Analysis of the Multifactorial Risks of Postpartum Urinary Incontinence: A Systematic Review
Nikoleta Tsinisizeli, Anastasia Bothou, Kleanthi Gourounti, Anna Deltsidou, Aikaterini Lykeridou, Giannoula Kyrkou

TL;DR
This review summarizes risk factors for postpartum urinary incontinence, highlighting delivery type, obesity, and pregnancy history.
Contribution
The study systematically identifies contemporary risk factors for postpartum urinary incontinence using recent data and highlights gaps in assessment methods.
Findings
Vaginal/instrumental delivery, obesity, maternal age, and neonate's birth weight are key risk factors for postpartum UI.
Multiparity and pre-pregnancy incontinence symptoms are strong predictors of postpartum urinary incontinence.
Heterogeneity in study methods and assessment timing limits the comparability of findings across studies.
Abstract
Introduction: Urinary incontinence (UI) is one of the most common pelvic floor disorders after childbirth and depends on hormonal changes, anatomical damage that occurs after childbirth, muscle and connective tissue weakness, fascia and nerves. UI is distinguished into three subtypes, including stress urinary incontinence (SUI), urgent urinary incontinence (UUI) and mixed urinary incontinence (MUI). Aim: The purpose of this review is to collect and summarize the results of studies related to the risk factors of urinary incontinence, to disseminate this information to scientists so that this major issue can be prevented, identified and managed. Methodology: This review followed the methodology of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and PECO eligibility criteria were used. We included studies published up to 2025 and not before 2019. The review was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
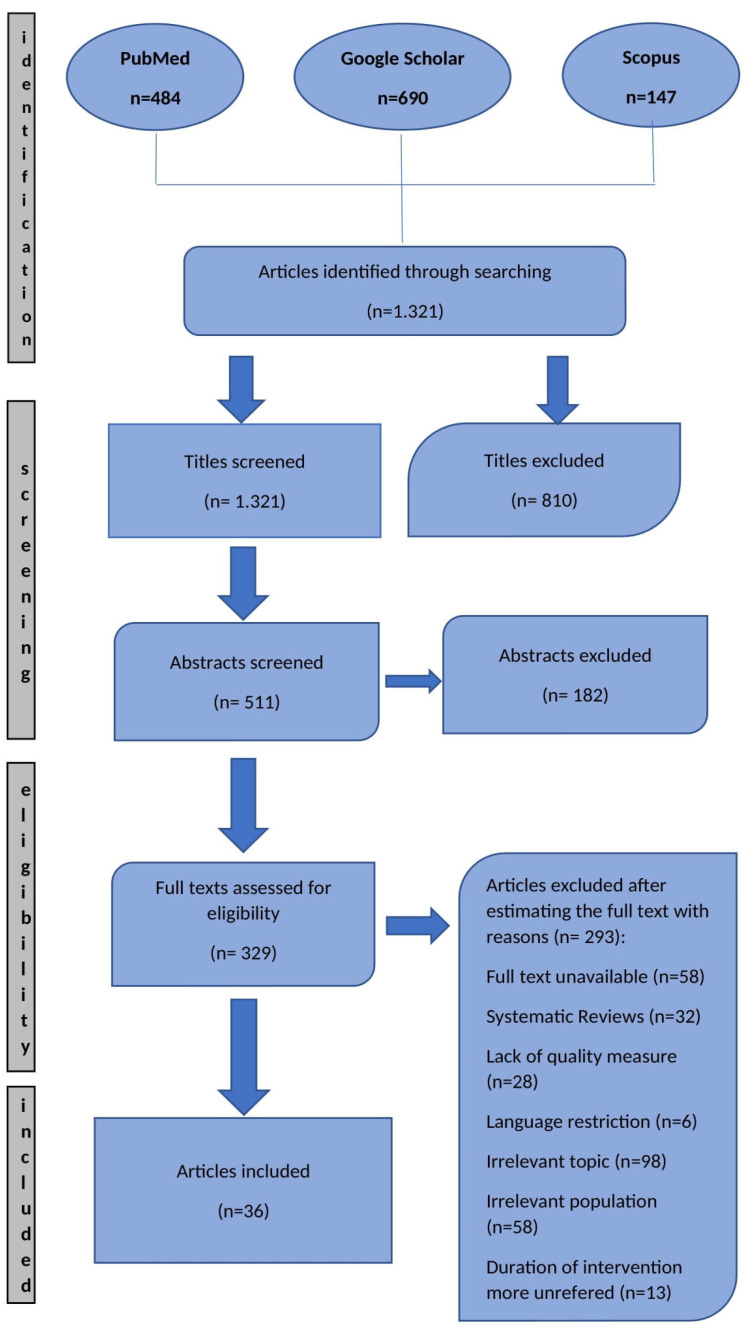 Figure 1
Figure 1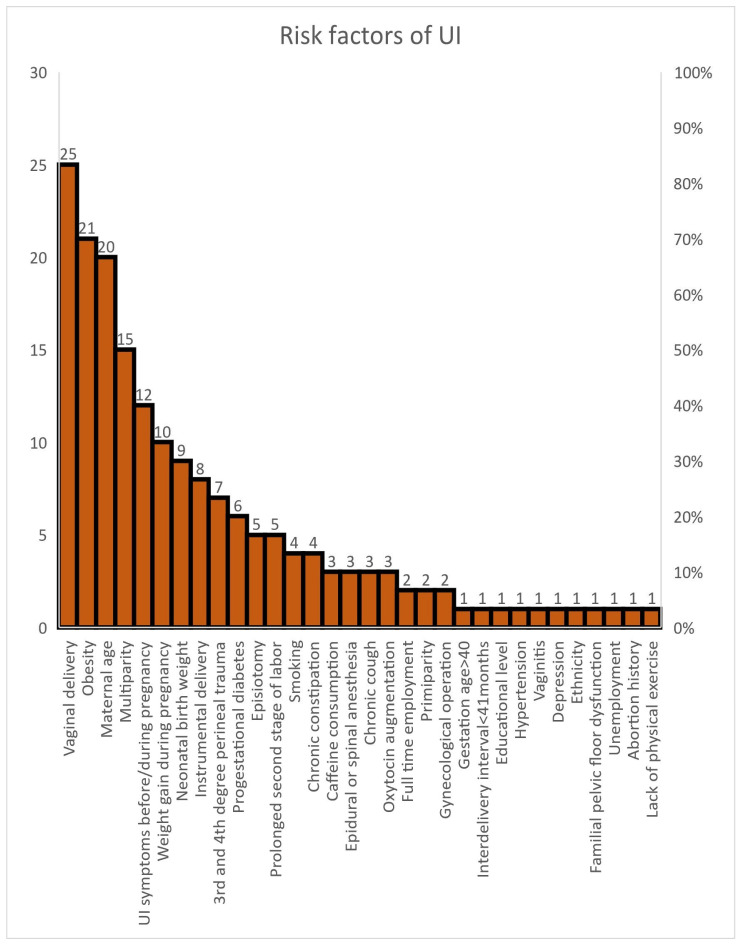 Figure 2
Figure 2- —University of West Attica
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPelvic floor disorders treatments · Pressure Ulcer Prevention and Management · Urinary Tract Infections Management
1. Introduction
