Psychosocial Aspects of Cystic Fibrosis: A Mixed-Methods Systematic Review
Maria Inês Griff, Rita Santos, Carmen Trumello, Tânia Brandão

TL;DR
This review shows that as people with cystic fibrosis live longer, their mental health and social challenges become increasingly important and need better support.
Contribution
The study updates the understanding of psychosocial challenges in adults with cystic fibrosis and emphasizes the need for integrated care models.
Findings
Optimistic coping is the most frequent strategy linked to improved survival in CF patients.
High social support and gratitude are key factors for treatment adherence and quality of life.
Depression is the primary mental health concern, and financial stress and stigma are major psychosocial challenges.
Abstract
What are the main findings? Psychosocial aspects (e.g., coping, social support) were identified as central to the CF patient experience, shifting the focus beyond biological survival.Advances in treatment have significantly increased life expectancy, introducing new psychosocial challenges for adults with CF (e.g., management of visible symptoms, stigma in the workplace, financial instability). Psychosocial aspects (e.g., coping, social support) were identified as central to the CF patient experience, shifting the focus beyond biological survival. Advances in treatment have significantly increased life expectancy, introducing new psychosocial challenges for adults with CF (e.g., management of visible symptoms, stigma in the workplace, financial instability). What are the implications of the main findings? There is a need for integrated care models that address both clinical symptoms…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
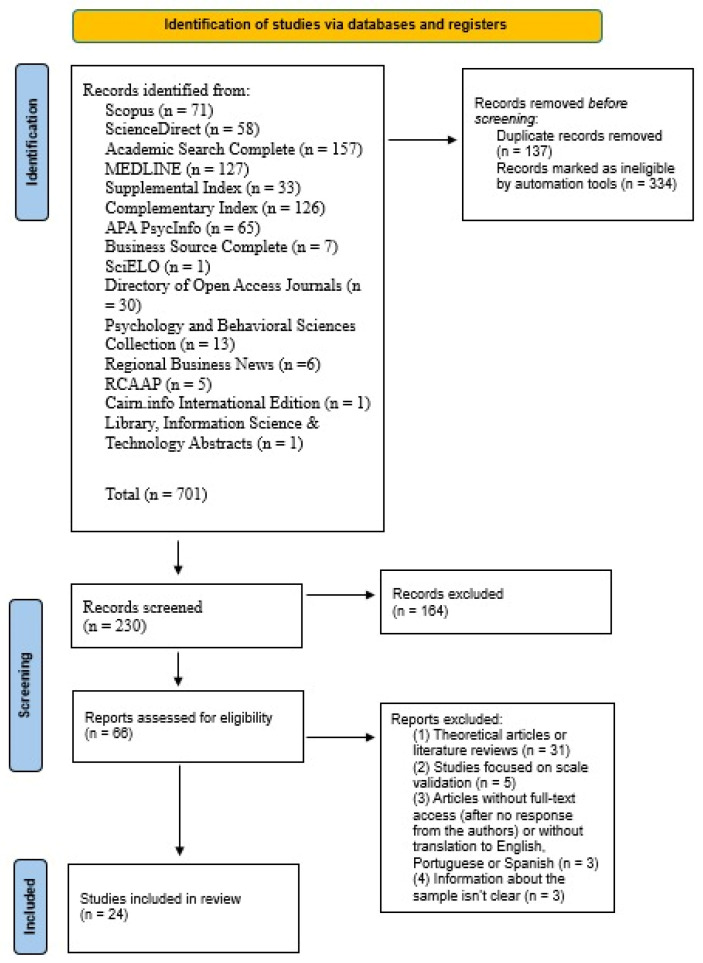 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCystic Fibrosis Research Advances · Adolescent and Pediatric Healthcare · Dialysis and Renal Disease Management
1. Introduction
Cystic fibrosis (CF) is a genetic, autosomal recessive disorder characterized by reduced or absent CFTR protein function [1]. This protein deficiency results in the accumulation of mucus in various organs, including the lungs, liver, pancreas, and gastrointestinal tract [1]. Consequently, the most prominent clinical manifestations of CF include chronic pulmonary infections, leading to bronchiectasis and progressive lung failure, chronic hepatobiliary disease, exocrine pancreatic insufficiency, intestinal obstruction, and male infertility [2]. As the disease progresses, individuals may also experience shortness of breath, exercise intolerance, chronic sinusitis, nasal polyps [3], and the potential development of diabetes [4]. CF primarily affects the Caucasian population, with a global prevalence of approximately 80,000 individuals [5]. However, between 2008 and 2021, only about 50,000 patients were registered in the European Cystic Fibrosis Society Database [6].
