Lower Selenoprotein P Is Independently Associated with Peripheral Arterial Disease in Peritoneal Dialysis
I-Min Su, Chung-Jen Lee, Chiu-Huang Kuo, Chih-Hsien Wang, Bang-Gee Hsu

TL;DR
Low levels of a protein called Selenoprotein P are linked to peripheral arterial disease in patients on peritoneal dialysis, suggesting it could be a useful biomarker.
Contribution
This study identifies Selenoprotein P as an independent biomarker for peripheral arterial disease in peritoneal dialysis patients.
Findings
Low Selenoprotein P levels were independently associated with peripheral arterial disease in peritoneal dialysis patients.
Selenoprotein P correlated positively with ankle-brachial index measurements.
Patients with peripheral arterial disease had significantly lower Selenoprotein P concentrations.
Abstract
Background/Objectives: Peripheral arterial disease (PAD) is a common yet often unrecognized complication in patients receiving peritoneal dialysis (PD). Considering that ankle–brachial index (ABI) can be difficult to interpret in this population, additional vascular biomarkers are needed. Selenoprotein P (SePP) is a major selenium transport protein with antioxidant and metabolic regulatory functions and may reflect vascular stress relevant to PAD. We investigated the association of circulating SePP levels with ABI-defined PAD in patients on PD. Methods: In this cross-sectional analysis of 98 patients on PD, ABI was assessed using an automated oscillometric device, and ABI < 0.9 was defined as ABI-defined PAD. Serum SePP levels were measured using enzyme-linked immunosorbent assay. Results: ABI-defined PAD was identified in 20 patients (20.4%). Compared with patients with normal ABI,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
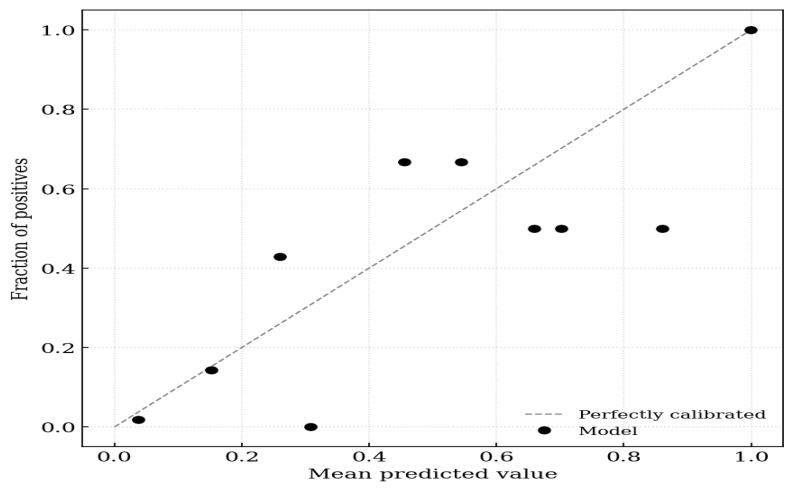 Figure 1
Figure 1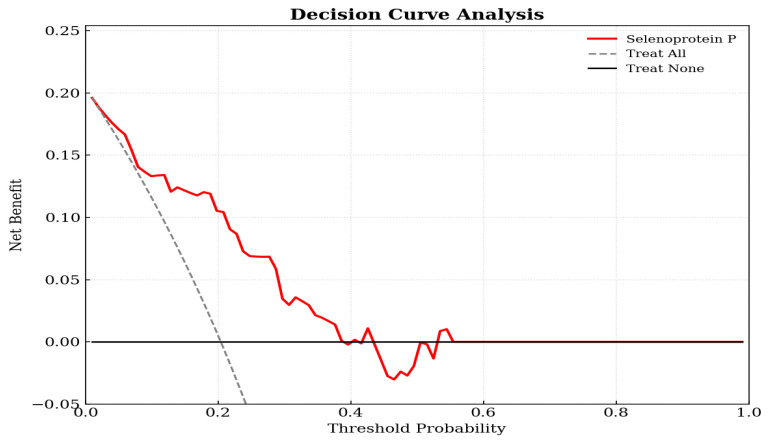 Figure 2
Figure 2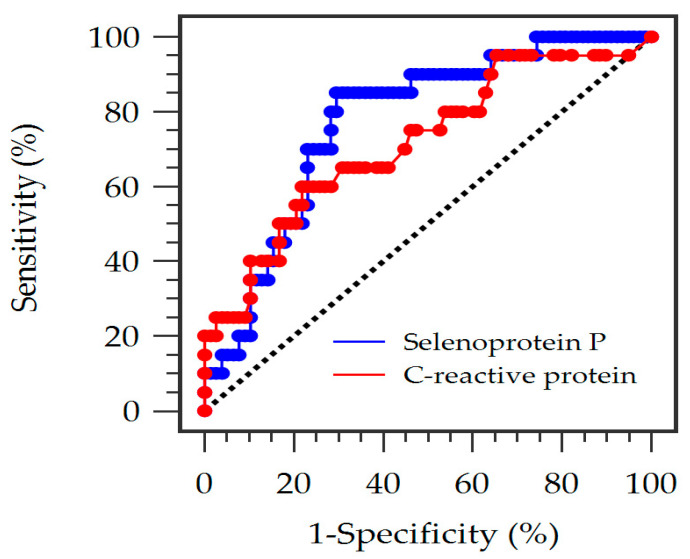 Figure 3
Figure 3- —Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Artery Disease Management · Dialysis and Renal Disease Management · Selenium in Biological Systems
1. Introduction