Urinary incontinence is a multifactorial health problem. In addition to pelvic organ prolapse and fecal incontinence, urinary incontinence is one of the most common pelvic floor disorders after childbirth and depends on hormonal changes, anatomical damage that occurs after birth, muscle and connective tissue weakness, fascia and nerves [1,2]. Urinary incontinence may be the result of bladder or sphincter dysfunction or both [3]. Hormonal changes during pregnancy, accompanied by weakened bladder neck support, contribute to a change in the pelvic floor support structure [4]. During that period, reduced muscle strength of the pelvic floor muscles, abnormal contractility of the urethra and relaxation of the pelvic ligaments are observed. Urinary incontinence (UI), according to the International Urinary Incontinence Society (ICS), is any involuntary loss of urine, and its severity is determined by frequency and type of leakage, confounding factors, impact on hygiene, social impact and impact on the woman’s quality of life with or without health care seeking.
Several guidelines argue that symptom reporting and self-assessment by women themselves can accurately reflect the severity of urinary incontinence symptoms without requiring measurement of the weight of the incontinence pads [5]. Some women perceive urinary incontinence as an expected symptom of childbearing, while for other women it is a social stigma. UI is distinguished into three subtypes, including stress urinary incontinence (SUI), urgent urinary incontinence (UUI) and mixed urinary incontinence (MUI) [6].
SUI is the main type of urinary incontinence, mainly in young and middle-aged women. It is caused by dysfunction of the internal urethral sphincter and pelvic floor muscles, relaxation of the fascia and ligaments and high mobility of the urethra [5]. Its appearance can be triggered by stressful situations such as childbirth and weight gain [5]. SUI is the most common form of incontinence in women of reproductive age, with an incidence of 5% to 60% worldwide [7]. It occurs after physical exertion such as running, jumping, any physical exercise, coughing, or sneezing [8,9]. It has been observed that healthy women with proper urinary continence before pregnancy will experience SUI in 15–21% [10].