Contrary to what occurred when CF was first described in 1938, individuals with CF have seen their life expectancy increase significantly due to the progressive understanding of the disease and, consequently, the development of more effective treatments [2]. These treatments include the use of antibiotics to manage pulmonary infections, dietary modifications aimed at increasing caloric and fat intake, the use of pancreatic enzymes, anti-pseudomonas therapies, mucolytics, prenatal screening for early identification and intervention, and, most recently, treatment with CFTR modulators [7]. Additionally, lung transplantation has emerged as an option for extending life in patients who are considered suitable candidates [8]. However, complications from lung transplants have become the second leading cause of death in patients with CF [9]. As a consequence of these treatments, the financial costs associated with this disease both for patients and their families, health care providers, and society are substantial [10].
Due to ongoing therapeutic advancements, there is continued optimism regarding the improvement of life expectancy [4]. As reported by Turcios [3], life expectancy has seen significant increases, rising from 41.2 years in 2015 to 47.7 years by 2016. Considering the projected 70% increase in the adult CF population between 2010 and 2025 [11], it is crucial to advance not only clinical care but also psychological support [4].
When diagnosed with multiple comorbidities that require costly and complex treatments and are associated with reduced survival rates, it is understandable that both patients and their families may experience negative reactions [12]. This is particularly evident in the case of CF, a genetic condition that shapes an individual’s life, bringing not only physical challenges but also psychological burdens [12].
Living with CF can trigger challenging emotions related to uncertainty, loss of identity, and the potential loss of social support networks, including long-standing family and friends [12]. Additionally, as CF is a chronic and debilitating disease, conditions like anxiety and depression—which have been linked to more frequent hospitalizations compared to patients without these conditions [13]—can severely impact patients’ quality of life [14]. These mental health challenges can foster less optimistic beliefs about the effectiveness of medications, consequently affecting treatment adherence [13]. Poor adherence, in turn, has been associated with higher healthcare costs [10], higher rates of depression [14], and more frequent episodes of exacerbation and hospitalizations [13].
Moreover, given that CF involves a wide range of daily treatments that may need to be carried out in public spaces (e.g., taking medications), often in front of people unaware of the condition, individuals with CF may experience a fear of stigmatization [13]. This fear has been associated with reduced pulmonary function, as well as more severe symptoms of depression and anxiety, lower levels of optimism, and a poorer health-related quality of life [13]. Additionally, frequent coughing, a common symptom of CF, can have negative social consequences, such as physical distancing by those who may perceive the coughing as a symptom of a contagious illness (e.g., a cold) [15].
The importance of research involving individuals with CF is underscored by the complexity of the condition, which presents both psychological and physical challenges, as well as the progressive increase in life expectancy associated with the disease [3]. This highlights the growing need to better understand the psychological challenges related to adapting to CF [16]. However, current research remains limited. While previous reviews exist, they are either outdated [17,18,19], focus solely on depression and anxiety [14], or concentrate only on factors that promote resilience [16].
Accordingly, this systematic review synthesized and analyzed the psychosocial factors associated with adults (≥18 years) living with CF, guided by the research question: “What psychosocial aspects of CF are documented in the current literature?” By identifying the most prominent psychosocial factors, this review provides a comprehensive update of existing evidence, characterizes current research gaps, and offers clinical insights to enhance psychological support and future investigations.
2. Materials and Methods
This mixed-methods systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [20] to ensure a structured and transparent approach in identifying, reviewing, and including articles for the present analysis. A review protocol was retrospectively registered into the Open Science Framework (OSF) database (registry number: 10.17605/OSF.IO/HFKVB).