Peripheral arterial disease (PAD) represents a major clinical manifestation of systemic atherosclerosis and is disproportionately prevalent among individuals with chronic kidney disease (CKD) and end-stage kidney disease (ESKD). Epidemiologic evidence indicates that patients with advanced kidney dysfunction develop PAD at rates that far exceed those in the general population, with dialysis cohorts exhibiting a four- to sixfold higher prevalence and substantially increased risks of limb ischemia, amputation, and cardiovascular mortality [1]. Large-scale analyses of inpatients further demonstrated that those who had ESKD and PAD had relatively long admissions, high healthcare costs, and significantly elevated in-hospital mortality, underscoring the considerable clinical burden when these conditions coexist [2]. Although much of the existing literature focused on hemodialysis, patients undergoing peritoneal dialysis (PD) share a comparable risk profile, because several major PAD contributors, including diabetes, hypertension, dyslipidemia, chronic inflammation, oxidative stress, and CKD mineral bone disorder, are also prevalent in PD populations [3]. Additional PD-specific factors, such as hypoalbuminemia, protein loss, malnutrition, and persistent inflammation, may further exacerbate endothelial dysfunction, vascular calcification, and impaired microvascular integrity, thereby increasing susceptibility to lower extremity ischemia [4].
Given the often silent or atypical presentation of PAD in patients with CKD and on PD, timely recognition remains challenging. The ankle–brachial index (ABI) is a widely used, noninvasive, and inexpensive method for assessing lower limb perfusion, with demonstrated strong predictive value for cardiovascular events and mortality in both community and dialysis cohorts [5]. However, ABI reflects a hemodynamic surrogate rather than a definitive anatomic obstruction and does not fully capture clinically or imaging-confirmed PAD, particularly in patients with CKD and PD. Moreover, ABI interpretation in patients on dialysis requires caution, because medial arterial calcification and increased arterial stiffness, which are common in CKD, may lead to falsely elevated values and underdiagnosis of PAD [6]. Despite these limitations, a low ABI remains a robust indicator of PAD severity and portends worse survival among patients receiving long-term dialysis [7]. Consequently, PAD in patients on PD is frequently underrecognized but is clinically consequential, contributing to poor wound healing, infection, limb loss, and excess cardiovascular mortality.