Women who develop postpartum SUI have been observed to have increased bladder-neck mobility before delivery compared with those without urinary incontinence [11]. Women who experience SUI after childbirth may not return to normal function and may have permanent urinary incontinence, specifically urge urinary incontinence (UUI). In particular, studies have shown that in women who experienced urinary incontinence 3 months after childbirth, these symptoms persisted even after 6 and 12 years by 24% and 38%, respectively [12]. The study by Ferrari et al. revealed that women who performed Pelvic Floor Muscle Training (PFMT) during pregnancy rather than only in the postpartum period were at lower risk of having symptoms of SUI [13].
UUI is characterized by an urgent need to urinate that cannot be postponed, followed by an involuntary loss of urine and nocturia or frequent urination [14]. A systematic review of 22 studies showed that UUI occurs in 1.8% to 30.5% in Europe, 1.7% to 36.4% in the USA and 1.5% to 15.2% in Asia [5]. The appearance of this particular subtype is associated with age, with a greater worsening of symptoms in women near the age of 70. Its symptoms can cause intense anxiety and depression and have a negative effect on the quality of life of these women [5].
Mixed UI is the most common form of urinary incontinence that combines the two previous subtypes. Its prevalence increases with age and tends to be more common in women aged > 65 years. MUI has the greatest impact on quality of life. The symptoms tend to worsen rather than improve. Studies have reported low remission rates. Only 8% of women with mild or moderate MUI will experience complete remission after 4 years of follow-up [5].
Worldwide, rates of urinary incontinence range from 15 to 52%, with a higher incidence in women, which has a significant impact on quality of life (QOL) [15]. Studies have shown that the problem gets worse in pregnancy and is observed in 30–35% during the third trimester [16]. Changes in the neuromuscular function of the urethral sphincter during pregnancy that may persist postpartum increase the likelihood of urinary incontinence [17]. The risk of urinary incontinence after childbirth, especially in the 4–18 months after childbirth, doubles in women who experience incontinence during pregnancy [11,18].
During the postpartum period, the rates range from 7 to 12% [19]. Approximately 34.3% of women worldwide experience urinary incontinence, while 8.5% of these women need to use pads on a daily basis [20]. In relation to primiparous women, studies have shown that during the first 12 months after giving birth, 55% of primiparous women will experience urinary incontinence [21]. Some cases of urinary incontinence are temporary and the symptoms subside after three months have passed since delivery. But if these symptoms persist, the chances increase to 92% that the problem will persist 5 years later [22].
Worldwide, reported rates of urinary incontinence in women aged 20 years and older are 45% in the USA, 46% in Australia, 30.9% in China, 25% in Norway, 48% in Germany, 46% in Denmark [23], 11% in Pakistan [24], in Turkey from 20.9 to 37.11% [15], in Qatar 20.6% and in the United Arab Emirates 20.3% [3]. In France, 1 in 4 women report urinary symptoms, the severity of which depends on age, body mass index and number of deliveries [25].
The pelvic floor consists of muscles, fascia and ligaments which are responsible for supporting the pelvic organs and maintaining their proper function. Pregnancy and childbirth can cause damage to both the structure and function of the pelvic floor [9]. Hormonal and anatomical changes are observed, relaxation of the pelvic floor muscles and subsequently their reduced contractility, and the weakening of the supporting structure of the urethra as a result of pregnancy, which increases the risk of urinary incontinence after childbirth [9]. At a hormonal level, the increased concentration of estradiol during pregnancy can adversely affect the metabolic capacity of pelvic floor muscle fibers [14].
During pregnancy and the postpartum period, most women with incontinence recover their symptoms as this is not a life-threatening condition. Urinary incontinence, if it does not subside automatically after training the pelvic floor muscles, can be combined with the appearance of accompanying problems, such as embarrassment, shame, sexual dysfunction, lack of self-esteem and social isolation, which can be particularly disturbing and lead to anxiety and depression with long-term effects on the woman’s quality of life [26]. Urinary incontinence is a major problem of psychosomatic morbidity that causes substantial damage to the quality of life [27]. The scientific community tends to search for aggravating factors. These factors are divided into modifiable and non-modifiable risk factors.
Modifiable risk factors include smoking, mode of delivery, oxytocin use and prolonged second stage of labor, pregnancy weight gain, stress and obesity [27]. A large body of literature demonstrates that obesity increases the risk of urinary incontinence, but this is not an independent risk factor. For example, waist circumference and height ratio can be a strong confounding risk factor [28]. Long-term obesity weakens the pelvic floor and the supporting structures of the urethra. It has been found that every five-unit increase in a woman’s BMI increases the potential risk of UI by 20–70% [29]. Early interventions, such as weight loss and pelvic floor muscle training, could be beneficial in reducing the incidence of urinary incontinence [30].