2.1. Eligibility Criteria
The following inclusion criteria were established for this mixed-methods systematic review: (1) quantitative, qualitative, or mixed-method studies that evaluate any type of psychosocial aspects associated with living with CF in adults (except anxiety and depression, examined in [14]; if studies included anxiety and depression as part of a broader psychosocial or health-related context, those studies were included); (2) peer-reviewed articles; (3) articles written in English, Portuguese, or Spanish; and (4) articles published in the last 10 years. Exclusion criteria were (1) theoretical articles or literature reviews; (2) studies focused on scale validation; and (3) articles without full-text access (after no response from the authors) or that did not provide a translation to English, Portuguese, or Spanish.
2.2. Search Strategy and Study Selection
The literature search for this mixed-methods systematic review was conducted in November 2024 for different databases including Scopus, ScienceDirect, Academic Search Complete, MEDLINE, Supplemental Index, Complementary Index, APA PsycInfo, SciELO, Directory of Open Access Journals via EBSCO—Research Databases, EBooks, and Discovery Service.
The search terms used were cystic fibrosis (TI) AND social support or coping or resilience or psychological distress or mental health or emotional distress or emotion or life satisfaction or psychosocial adaptation or psychological adaptation or psychological needs or psychological well-being or stigma (all fields). To exclude studies only focused on anxiety, depression, children, adolescents, caregivers, or the focus on lung transplantation, additional terms were applied: NOT depression or anxiety NOT children or adolescents or youth or child or teenager or pediatric or caregivers or transplantation (see Supplementary Materials).
This initial search yielded a total of 701 articles. After the automatic removal of 137 duplicate articles and the application of database-built filtering options, 334 articles were excluded. These exclusions were based on the following criteria: the search was limited to peer-reviewed articles in English, Portuguese, and Spanish, and to studies published within the last 10 years. These filters were automatically applied using the built-in features of the databases, ensuring that the retrieved articles met the language, publication, and peer-review criteria.
Thus, a final total of 230 articles remained for further analysis. The 230 articles were screened based on their titles and abstracts, considering both the inclusion and exclusion criteria. Following this step, 66 articles remained for full-text review. During this stage, articles that did not meet the predefined inclusion criteria were excluded, resulting in the removal of 42 articles. Therefore, a total of 24 scientific articles were included in this mixed-methods systematic review (Figure 1). This was performed and independently reviewed by two researchers.
3. Results
The results of this mixed-methods systematic review are presented below. First, an overview of the general characteristics of the included studies is presented, including information on the authors, country, demographic characteristics of the participants, study design, types of measures used (to indicate the source of validity for each tool), and the objective of each study. Then, the data analyses and the key findings from each study are described.
3.1. General Description of the Articles
Table 1 presents the 24 articles included in this mixed-methods systematic review, published between 2015 and 2024. Most of the studies were conducted in the United Kingdom (n = 9) [21,22,23,24,25,26,27,28,29] and the United States of America (n = 8) [30,31,32,33,34,35,36,37]. Two studies were from Brazil [38,39], one study was from Sweden [40], one was from Australia [41], one was from Greece [42], one was from Canada [43], and one was from Israel [44].
In terms of participant characteristics, sample size ranged from a minimum of 12 participants in a cross-sectional qualitative study [39] to a maximum of 250 participants in a longitudinal quantitative study [32], yielding a total of 2023 participants across all 24 studies. Data were collected from both male and female participants in all studies, although Aguiar et al. [38] did not provide specific information regarding the sex or the age of the participants (n = 52). For the remaining 1971 participants, where sex information was available, 843 were male (42.77%) and 1128 were female (57.23%). Although there were more female participants in total, the male participants were predominant in 13 of the 24 studies included. The study of Williaws et al. [29], due to his aim, only had female participants (n = 182). The average age of the participants was 31.2 and the age range varied from a minimum of 20.7 years [23] to a maximum of 70 years [24].