Selenoprotein P (SePP) is the major selenium-transporting glycoprotein in circulation that plays a central role in systemic selenium homeostasis and antioxidant defense. SePP is predominantly synthesized in the liver and is responsible for delivering selenium to peripheral tissues. Impaired SePP production reduces selenium bioavailability, disrupts redox balance, and increases susceptibility to oxidative injury, all of which are closely linked with atherosclerotic vascular disease [8,9]. In addition to its transport function, SePP interacts with vascular endothelial proteoglycans through its heparin-binding domain, suggesting its localized role in modulating vascular redox activity [10]. Recent evidence has further identified SePP as a hepatokine capable of influencing metabolic signaling. In particular, elevated SePP was found to suppress adenosine monophosphate-activated protein kinase (AMPK) activation and promote insulin resistance, which are associated with endothelial dysfunction, inflammation, and accelerated vascular injury [11,12]. Moreover, genetic studies have demonstrated associations between SEPP1 variants, altered SePP isoform distribution, reduced selenium bioavailability, and the coexistence of PAD in patients with aortic disease [10]. Collectively, these findings support SePP as a biologically plausible and potentially relevant factor involved in vascular homeostasis and PAD susceptibility [13].
Despite these insights, the clinical significance of circulating SePP in PAD has not been established in PD populations. Existing research has largely examined selenium deficiency in CKD or explored the metabolic effects of SePP in nonuremic settings, and data on direct evaluation of SePP in relation to lower extremity arterial disease among patients on dialysis remain scarce. Moreover, it is unclear whether SePP level reflects vascular vulnerability beyond traditional cardiovascular and inherent PD-related risk factors, including chronic inflammation, oxidative stress, and protein loss. To address this gap, this study investigated the association between serum SePP concentrations and ABI-defined PAD in individuals undergoing maintenance PD. We further examined whether lower SePP levels are independently associated with ABI-defined PAD after adjustment for conventional cardiovascular and dialysis-specific risk factors.
2. Materials and Methods
2.1. Ethics and Study Participants
This cross-sectional study consecutively enrolled individuals who had been on PD for more than 6 months due to ESKD at Hualien Tzu Chi Hospital, Taiwan, from 1 February 2020, to 31 May 2020. The study protocol received approval from the Institutional Review Board of Hualien Tzu Chi Hospital (approval number: 108-219-A), and written informed consent was obtained from all participants. No compensation was provided. Patients were excluded if they had acute or active infections, decompensated heart failure, recent acute coronary syndrome or stroke, known malignancies, prior lower limb amputation, or an ABI > 1.3. Clinical parameters related to solute removal (i.e., weekly and peritoneal fractional clearance index for urea (Kt/V) and total and peritoneal creatinine clearance) were retrieved from electronic medical records. Diabetes mellitus (DM) was defined as a fasting plasma glucose level of ≥126 mg/dL or ongoing use of antidiabetic medications. Hypertension was defined as systolic blood pressure ≥140 mmHg, diastolic pressure ≥90 mmHg, or use of antihypertensive agents within 2 weeks prior to enrollment.
2.2. Anthropometric Measurements
All anthropometric assessments were conducted with the participants wearing light indoor clothing. Height and body weight were measured three times each, and the mean values were used in the analyses. Standing height was assessed using a stadiometer (H910; Nagata Scale Co., Tainan, Taiwan), and weight was determined using a calibrated digital scale (FM-200; Hostart Co., New Taipei City, Taiwan). Body mass index was calculated as weight divided by height squared (kg/m^2^).