In the case of stress, it is observed that it can be both a risk factor in the possibility of urinary incontinence and an impact on those women who face this problem [5]. In addition, pelvic floor gynecological operations, limited physical function and especially the history of pregnancies, deliveries and perineal tears tend to be important modifiable risk factors [8,15]. Deliveries that happen with the use of suction combined with episiotomy, newborn birth weight, head circumference and gestational age may increase the risk of urinary incontinence [4,19].
Some of the non-modifiable risk factors are race, age, multiparity, fetal size and medical comorbidities such as hypertension, diabetes, history of constipation, the presence of more than 2 chronic diseases and chronic cough [27]. Also, important risk factors include gender, age of the woman over 35 years, age at menopause and ethnicity [31]. Studies have shown that pregnancy, childbirth, depression and history (first-degree relatives with urinary incontinence) influence the onset and progression of SUI [5].
Dysfunction of the autonomic nervous system and changes in the level of the neurotransmitter serotonin increase the level of catecholamines and circulating cortisol, which can cause changes in the function of the urethral sphincter and can trigger the possibility of urinary incontinence [5]. Diabetes is also associated with the occurrence of urinary incontinence, as elevated blood sugar can affect the pH of the urine, making it hypertonic and can increase episodes of urinary frequency and urgency [5].
Despite the high prevalence of urinary incontinence during pregnancy and the postpartum period, and its significant impact on women’s quality of life, the available research data remain fragmented and show significant heterogeneity in terms of incidence rates, subtypes and risk factors. Although urinary incontinence is often considered transient, a significant proportion of women experience persistent symptoms in the long term, with serious psychosocial consequences. The need for a clear evidence-based understanding of the natural course and interventions, particularly in the postpartum period, necessitates the conduct of this systematic review.
2. Aim
The aim of this systematic review was to synthesize recent evidence on postpartum urinary incontinence, focusing on its prevalence, associated risk factors and evidence-based preventive and management approaches.
More specific objectives:
To summarize the prevalence and incidence of urinary incontinence during the postpartum period.
To identify and evaluate risk factors associated with postpartum urinary incontinence based on the available evidence.
To assess the methodological quality of the included studies using a standardized appraisal approach.
To synthesize current evidence on preventive and management interventions for postpartum urinary incontinence.
To identify gaps in the literature and highlight priorities for future research.
3. Methodology
3.1. PECO Eligibility Criteria
Population (P): Postpartum women, regardless of age, parity, or mode of delivery.
Exposure (E): Potential risk factors for urinary incontinence (e.g., mode of delivery, number of pregnancies, maternal age, BMI, obstetric complications, perineal trauma, breastfeeding, hormonal changes).
Comparison (C): Postpartum women without the same risk factors or with different levels of exposure.
Outcome (O): Incidence, prevalence, severity, duration of urinary incontinence and its impact on quality of life.
Based on this framework, the formulated research question was as follows: “What are the risk factors associated with urinary incontinence during the postpartum period, and how do they influence its incidence, severity, and impact on women’s quality of life?”
3.2. Study Selection
This systematic review was based on the PRISMA method (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) and aggregated data published in international literature. A systematic bibliographic search was conducted across the electronic databases PubMed, Google Scholar and Scopus for studies concerning the relationship between risk factors and postpartum UI. Study selection was guided by predefined inclusion and exclusion criteria, as outlined below.
The review was limited to studies published within the last six years in order to reflect contemporary diagnostic criteria, assessment tools and current postpartum care practices related to urinary incontinence. The final search date was April 2025.
3.2.1. Inclusion Criteria
Women assessed for urinary incontinence within 12 months postpartum, regardless of follow-up duration.
Studies reporting any type of urinary incontinence during the postpartum period.
Research analyzing predictive or associated risk factors for postpartum urinary incontinence.
Original research studies (cross-sectional, cohort, case–control, or longitudinal).
3.2.2. Exclusion Criteria
Women with pre-existing urinary incontinence prior to pregnancy.
Studies not specifically reporting postpartum UI.
Studies including mixed populations without separate postpartum data.
Reviews, meta-analyses, case reports, letters, editorials, or conference abstracts.
Articles published in languages other than English.
3.3. Search Strategy
The search strategy was developed according to the PECO framework, using a combination of keywords and Boolean operators. The following terms and their variations were used:
Search String: (((postpartum women) OR (postnatal women) OR (women after childbirth)) AND ((urinary incontinence) OR (UI) OR (urine leakage))) AND ((risk factors) OR (predictive factors) OR (associated factors) OR (determinants)).
The initial search results were screened independently by two reviewers. After duplicates were removed, the remaining records were evaluated based on titles and abstracts according to the predefined inclusion criteria. Subsequently, the full texts of potentially relevant articles were assessed for eligibility. Disagreements regarding the inclusion of studies were resolved through discussion with a third reviewer to reach consensus. Only full-text articles published in English were included in the final synthesis, resulting in 36 studies selected for qualitative analysis.