Regarding the study designs of the 24 included articles, nine employed a cross-sectional quantitative design, seven used a cross-sectional qualitative design, four employed a longitudinal quantitative design, three utilized a mixed-methods cross-sectional design, and one used a mixed-methods longitudinal design. In the cross-sectional quantitative studies (n = 9) and in the longitudinal quantitative studies (n = 5), self-report scales were administered to participants. The cross-sectional qualitative studies (n = 7) used a semi-structured interview developed by the authors to address the study’s objectives. The mixed-methods cross-sectional studies (n = 3) employed both self-report scales for participants and a structured interview [23] or a semi-structured interview [28,29] to assess participants’ psychosocial functioning.
Although all the articles aimed to identify the psychosocial aspects associated with CF, they focused on different topics. These included the use of mindfulness and self-compassion [25], coping strategies [21,23,27], or hygge practices [35] to deal with the disease. Additionally, the experience of dealing with CF and overall psychological well-being [24,32,38,39,40], possible health risk behaviors [26], and treatment adherence [22,36] were also some of the themes explored. More specifically, themes like adverse childhood experiences [28], existential distress [37], and social isolation [34] within this population were studied.
In addition, there were themes like self-disclosure of the diagnosis to family, friends, romantic partners, and co-workers [30,31,44], shared decision-making of reproductive goals [29], and social support [33]. Finally, there were some studies concerning social issues, like the access to psychological services [43], financial costs related to the maintenance of the disease [42], and the use of telehealth [41].
3.2. Main Results
Table 2 presents the data analysis methods used in the 24 articles included in this mixed-methods systematic review. The seven qualitative studies [22,25,26,31,35,39,44] employed thematic coding to analyze the collected data. In contrast, the 14 quantitative studies utilized various statistical tests, including descriptive analyses to characterize the sample, Spearman correlations [30,34,38,42], Pearson correlations [37,42], bivariate correlations [24,32,33], T-tests [21,30,36,41,42], Bonferroni post hoc corrections [24,30], and Holm’s sequential Bonferroni procedure [43]. Additionally, multiple linear regression [33,36,42], multivariate regression [27,37], linear regression [17,32], logistic regression [36], Mann–Whitney [34,38], Wilcoxon [37,41], Fisher exact test [21,43], Kruskal–Wallis [34], structural equation modelling [40], Cox’s proportional hazards model [21], McNemar test and linear mixed effects models [41], and, at last, Kolmogorov-Sminorv and Anova [42] were used.
In the mixed-methods studies, one of them used thematic coding and descriptive analyses [23], one used only Pearson correlations and did not provide information on how they coded the semi-structured interview [28], and the last one used descriptive analysis and multivariable linear regression models to analyze the quantitative data, while thematic analysis using the COM-B model was used to treat the semi-structured interview [29].
4. Discussion
The main objective of this mixed-methods systematic review was to organize and analyze the literature on the psychosocial aspects associated with the experiences of patients over 18 years old with CF. This review aimed to contribute to the understanding of the psychological component of CF and to advance research on the involved psychosocial aspects. This need arises from the genetic and clinical advancements in treating CF, which have led to an increased life expectancy for this population [4], consequently introducing new challenges in adulthood.
Firstly, it is important to note that the number of studies (n = 24) published between 2015 and 2024 that were included in this mixed-methods systematic review marks a powerful statement regarding the importance that is now being given to the psychosocial experiences of adults with CF, a population whose life expectancy has increased in recent years [7]. This robust number contradicts the historical notion that psychological knowledge in CF is sparse, confirming that the field has shifted its focus beyond purely physical and biological concerns.
At least one psychosocial aspect associated with the experience of living with CF was identified in all 24 studies, with coping mechanisms [21,23,27,39], quality and nature of social support [26,29,30,31,32,33], and the challenges that affect the quality of life of patients [24,34,35,38,42,43] appearing as particularly dominant. Among the other mentioned psychosocial factors are the effects of physical activity towards psychological well-being [40], the experiences of telehealth [41], the challenges of entering adulthood, particularly in relation to financial matters [25], a lack of access to effective mindfulness practices tailored for CF patients [25], difficulty in implementing self-compassion [25], and challenges in connecting mind and body [25]. Furthermore, the effects of child maltreatment and household dysfunction [28], the adherence of treatment [22,23,36], the effects of symptom burden [37], and the disclosure styles and their psychosocial implications [44] were also highlighted.