2.3. Biochemical Analyses
Blood samples were collected after an overnight fast of at least 8 h and prior to the first daytime PD exchange. Venous blood (5 mL) was drawn into two tubes. An ethylenediaminetetraacetic acid (EDTA) containing tube was used for hemoglobin analysis using a hematology analyzer (Sysmex XS-1000i; Sysmex America, Mundelein, IL, USA). The remaining sample was centrifuged at 3000× g for 10 min, and serum was stored at 4 °C until testing. Serum biochemical parameters, including total cholesterol, triglycerides, glucose, albumin, blood urea nitrogen, creatinine, calcium, phosphorus, and C-reactive protein (CRP), were measured using an automated analyzer (Siemens Advia 1800; Siemens Healthcare, Erlangen, Germany). Enzyme-linked immunosorbent assays were used to determine concentrations of intact parathyroid hormone (iPTH) (NM59041, IBL International, Hamburg, Germany) and SePP (CSB-EL021018HU, Cosmo Bio USA, Carlsbad, CA, USA). The respective intra- and interassay coefficients of variation were 3.6% and 2.8% for iPTH and 3.2% and 5.4% for SePP.
2.4. Ankle-Brachial Index Assessment
ABI measurements were obtained using an automated oscillometric device (VaSera VS-1000; Fukuda Denshi, Tokyo, Japan). While supine, participants underwent three repeated measurements of systolic pressures on both brachial arteries and both ankles (dorsalis pedis and posterior tibial arteries). The ABI for each leg was calculated by dividing the highest ankle systolic pressure by the highest brachial systolic pressure. The average of three consecutive ABI measurements was used for analysis. Electrocardiographic monitoring was maintained for approximately 15 min during assessment. The device was calibrated in accordance with manufacturer recommendations, and all cuffs were certified and regularly inspected. PAD was defined as an ABI < 0.9 in either limb (ABI-defined PAD), which serves as a noninvasive surrogate marker of lower extremity arterial disease rather than a clinical or imaging-based diagnosis [14].
2.5. Statistical Analysis
The required sample size was estimated a priori, indicating that a minimum of 85 participants would be needed to achieve 80% statistical power (ɑ = 0.05) to detect a correlation coefficient of 0.30 between SePP levels and ABI values. Continuous variables were assessed for normality and presented as mean ± standard deviation or median with interquartile range, as appropriate. Group differences were evaluated using Student’s t-test or Mann–Whitney U test. Categorical variables were reported as counts with percentages and compared using chi-square analysis. Variables exhibiting skewed distributions, including PD vintage, fasting glucose, iPTH, CRP, and total creatinine clearance, were logarithmically transformed (log−) before correlation analyses and regression modeling. Multivariate logistic regression analysis was performed to identify factors associated with ABI-defined PAD, adjusting for the following clinical variables that exhibited significant differences between patients with and without ABI-defined PAD: PD vintage, age, CRP, fasting glucose, SePP, and diagnosis of DM. To further examine model stability, multivariate logistic regression was conducted with 1000 bootstrap resamples using bias-corrected and accelerated (BCa) confidence intervals. Model calibration was evaluated using the Hosmer–Lemeshow goodness-of-fit test, calibration intercept, calibration slope, and Brier score. A decision curve analysis was used to quantify the clinical utility of SePP-based prediction. Spearman’s rank correlation coefficients were calculated to explore associations among ABI values, SePP, and clinical parameters. To evaluate the diagnostic performance of serum SePP for ABI-defined PAD, receiver operating characteristic (ROC) curves were generated, and the area under the curve (AUC) was calculated (MedCalc Software Ltd., version 22.019, Ostend, Belgium). All analyses except ROC curves were performed using Statistical Package for the Social Sciences version 25.0 (IBM Corp., Armonk, NY, USA). Statistical significance was defined as p < 0.05.
3. Results
3.1. Baseline Characteristics
The clinical characteristics of the study population are summarized in Table 1. Of 98 patients on PD, 20 (20.4%) had ABI-defined PAD. Compared with patients with normal ABI group, those with low ABI group were significantly older (p = 0.014); had significantly longer PD vintage (p = 0.036); had similar body mass index, blood pressure, lipid parameters, hemoglobin, calcium, phosphorus, and dialysis adequacy metrics; had significantly higher levels of fasting glucose (p = 0.005) and CRP (p = 0.003); had significantly higher prevalence of DM (p = 0.033); and had significantly lower SePP levels (p < 0.001).