3.4. Methodological Quality Assessment
The methodological quality and risk of bias of the studies were assessed using the NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies and the Mixed Methods Appraisal Tool (MMAT) for studies with mixed-methods designs, to ensure appropriate appraisal across different study types. These tools were applied to each selected study, examining specific criteria such as: sample representativeness, control of confounding factors, assurance that urinary incontinence did not pre-exist the study period, the final sample size and data adequacy. Studies were rated as low risk of bias when the majority of quality assessment domains were fulfilled and no critical methodological limitations were identified. Studies were rated as moderate risk when some domains were not fulfilled, but without substantial risk of bias affecting the validity of the results. The detailed quality ratings for each study, as derived from the application of these tools, are presented in Table 1 and Table 2.
4. Results
In the present systematic review, the PRISMA method was used. Focusing on studies published in the last 6 years, a total of 484 articles were retrieved from the PubMed database, 690 from Google Scholar and 147 from Scopus. 1321 results were obtained. Then, by reviewing the titles and abstracts of the articles, 810 articles and 182 abstracts were excluded, respectively. Finally, 329 full texts were assessed for eligibility. After reading the full text, 293 articles were excluded. Finally, 36 articles were included in this review. Risk of bias assessment indicated variability in methodological quality across studies, with detailed judgements presented in Table 1 and Table 2. The search algorithm refers to Figure 1.
4.1. Characteristics of the Included Studies
Table 3 summarizes the characteristics of the studies included in this review. The study sample in each of the articles varied from 140 to24.985 women. A total of 84.721 women were enlisted in the included studies. This systematic review included 10 cross-sectional studies [3,6,8,10,25,32,33,34,35,36], 14 prospective studies [4,6,13,16,18,21,26,27,29,31,37,38,39,41], 9 retrospective studies [7,11,12,14,17,20,40,42,43], 1 cohort study [22], 1 descriptive [15] and 1 longitudinal study [1].
4.2. Data Collection Methods
Data on urinary incontinence were collected either through telephone interviews [10,36,38] or via self-administered questionnaires [3,6,9,11,15,18,27,32,33,39], provided to the participants. Some of the studies used ICIQ-UI SF Questionnaire [1,13,14,16,22,30,35,38,42] and two studies used PFDI-20 and ICIQ-FLUTS Questionnaire, respectively [20,21]. Three researchers, through UDI-6 and IIQ-7 questionnaires, tried to reveal the areas in the quality of life of the women that may have been influenced by the urine leakage [4,17,25,31]. Rajavuori et al. questionnaire based on the Wexner incontinence score [29].
Juraskova et al. screened for symptoms of anxiety and postpartum depression in new mothers by means of the Edinburgh Postnatal Depression Scale Questionnaire [26]. One researcher used a combined reproductive health and kidney conditions—urology questionnaire in order to cover areas such as menstrual history, pregnancy history, family history of urinary tract issues and urinary symptoms [34]. Last but not least, Liu et al. performed a clinical examination assessing the woman’s ability to contract their pelvic floor muscles using the modified Oxford grading system [7]. The assessment of predictive risk factors for urinary incontinence focused on either the intrapartum and postpartum period or the prenatal period.
4.3. Risk Factors Identified in Individual Studies
In the case of researchers who used telephone interviews, Zhong et al. focused on maternal age and women’s lack of knowledge, while the other two studies searched for confounding factors such as obesity and weight gain during pregnancy, history of pregestational SUI, age of the woman, type of delivery and pregestational diabetes. The duration of the follow-up was not more than one year postpartum [10,40,43].
In the case of self-administered questionnaires, Liu et al. revealed two risk factors, such as the mode of delivery and episiotomy [9]. Jansson et al. [18,39] and Patel et al. [27] also searched for additional factors such as maternal age, connective tissue deficiency, familial pelvic floor dysfunction and history of urinary tract infection. Alamri et al. focused on multiparity, maternal age and vaginal delivery [3] while Subki et al. measured the Body Mass Index and examined an important confounding factor, which was fecal incontinence [33].
4.4. Findings Based on Measurement Instruments
The International Consultation on Incontinence Questionnaire—Urinary Incontinence Short Form (ICIQ-UI SF) was used by 9 researchers in this review. Most of them were focused on maternal age, multiparity, family history of UI, high birth weight, BMI postpartum, vaginal delivery, especially forceps delivery [42], interdelivery interval less than 41 months [14] and episiotomy or spontaneous tears [13,16,22,35,38,42]. Diez-Itza et al. referred to the prolonged second stage of labor for more than 1 h and to the SUI during pregnancy [1]. Wang et al. assessed chronic coughing and constipation as the main risk factors for UI [30].