Regarding the individual psychological experience, coping mechanisms appeared as a dominant theme. Optimist coping was the most used strategy [23,39] and the only coping measure that showed a beneficial effect on survival, especially in women [21], whilst active coping was positively associated with social quality of life [27]. Interestingly, the practice of hygge, a concept centered on consciously creating coziness, comfort, and connection, appeared as a valuable strategy for promoting wellness. This practice enhanced resilience and overall quality of life, allowing patients with CF to re-establish a degree of perceived control over their health condition [35].
However, the review also highlighted challenges in adjustment. While overall levels of psychological distress (anxiety and depression) were reported as low [23], depression emerged as predominant, with patients reporting they would use psychological services if available [43]. Importantly, psychological distress appears to stem less from general adverse childhood experiences and more from illness-related trauma, which was highly prevalent [28]. Specifically, distress related to painful procedures and forced treatments during childhood emerged as a more significant burden than typical household dysfunction [28]. Furthermore, although patients recognize the protective value of self-compassion for quality of life [24] and sexual satisfaction [38], they reported significant barriers in its practical application and a perceived lack of access to relevant therapeutic tools like mindfulness [25].
This complexity in adjustment is also visible in health risk behaviors. Patients reported engaging in behaviors such as smoking and drinking, which resulted from complex interactions between identity, social support, and attitudes towards CF [26]. Notably, there was a reported lack of knowledge on the consequences of these behaviors, with many patients declaring not being informed of these by clinicians [26].
The psychological dimension deeply influences treatment adherence; while participants in general felt that their levels of adherence were reasonably high [23], the ones with a higher baseline gratitude were significantly more likely to demonstrate persistent adherence [36]. Actually, poor adherence appeared to be often rooted in opportunity and capability barriers rather than purely psychological resistance; individuals with very low adherence frequently cited logistical factors (e.g., lack of time, privacy, or financial resources) as the primary challenge [22]. Conversely, social influences—specifically the comfort and willingness to perform treatments openly—act as a strong enabler for high adherence [22]. Self-efficacy regarding medication adherence was also shown to be positively correlated with undergoing treatments in front of loved ones [30].
Regarding the physical outcomes, the use of medication ensured better physical health [42], whilst a better physical condition resulted in better sexual activity [38]. These findings regarding the connection between physical action and well-being were in contrast to the ones from Bäckström-Eriksson et al. [40], where the authors noted that there seems to be no advantage in performing physical exercise concerning psychological well-being if not accompanied by a positive effect on medical status.
Navigating the social world remains a central challenge. While CF had no reported negative effect on friendships, being admitted to the hospital and managing treatments impacted work or studies [23], whilst support from loved ones and the professional team represented a crucial buffer against these difficulties [39]. Women reported more social support than men, and being employed was also associated with greater perceptions of support [33]. Greater social support was associated with less treatment burden and a better overall perception of health [32]. However, subjective social isolation—the feeling of loneliness—significantly predicted poorer quality-of-life outcomes, particularly among unmarried individuals, suggesting that the perception of loneliness leads to behavioral withdrawal [34].
A key component of social interaction is disclosure. Many patients used more than one disclosure strategy during their lifetime, depending on life transitions like marriage, having children, or disease worsening [44], while participants typically adopted the disclosure method of their parents. Nonetheless, selective disclosure was predominantly used to reduce negative consequences like pity, insults, or discrimination [44]. While patients experienced a greater comfort sharing their diagnosis with loved ones [30], shame and embarrassment due to symptoms like coughing may still lead to difficulties in maintaining romantic relationships [39].
Finally, this review highlights systemic gaps. The findings indicate that the unexpectedly prolonged life trajectory leaves CF adults unprepared for key life transitions, with financial issues being a major concern [25]. Patients reported unmet needs predominantly in the physical, daily living, and psychological domains, with concerns such as fatigue and fears about disease progression being highly prevalent [37]. Furthermore, while participants expressed a high motivation to engage in shared decision-making (SDM), their capacity was compromised by structural barriers, specifically insufficient information about reproductive goals (e.g., pre-pregnancy preparations), indicating that healthcare teams must proactively address these gaps [29]. On a positive note, telehealth delivery offered a comparable quality of care to in-person visits, while reducing costs and improving emotional functioning [41,42].