3.2. Factors Associated with Peripheral Artery Disease
Variables with p < 0.05 in the comparison of the normal and low ABI groups were included in a multivariate logistic regression model, with adjustments for age, DM, PD vintage, CRP, fasting glucose, and SePP. As shown in Table 2, multivariate logistic regression analysis revealed that ABI-defined PAD was independently associated with each 0.1 mg/dL increase in serum CRP [odds ratio (OR) 1.188, 95% confidence interval (CI) 1.062–1.329; p = 0.003] and serum SePP (OR 0.930, 95% CI 0.870–0.994; p = 0.032).
3.3. Bootstrap Internal Validation
Bootstrap internal validation (1000 iterations) further supported the robustness of these findings (Table 3). A low SePP level remained significantly associated with and continued to be a significant predictor of ABI-defined PAD (bootstrap B = −0.072; BCa 95% CI, −0.152 to −0.034).
Calibration analyses showed good model performance (Hosmer–Lemeshow χ^2^ = 5.429, p = 0.711). The calibration intercept was 0.000 (95% CI −0.428 to 0.428), and the calibration slope was 1.000 (95% CI 0.706–1.294), indicating excellent agreement between predicted and observed risk. The Brier score was 0.169, reflecting strong overall predictive accuracy (Figure 1).
3.4. Decision Curve Analysis
Decision curve analysis demonstrated that the SePP-based logistic model provided a clear clinical net benefit across a wide range of decision thresholds, compared with treat-all or treat-none strategies (Figure 2). Decision curve analysis results supported the potential clinical utility of the SePP-based logistic model for stratifying ABI-defined PAD risk.
3.5. Correlation Analysis
Spearman correlation analysis (Table 4) revealed moderate positive correlations between SePP level and ABI on the left (r = 0.336, p = 0.001) and right (r = 0.314, p = 0.002). ABI values were inversely correlated with age, log-PD vintage, log-glucose, and log-CRP (all p < 0.05). SePP was found to have negative correlations with log-glucose (r = −0.276, p = 0.006) and log-CRP (r = −0.234, p = 0.021), and a positive correlation with residual renal function (urine Clcr; r = 0.337, p = 0.014), but not with lipid parameters, blood pressure, or dialysis adequacy indices.
3.6. Receiver Operating Characteristic Curve Analysis
ROC curve analysis was performed to compare the diagnostic performance of SePP and CRP for ABI-defined PAD. The ROC analysis shows that serum SePP level has an AUC of 0.774 (95% CI: 0.669–0.880, p < 0.001), which is superior to CRP (AUC: 0.716; 95% CI: 0.583–0.850, p = 0.0015) in predicting ABI-defined PAD (Figure 3). The optimal cutoff value determined by the Youden index was <20.20 mg/L for SePP, yielding a sensitivity of 85.00% and a specificity of 70.51%. At this threshold, the positive predictive value was 42.50% and the negative predictive value was 94.83%. The optimal cutoff value determined by the Youden index was >0.62 mg/dL for CRP, yielding a sensitivity of 60.00%, a specificity of 78.21%, a positive predictive value of 41.49%, and a negative predictive value of 88.41%. SePP demonstrated a high AUC, suggesting its potential as a diagnostic marker in this population.
4. Discussion
In this exploratory cross-sectional study on patients undergoing maintenance PD, low serum SePP level was independently associated with ABI-defined PAD, even after adjustment for age, DM, PD vintage, fasting glucose, and CRP, and this relationship remained robust upon bootstrap internal validation and showed acceptable calibration. SePP correlated positively with both left and right ABI values and urine creatinine clearance and negatively with PD vintage, glycemic indices, and CRP, suggesting that reduced SePP may reflect cumulative vascular injury in this population. Our ROC curve analysis further supports the clinical utility of SePP, demonstrating a notable diagnostic performance for identifying ABI-defined PAD in patients on PD. In addition to SePP, several clinical factors were also associated with ABI-defined PAD, including older age, longer PD vintage, diabetes, elevated fasting glucose, and higher CRP levels, consistent with established mechanisms of vascular injury in CKD and dialysis populations [15,16,17,18,19,20]. These findings highlight the multifactorial nature of PAD in PD and the interplay among metabolic, inflammatory, and dialysis-related contributors.