The Pelvic Floor Distress Inventory Questionnaire (PFDI-20) was the measurement instrument of Cheng et al., which assessed the impact that pelvic floor disorders have on quality of life in women [20]. Number of pregnancies, oxytocin use and delivery method were the main risk factors. Besides these, they mentioned three additional risk factors such as occupation, residence and educational level. ICIQ-FLUTS Questionnaire evaluated the severity and impact of female lower urinary tract symptoms on quality of life [21]. Huang et al. found that family history, perineal laceration after vaginal birth, frequent coughing and constipation were some of the risk factors that were revealed in their study. They also searched for a different risk factor, which was the consumption of coffee or tea [21].
The use of the Urinary Distress Inventory Questionnaire (UDI-6) and Incontinence Impact Questionnaire (IIQ-7) helped the researchers to estimate the quality of life in women who suffer from urine leakage [4,17,25,31]. Naorungrot et al. searched for risk factors such as diabetes mellitus, intrauterine growth restriction, stillbirth, breech presentation and multiple pregnancies [31]. Abushamma et al. referred to smoking, physical inactivity, unemployment and caffeine consumption as possible risk factors for UI [25]. Chang et al. found that maternal age, stillbirth and severe perineal lacerations were the risk factors for UI [17], while Ahlund et al. referred only to urinary leakage symptoms as a risk factor, before and during pregnancy [4].
Bonasia et al. used the National Health and Nutrition Examination Survey (NHANES), a program of the National Center for Health Statistics, to assess the health status of reproductive-age women. This was the main strength of the above study and also the assessment of urinary incontinence during the first 24 months after birth. Among the risk factors of UI were birth weight more than 4000 g and smoking [34].
4.5. Primary Risk Factors for Postpartum Urinary Incontinence
The results revealed that the primary risk factors for urinary incontinence during the postpartum period are vaginal delivery, obesity and maternal age. However, not only the above but also symptoms of UI before and during pregnancy, multiparity, the high birth weight of the newborn and the overall weight gain of the women during pregnancy are strong risk factors. The strengths of the study of Magnani et al. were the number of women who had been followed up for a period of over 12 to 24 months after birth. The main risk factor was the weight gain during pregnancy. The cases of UI were improved within the period of the 12th and 24th months after birth [32]. The influencing factors from the included studies are presented in Table 4.
4.6. Strengths and Limitations of the Included Studies
Ahlund’s study had a number of limitations that may have influenced the results, such as the fact that the study sample came only from two delivery wards of one hospital in Stockholm, and there was a lack of information regarding the women’s history before pregnancy [4]. The studies of Diez-Itza and Gabilondo were the only studies that investigated the long-term persistence of urinary incontinence from 6 months to 12 years after the first delivery. The very long follow-up was the main strength of these studies. The main limitation of the study of Diez-Itza was that it was not possible to perform a stress test in order to assess a strong risk factor, such as antenatal bladder neck mobility [1,37].
The main strength of Chang et study was the follow-up time with multiple time points, 3, 6 and 12 months after birth [41]. The study of Pang et al. had several limitations, such as the loss to follow-up of a high percentage of participants and the unmeasurement of the frequency and volume of urine leakage and its impact on the women’s quality of life [6]. Patel’s study gathered a population of white, college-educated women, which may not allow the generalization of the results to other populations [27]. The follow-up time of the included studies is presented in Table 5.
Zhong et al. included women with a history of two deliveries, so the generalizability of the results to women with greater parity was not possible [40]. The limitation of the cross-sectional study of Abushamma et al. was that there was no BMI data for all the Palestinian women owing to the unwillingness of many women to reveal their weight for scientific reasons [25]. The strength of Ferrari’s study relied on the large amount of data collected from the beginning of pregnancy till the 12th month after birth to assess the risk factors that may lead to UI during the postpartum period [13].
4.7. Risk Prediction Models
Huang et al. developed a risk prediction model for urinary incontinence during the postpartum period. They are based on the following parameters: urinary incontinence during pregnancy, family history of urinary incontinence, consumption of caffeine, frequent cough and last but not least mode of delivery [21]. Zhang et al. created another risk-predictive model including pre-pregnancy BMI, height, delivery mode and induction method, fetal weight, stress urinary incontinence during pregnancy and perineal condition [43]. The risk predictive models facilitate early prevention and are significant achievements in this field.
The results from the studies are presented in Figure 2.
5. Discussion
5.1. Sociodemographic Predictors-Body Mass Index and Obesity as Risk Factors
Sociodemographic factors identified, such as age, education, BMI and unemployment, are important factors associated with postpartum urinary incontinence. Regarding increased BMI, studies suggest that it may be associated with increased pressure on the bladder and may impair blood supply to this area [2,33]. In the study by Jia et al., vaginal delivery combined with high BMI was strongly associated with urinary incontinence during the postpartum period, while the problem was more likely to resolve in women with low BMI, in those who had delivered by cesarean section and in women who had mild symptoms of urinary incontinence [38].
