categorical VCS. Additionally, older adults may perceive and report pain differently when constrained to verbal categories, potentially leading to less variability in VCS scores. The strong positive correlation between TAMPA and Tinetti scores highlights the reciprocal relationship between movement fear and functional performance. This suggests that interventions aiming to reduce kinesiophobia could also enhance balance confidence and mobility, which are critical components in fall prevention programs.
Although subgroup analyses for chronic disease did not reveal statistically significant differences, trends were in line with previous findings. Chronic illness has been associated with greater fatigue, reduced activity, and impaired balance (Karataş & Maral, 2010; Schnelle et al., 2012). Fatigue in elderly populations has also been linked to sleep disturbances and lack of physical exercise (Schultz-Larsen & Avlund, 2007). Interventional studies have shown that structured physical activity improves sleep quality and reduces fatigue (Ferris et al., 2005; Reid et al., 2010). Considering that fatigue and poor sleep are also linked to fall risk and mortality (Bloom, Ahmed & Alessi, 2009; Onat et al., 2013), these parameters warrant greater attention in geriatric assessments.
Physical activity plays a critical role in maintaining balance and mobility. Previous studies demonstrated significant improvements in strength and balance following structured exercise interventions (Lee & Park, 2013; Soyuer, Şenol & Şenol, 2012). In our study, although occupation and activity levels were not significant predictors, trends supported the established literature that sedentary individuals have poorer outcomes compared to physically active peers (Fortuño-Godes, Guerra-Balic & Cabedo-Sanromà, 2013). Taken together, these findings suggest that exercise-based interventions should be prioritized for fall prevention.
The use of assistive devices is considered both a risk factor and a preventive strategy. While elderly individuals with gait or balance impairments are more prone to falls, assistive devices can help stabilize mobility when appropriately prescribed (Fink, Wyman & Hanlon, 2003; Rao, 2005; Erdoğmuş & Tüzün, 2001). Our findings support the view that careful assessment and tailored prescription of assistive devices are critical for reducing fall risk.
Falls remain a major public health concern. Globally, they are among the leading causes of mortality and morbidity in older adults (Berg et al., 1997; Tideiksaar, 1988). Fear of falling has been reported in 12–65% of community-dwelling elderly without prior falls, and up to 92% among those with a history of falls (Legters, 2002). This highlights the substantial psychological burden even beyond actual fall events. Our findings align with the broader literature, showing that pain, psychological factors, and physical inactivity together perpetuate fall risk in aging populations.
This study has some limitations, including its cross-sectional design, single-center setting, and relatively small sample size, which may reduce generalizability and statistical power. Nevertheless, the integration of multiple scales (VAS, VCS, TAMPA, Tinetti) provided a comprehensive evaluation of pain, fear of movement, and fear of falling. Future longitudinal and interventional studies are needed to establish causal relationships and evaluate the effectiveness of multidisciplinary programs.
In conclusion, this study demonstrated that pain intensity, fear of movement, and fear of falling are interrelated constructs that contribute to mobility limitations in older adults. Although some associations did not reach statistical significance, the observed trends suggest that increased pain and kinesiophobia may negatively affect functional performance and confidence in balance. These findings emphasize the importance of comprehensive geriatric assessments that address both physical and psychological factors in fall prevention. Future research with larger and more diverse samples, including regression-based analyses, is recommended to clarify the causal pathways between pain, movement fear, and fall risk.
Conclusions
Aging is one of the health-related challenges that affects all body systems particularly the musculoskeletal system resulting in a sense of inadequacy, disability, and loss of workforce, and is becoming increasingly prevalent. While technological advancements continue to make daily life easier for individuals, they also contribute to a sedentary lifestyle and reduced levels of physical activity. Furthermore, risk factors such as smoking, obesity, poor posture, and strenuous working conditions are known contributors to chronic pain. Over time, impaired posture, muscle weakness, spasms, and pain diminish the quality of life and the ability to perform daily activities among geriatric patients. Cognitive functions and emotional states are also significantly affected in patients experiencing chronic pain, leading to delays in the initiation of rehabilitation.
Among the preventive measures for chronic conditions, proper nutrition programs stand out as essential. A balanced and healthy diet increases resistance to disease and significantly lowers the risk of illness.
Fear of movement, also known as kinesiophobia, has recently drawn attention from researchers as a factor contributing to persistent pain and the limitation of daily activities in geriatric patients. Pain in elderly individuals often cannot be explained by clinical findings alone. Instead, behavioral, social, perceptual, and physical factors are believed to play a role. Reduced physical activity leads to decreased physical fitness, which in turn may contribute to the development of diabetes, obesity, and cardiovascular diseases. Additionally, living in social isolation often leads to psychological problems in elderly individuals.