As the major selenium transport protein, SePP plays an essential role in maintaining systemic antioxidant capacity [21,22]. Reduced SePP may exacerbate oxidative stress and endothelial dysfunction, thereby facilitating atherosclerotic vascular injury [23,24,25]. In patients undergoing PD, chronic inflammation, protein loss, and nutritional deficiencies may further reduce selenium reserves and impair SePP synthesis [26,27,28,29], providing a plausible biological explanation for the observed association between low SePP and ABI-defined PAD. The inverse associations we observed between SePP and CRP, as well as fasting glucose, together with its relation to longer PD vintage, suggest that circulating SePP reflects the cumulative metabolic–inflammatory and nutritional stress that characterizes long-term PD, including protein loss, malnutrition, and persistent low-grade inflammation. In this context, SePP appears to capture a cluster of vascular risk states, oxidative stress burden, chronic inflammation, and impaired nutritional status that are tightly linked to vascular dysfunction and PAD in PD populations. Our results support SePP as a biologically plausible proxy for vascular vulnerability, as it is associated with ABI-defined PAD in patients on PD.
Although previous studies have established the physiological importance of SePP in selenium transport and metabolic regulation [8,9,10,11,30,31], direct evidence linking SePP to PAD remains scarce, and no data specific to PD populations have been available. Given the limitations of ABI in dialysis populations [32], data on the association between circulating SePP and PAD in hemodialysis populations are currently lacking. Most studies in hemodialysis patients have focused on selenium status in relation to inflammation and cardiovascular risk rather than limb ischemia or PAD [33]. Therefore, whether similar associations exist in hemodialysis populations remains to be clarified in future studies. In our study, SePP was primarily evaluated as an associative marker of PAD-related pathophysiology rather than as a fully validated diagnostic test. The ROC-derived cut-off of <20.20 mg/L, with a sensitivity of 85.00% and an NPV of 94.83%, together with good calibration, internal bootstrap validation (1000 iterations), and favorable decision curve analysis, suggests that lower SePP levels are consistently associated with ABI-defined PAD and may have potential utility for ruling out PAD in this population. However, these performance estimates should be interpreted as exploratory and hypothesis-generating rather than as definitive evidence of diagnostic applicability.
This study had several limitations that should be acknowledged when interpreting the findings. First, the cross-sectional design precluded any causal inferences regarding the relationship between SePP levels and ABI-defined PAD; it cannot determine whether reduced SePP directly contributes to vascular pathology or represents a downstream marker of underlying metabolic and inflammatory disturbances. Second, the single-center design and relatively modest sample size of this study may limit the generalizability of our results to broader PD populations and reduce the power to detect more subtle associations. Third, PAD was not confirmed by advanced imaging modalities, such as duplex ultrasonography or computed tomography angiography, but was defined solely by ABI, which reflects a hemodynamic surrogate of lower extremity arterial disease rather than definitive anatomic obstruction. Although ABI is widely recommended for PAD screening, it may underestimate disease severity in patients with CKD and PD due to arterial stiffness and medial vascular calcification, potentially leading to false-negative results. Nevertheless, to minimize misclassification related to noncompressible arteries, patients with ABI > 1.3 were excluded from the present analysis. Fourth, circulating SePP was measured at a single time point, and dynamic changes in selenium status, dietary intake, protein losses, and inflammation over time were not assessed. Additionally, we did not measure other selenium-dependent enzymes or selenium intake, which may have influenced antioxidant capacity and vascular risk. Another limitation is that PD patients with PAD had higher daily peritoneal protein clearance than those without PAD [34]. We did not evaluate peritoneal protein or albumin losses concomitantly with SePP measurements; therefore, we cannot determine whether lower SePP levels simply mirror greater peritoneal protein loss and associated malnutrition, or whether SePP captures additional aspects of vascular and redox imbalance. Finally, although the analysis incorporated several multivariate models adjusting for significant factors, the influence of unmeasured residual confounding variables cannot be excluded. These limitations highlighted the need for larger-scale longitudinal studies to clarify temporal relationships and evaluate the predictive utility of SePP in clinical practice.