The study by Pang et al. shows that proper management of conditions such as obesity and diabetes may be associated with a reduction in the frequency of urinary incontinence episodes [6]. The study by Wang et al. confirms that obesity and BMI are associated with an increased risk of urinary incontinence one year postpartum [49]. Control of weight gain appears important and pregnant women should be informed about the recommended weight gain during pregnancy.
5.2. Mode of Delivery and Obstetric Interventions
In Siahkal’s study et al., spontaneous vaginal delivery, invasive vaginal delivery and episiotomy were associated with a higher likelihood of urinary incontinence [19]. Meta-analysis by Wang et al. showed that maternal BMI, pregnancy and vaginal delivery were associated with postpartum UI, particularly SUI, while cesarean section appeared to be associated with a lower likelihood of UI. Regarding vaginal delivery, the use of forceps was associated with higher rates of UI, whereas vacuum extraction was not associated with an increased risk [2]. Gao et al. reported that vaginal delivery, newborn’s weight, duration of the second stage of labor, increased BMI and epidural analgesia were associated with postpartum urinary incontinence [11].
5.3. Prevalence and Characteristics of Postpartum UI
The study by Liu et al. reported that women who delivered vaginally had a higher prevalence of SUI compared to those with cesarean section, while episiotomy was associated with increased SUI rates [7]. The study by Chang et al. demonstrated that the prevalence of SUI one year after vaginal birth was 16.5%, with a significantly higher prevalence in older primiparous women (>35 years) compared to younger primiparous women [17].
Zhong et al. reported an association between prior postpartum SUI and increased likelihood of SUI in multiparous women one year postpartum [40]. The one-year follow-up period is commonly considered appropriate, as pelvic floor recovery typically occurs within this timeframe [39].
5.4. History of UI and Long-Term Predictors
The longitudinal study by Pang et al. showed that spontaneous and instrumental vaginal delivery, diabetes, middle age, chronic cough, excessive gestational weight gain and smoking were associated with SUI [6]. Novo et al. reported that age is associated with urinary incontinence, potentially due to age-related changes in urethral sphincter muscle fibers [10]. According to Dias do Rego et al., home birth was associated with a higher likelihood of stress urinary incontinence compared to hospital birth [8].
Huber et al. reported that urinary incontinence four years postpartum was more prevalent among women who experienced pelvic inflammatory symptoms during the first postpartum year [50]. Moossdorf-Steinhauser et al. found that the prevalence of urinary incontinence increased over time postpartum [44]. Management strategies should be individualized based on symptom severity [5].
5.5. Lifestyle, Exercise and Modifiable Factors
Although pelvic floor muscle function typically improves 6–10 weeks postpartum, several studies indicate that urinary incontinence may persist for up to one year [31]. Abushamma et al. reported that lack of physical exercise was associated with higher rates of urinary incontinence [25]. Yang et al. found that vaginal delivery was the factor most strongly associated with postpartum urinary incontinence [35].
5.6. Pathophysiological Mechanisms
Episiotomy has been associated with alterations in pelvic floor structures, particularly connective tissue and neuromuscular stretching [22]. Postpartum pelvic floor tissues may undergo neurological and collagen-related changes, which may contribute to pelvic floor dysfunction [11]. Dai et al. reported that lateral episiotomy was associated with more severe symptoms of stress urinary incontinence [51].
5.7. Protective Factors
Ferrari et al. identified low body weight and cesarean section as factors associated with lower rates of UI [13]. Pizzoferrato et al. reported that cesarean section was associated with lower urethral mobility and reduced urinary symptoms [45]. However, cesarean section remains controversial, as vaginal delivery also confers maternal and neonatal benefits [46].
Zhang et al. found that epidural analgesia was associated with higher rates of postpartum SUI, possibly due to prolonged labor duration [43]. Liu et al. reported that multiparity was associated with a higher likelihood of postpartum SUI [9]. Urethral hypermobility has been linked to mechanical strain during pregnancy and vaginal delivery [39].
Patel et al. reported that previous urinary incontinence and vaginal delivery were strongly associated with postpartum UI [27]. Similarly, Wang et al. identified urinary incontinence during pregnancy, delivery mode, maternal age and gestational age as key prognostic factors associated with postpartum UI [30]. Xu et al. reported that a longer inter-delivery interval was associated with lower rates of postpartum urinary incontinence [14].