Identifying kinesiophobia in geriatric patients and understanding its connection with quality of life are critical steps toward improving their well-being and promoting activity participation. Encouraging appropriate physical activity among elderly individuals can help reduce sedentary behavior and mitigate the associated health risks. It is well established that elderly individuals who exercise regularly experience lower levels of kinesiophobia. Therefore, engaging elderly individuals in regular group-based exercise programs can increase participation and adherence. Educational initiatives focused on specific health topics can also raise awareness and positively influence the quality of life. Elderly individuals who become more informed tend to incorporate this knowledge into their daily lives, improving self-care.
Additionally, those who engage in their own housework remain more physically active throughout the day. Thus, encouraging older adults to perform household tasks is important for maintaining daily activity levels.
This study demonstrated that pain intensity and kinesiophobia are important correlates of fear of falling among older adults. Although fear of movement and falling are common, they are modifiable through appropriate interventions. Incorporating regular exercise, balance training, and psychological support into geriatric care may reduce these fears and improve quality of life. Future studies using longitudinal and intervention designs could further clarify these relationships. These findings collectively emphasize the multifactorial nature of pain, movement fear, and fall risk in older adults. Addressing these interrelated factors through targeted physical activity programs and psychosocial support could help improve mobility and reduce fall incidence in geriatric populations.
Limitations
This study has several limitations. First, the cross-sectional design prevents causal inferences. Second, the single-center setting may limit the generalizability of findings. Third, although bivariate analyses provided meaningful insights, regression models were not performed to adjust for potential confounders such as age, gender, and comorbidities. Future research could incorporate regression-based models to better adjust for potential confounding variables. Finally, the sample size was relatively modest, which may have limited the detection of smaller effects. Future studies should employ multivariable regression models to adjust for potential confounding factors (e.g., age, sex, comorbidities) and to test the robustness of the observed associations.
Future research
Future research should further investigate the causal pathways between pain, kinesiophobia, and fear of falling in older adults. Longitudinal and interventional studies are needed to determine whether reducing pain and movement fear can directly lower fall risk. Moreover, integrating objective mobility measures and psychosocial interventions into future designs would help clarify how physical and psychological factors interact in fall prevention.
Supplemental Information
10.7717/peerj.20661/supp-1Supplemental Information 1Dataset and codebook
10.7717/peerj.20661/supp-2Supplemental Information 2STROBE checklist
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Berg WP Alessio HM Mills EM Tong C 1997 Circumstances and consequences of falls in independent community-dwelling older adults Age and Ageing 2626126810.1093/ageing/26.4.2619271288 · doi ↗ · pubmed ↗
- 2Bloom HG Ahmed I Alessi CA 2009 evidence based recommendations for the evaluation and management of sleep disorders in older persons Journal American Geriatric Society 5776178910.1111/j.1532-5415.2009.02220.x PMC 274812719484833 · doi ↗ · pubmed ↗
- 3Chantanachai T Taylor ME Lord SR Menant J Delbaere K Sachdev PS Kochan NA Brodaty H Sturnieks DL 2022 Risk factors for falls in community-dwelling older people with mild cognitive impairment: a prospective one-year study Peer J 10e 1348410.7717/peerj.1348435663527 PMC 9161814 · doi ↗ · pubmed ↗
- 4Delbaere K Crombez G Vanderstraeten G Willems T Cambier D 2004 Fear-related avoidance of activities, falls oath physical frailty. A prospective community-based cohort study Age and Aging 33436837310.1093/ageing/afh 10615047574 · doi ↗ · pubmed ↗
- 5Doutre L Beaumier M Parent A-A Talbot S Tremblay M 2024 Kinesiophobia among health professionals’ interventions: a scoping review Peer J 12e 1793510.7717/peerj.1793539184383 PMC 11344999 · doi ↗ · pubmed ↗
- 6ErdoğmuşCB Tüzün S 2001 Walking kinematics in the elderly Geriatrics 413339
- 7Ertem U 2025 Ankylosing spondylitis and kinesiophobia Peer J 13e 1903410.7717/peerj.1903439959836 PMC 11830361 · doi ↗ · pubmed ↗
- 8Ferris LT Williams JS Shen CL O’Keefe KA ve Hale KB 2005 Resistance training improves sleep quality in older adults: a pilot study Journal of Sports Science and Medicine 435436024453540 PMC 3887339 · pubmed ↗