5. Conclusions
In summary, this study demonstrated that low circulating SePP concentrations were significantly and independently associated with ABI-defined PAD in patients undergoing PD. Given the high prevalence of subclinical PAD and limitations of ABI interpretation in this population, SePP should be interpreted primarily as an associative biomarker rather than as a validated diagnostic test for PAD. While ROC analysis and decision-curve metrics suggest that SePP may have potential for risk stratification, these findings are exploratory and derived from a single-center, cross-sectional cohort with limited sample size. Future longitudinal and interventional studies are warranted to clarify the temporal and mechanistic links among SePP deficiency, selenium homeostasis, and PAD and to determine the effect of correcting selenium or SePP levels on mitigating vascular risk in patients undergoing PD.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Huish S. Nawaz S. Bellasi A. Diaz-Tocados J.M. Haarhaus M. Sinha S. Clinical management of peripheral arterial disease in chronic kidney disease-A comprehensive review from the European Renal Association CKD-MBD Working Group Clin. Kidney J.202518 sfaf 0894059982110.1093/ckj/sfaf 089PMC 12209849 · doi ↗ · pubmed ↗
- 2De Stefano F. Rios L.H.P. Fiani B. Fareed J. Tafur A. National trends for peripheral artery disease and end stage renal disease from the National Inpatient Sample Database Clin. Appl. Thromb. Hemost.202127107602962110256253415160810.1177/10760296211025625 PMC 8221664 · doi ↗ · pubmed ↗
- 3Ho C.L.B. Chih H.J. Garimella P.S. Matsushita K. Jansen S. Reid C.M. Prevalence and risk factors of peripheral artery disease in a population with chronic kidney disease in Australia: A systematic review and meta-analysis Nephrology 20212679880810.1111/nep.1391434156137 · doi ↗ · pubmed ↗
- 4De Loach S.S. Mohler E.R.3rd Peripheral arterial disease: A guide for nephrologists Clin. J. Am. Soc. Nephrol.200728398461769950110.2215/CJN.04101206 · doi ↗ · pubmed ↗
- 5Newman A.B. Shemanski L. Manolio T.A. Cushman M. Mittelmark M. Polak J.F. Powe N.R. Siscovick D. Ankle-arm index as a predictor of cardiovascular disease and mortality in the Cardiovascular Health Study. The Cardiovascular Health Study Group Arterioscler. Thromb. Vasc. Biol.19991953854510.1161/01.ATV.19.3.53810073955 · doi ↗ · pubmed ↗
- 6Aboyans V. Criqui M.H. Abraham P. Allison M.A. Creager M.A. Diehm C. Fowkes F.G. Hiatt W.R. Jönsson B. Lacroix P. Measurement and interpretation of the ankle-brachial index: A scientific statement from the American Heart Association Circulation 2012126289029092315955310.1161/CIR.0b 013e 318276 fbcb · doi ↗ · pubmed ↗
- 7Miguel J.B. Matos J.P.S. Lugon J.R. Ankle-brachial index as a predictor of mortality in hemodialysis: A 5-year cohort study Arq. Bras. Cardiol.201710820421110.5935/abc.2017002628443959 PMC 5389869 · doi ↗ · pubmed ↗
- 8Burk R.F. Hill K.E. Selenoprotein P: An extracellular protein with unique physical characteristics and a role in selenium homeostasis Annu. Rev. Nutr.20052521523510.1146/annurev.nutr.24.012003.13212016011466 · doi ↗ · pubmed ↗