All of these interconnected psychosocial aspects and their consequences on the mental and physical health of individuals with CF highlight the importance of interventions that address both clinical and psychosocial aspects—from those most studied in this population (e.g., anxiety and depression) to those less explored (e.g., stigma, self-esteem, symptom burden).
In conclusion, this mixed-methods systematic review has fulfilled its objective: to organize and analyze the psychosocial aspects associated with living with CF in individuals over 18 years old. In doing so, it has contributed to the current understanding of what is known and the path that remains in terms of the psychosocial aspects impacting the lives of adult CF patients.
4.1. Limitations
Although this mixed-methods systematic review identifies and updates information on the psychosocial aspects that may be involved in the experience of living with CF and provides useful insights into the gaps in this area of study, several limitations must be acknowledged.
A limitation of this review is the absence of formal inter-rater reliability testing (e.g., kappa analysis) during the full-text screening and data extraction process. While discrepancies between reviewers were resolved through discussion and mutual agreement, the lack of formal reliability measures may limit the reproducibility and consistency of the screening process.
Also, 17 of the 24 studies were conducted predominantly in the same countries—nine in the United Kingdom and eight in the United States of America—with the remaining seven being conducted in Brazil (n = 2), Sweden (n = 1), Australia (n = 1), Greece (n = 1), Canada (n = 1), and Israel (n = 1). Therefore, most of the studies (n = 20) originate from only two continents, Europe and North America, specifically in the Northern Hemisphere. This limitation may introduce a cultural bias in the results and interpretations of this review. While this may be partially explained by the prevalence of the disease in the Caucasian population [5] and the lack of recent implementation of neonatal screening for CF diagnosis in some of the excluded continents, it limits this mixed-methods systematic review in addressing the psychosocial aspects of living with CF in non-Western cultures. Furthermore, according to the latest record from the Cystic Fibrosis Foundation, which collects data solely in the United States, more than 17% of the 33.288 patients registered in the database are not of Caucasian descent, demonstrating that the CF population has diversified in recent years [9].
The use of a variety of different scales to assess similar psychosocial constructs (e.g., quality of life, anxiety, or coping) limits the ability to directly compare results or conduct a quantitative synthesis of the findings.
To conclude, the timeframe of the 24 articles included in this mixed-methods systematic review coincides with the widespread introduction of highly effective modulator therapies (e.g., CFTR modulators). The reviewed studies did not consistently control for or distinguish between patients receiving these transformative therapies and those who were not; as for this, the psychosocial experiences reported in earlier studies may differ significantly from the current reality of patients benefiting from these new treatments, potentially affecting the generalizability of the findings to the current clinical landscape.
4.2. Future Research and Clinical Implications
Based on the results of this mixed-methods systematic review, all studies (n = 24) identified at least one psychosocial aspect that impacts the life of an adult with CF. While the findings of this review confirm a positive shift beyond purely physical concerns, the study of psychosocial adaptation in adulthood is still a relatively recent and evolving field. This timeline mirrors the medical history of the disease: for decades, the urgent scientific priority was aimed at genetic and biological advancements to reduce early mortality [4], given that widespread survival into adulthood only became a reality after the 1980s [7].
CF affects approximately 80,000 people worldwide [5]. With increasing life expectancy, particularly due to advances in treatments with CFTR modulators [7], individuals with this disease are experiencing new phases of adulthood (e.g., entering the workforce and starting families). In fact, the life expectancy for babies born with CF between 2019 and 2023 is now 61 years, compared to 45 years for those born between 2014 and 2018 and 33 years for those born between 1999 and 2003 [9]. This data shows that adults aged 21 to 25, born between 1999 and 2003, are now entering adulthood, which presents an opportunity to address the gaps in research on CF and psychosocial aspects in adult life with a significant sample. Therefore, investigating this topic and its implications for older ages, with accompanying clinical progress and emerging psychosocial needs, becomes increasingly relevant.
The implications should not remain limited to research, as this work could enable healthcare teams involved in the treatment and management of CF (e.g., doctors, physiotherapists, nurses, psychologists) to better understand the daily challenges faced by adult CF patients. This, in turn, could lead to the adjustment of techniques and more effective support. The need for more studies on the psychosocial impact in this population is closely linked to the need to develop effective intervention programs to improve adaptation to the disease, particularly as it relates to adulthood, given the physical limitations this disease entails.
In this context, recognizing that CF is a rare lifelong disease, group intervention programs—considering healthcare guidelines to maintain necessary distance (e.g., online group interventions) and avoid cross-contamination [13]—could prove valuable. These groups foster therapeutic factors that contribute to patient change, such as instilling hope, promoting universality, and sharing information [75]. Through such interventions, CF patients could find a safe and supportive environment to share their difficulties, fears, and concerns.
Additionally, since CF is a progressive disease, although individuals are born with it and do not experience an initial adjustment to the condition, they must adapt to their deteriorating health over the years and the possibility of early mortality. Interestingly, anxiety related to death was not explored in this mixed-methods systematic review, highlighting a significant gap in research on this population. Given the progressive nature of the disease and the reality of early mortality, further research in these areas is essential to help healthcare professionals provide effective intervention, particularly in guiding patients through adulthood and preparing for potential early death.
5. Conclusions
This mixed-methods systematic review synthesized and analyzed the psychosocial dimensions of living with CF in adults. The findings underscore the critical importance of addressing the psychological burden alongside physical symptoms, especially as life expectancy increases due to therapeutic advancements. Key psychosocial factors—including coping strategies, social support, stigma, and mental health—were found to profoundly influence quality of life and treatment adherence in adults with CF. Furthermore, this review identifies a significant disparity in psychological support, particularly in non-Western contexts, highlighting the urgent need for integrated healthcare models that bridge clinical and psychosocial interventions. By providing a holistic understanding of the multifaceted experiences of individuals with CF, this study offers clear directions for future research and clinical practices dedicated to enhancing person-centered care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ong T. Ramsey B.W. Cystic Fibrosis: A Review JAMA 2023329185910.1001/jama.2023.812037278811 · doi ↗ · pubmed ↗
- 2De Boeck K. Cystic fibrosis in the year 2020: A disease with a new face Acta Paediatr.202010989389910.1111/apa.1515531899933 · doi ↗ · pubmed ↗
- 3Turcios N.L. Cystic Fibrosis Lung Disease: An Overview Respir. Care 20206523325110.4187/respcare.0669731772069 · doi ↗ · pubmed ↗
- 4Singh J. Towns S. Jayasuriya G. Hunt S. Simonds S. Boyton C. Middleton A. Kench A. Pandit C. Keatley L.R. Transition to adult care in cystic fibrosis: The challenges and the structure Paediatr. Respir. Rev.202241232910.1016/j.prrv.2020.07.00932917516 · doi ↗ · pubmed ↗
- 5Taylor-Cousar J.L. CFTR Modulators: Impact on Fertility, Pregnancy, and Lactation in Women with Cystic Fibrosis J. Clin. Med.20209270610.3390/jcm 909270632825766 PMC 7563981 · doi ↗ · pubmed ↗
- 6European Cystic Fibrosis Society Patient Registry 2020 Available online: https://www.ecfs.eu/ecfspr(accessed on 1 September 2025)
- 7Mason K.A. Rogol A.D. Trends in Growth and Maturation in Children with Cystic Fibrosis Throughout Nine Decades Front. Endocrinol.20221393535410.3389/fendo.2022.935354 PMC 931772435903281 · doi ↗ · pubmed ↗
- 8Ramos K.J. Quon B.S. Heltshe S.L. Mayer-Hamblett N. Lease E.D. Aitken M.L. Weiss N.S. Goss C.H. Heterogeneity in Survival in Adult Patients with Cystic Fibrosis with FEV 1 < 30% of Predicted in the United States Chest 20171511320132810.1016/j.chest.2017.01.01928115168 PMC 5472512 · doi ↗ · pubmed ↗