5.8. Socioeconomic and Psychosocial Influences
Financial difficulties, psychosocial stress and reduced social support were associated with increased urinary incontinence symptoms [13,52]. Chang et al. reported that full-time employment was associated with postpartum urinary incontinence [16]. Abushamma et al. confirmed similar findings [25].
Xue et al. identified genetic, lifestyle and socioeconomic factors associated with urinary incontinence [23].
5.9. Endocrinological, Biological and Quality-of-Life Factors
Hormonal changes during pregnancy may influence the development of SUI [53,54]. Genetic and microbiome alterations have been associated with urinary incontinence [21,55]. Juraskova et al. reported an association between urinary incontinence and depression [3,26].
6. Strengths and Limitations
This systematic review synthesizes recent evidence on postpartum urinary incontinence using a structured and transparent methodology in accordance with PRISMA guidelines. The inclusion of multiple study designs and a broad range of risk factors provides a comprehensive perspective on postpartum urinary incontinence as a multifactorial condition, while dual independent screening enhanced the robustness of study selection.
Nevertheless, heterogeneity across studies in outcome measures, assessment tools, definitions of key variables and timing of postpartum assessment should be acknowledged. Due to heterogeneity in outcome measures and assessment tools, results were synthesized narratively rather than quantitatively, and findings should therefore be interpreted with caution. Residual confounding cannot be excluded, as most included studies were observational and adjustment for all potential confounders was not uniformly possible. Limitations of the review process should also be considered, including restriction to English-language publications, selection of specific electronic databases and the potential for publication bias. The absence of protocol may further affect transparency.
7. Conclusions
Episodes of urinary frequency and urinary incontinence may significantly affect the quality of life of a woman, her psychology, sexual life and the way she copes with daily activities, causing socio-economic costs [44,52]. The early recognition and investigation of the risk factors associated with this dysfunction could facilitate health professionals to develop prevention and treatment strategies, emphasizing the change in obstetric care, improving the prognosis and reducing the adverse effects that these could have on a woman’s quality of life [22]. The strategy of developing prognostic models in the coming years may be the only way for the early identification and follow-up of women at high risk for urinary disorders.
Detection of the type of urinary incontinence by healthcare professionals, lifestyle modifications, monitoring women’s body weight and encouraging them to follow a program of pelvic floor muscle exercises should be a priority for professionals [41]. Strengthening the knowledge of healthcare professionals is necessary to provide targeted intervention to patients when deemed necessary. At the same time, the strengthening of awareness and the understanding of dysfunctions by the women themselves could significantly reduce long-term morbidity. Women have a right to know the possible dysfunctions they may experience from their pelvic floor, as this would allow them to control some of the modifiable risk factors that can be avoided.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diez-Itza I. Zubikarai M. Galan C. Ginto L. Saro J. Arrue M. Factors involved in the persistence of stress urinary incontinence from postpartum to 12 years after first delivery Neurourol. Urodyn.2020391849185510.1002/nau.2444232558998 · doi ↗ · pubmed ↗
- 2Wang K. Xu X. Jia G. Jiang H. Risk factors for postpartum stress urinary incontinence: A systematic review and meta-analysis Reprod. Sci.2020272129214510.1007/s 43032-020-00254-y 32638282 · doi ↗ · pubmed ↗
- 3Alamri A. Alqahtani M. Asiri K. Albagami S. Hassan B.A. Alhumaid R.M. Alharbi A. Safar O. Khan M.A. Prevalence and Risk Factors of Postpartum Urinary Incontinence in Southern Saudi Arabia: A cross-sectional study King Khalid Univ. J. Health Sci.20249242810.4103/KKUJHS.KKUJHS_30_23 · doi ↗
- 4Åhlund S. Rothstein E. Rådestad I. Zwedberg S. Lindgren H. Urinary incontinence after uncomplicated spontaneous vaginal birth in primiparous women during the first year after birth Int. Urogynecol. J.2020311409141610.1007/s 00192-019-03975-031139858 PMC 7306031 · doi ↗ · pubmed ↗
- 5Li Q. Cheng Y. Shi H. Xue K. Zhou F. Advances in the natural history of urinary incontinence in adult females J. Obstet. Gynaecol.202343217177410.1080/01443615.2023.217177436772931 · doi ↗ · pubmed ↗
- 6Pang H. Lv J. Xu T. Li Z. Gong J. Liu Q. Wang Y. Wang J. Xia Z. Li L. Incidence and risk factors of female urinary incontinence: A 4-year longitudinal study among 24985 adult women in China BJOG Int. J. Obstet. Gynaecol.202112958058910.1111/1471-0528.1693634536320 PMC 9298368 · doi ↗ · pubmed ↗
- 7Liu X. Wang Q. Chen Y. Luo J. Wan Y. Factors associated with stress urinary incontinence and diastasis of rectus abdominis in women at 6–8 weeks postpartum Urogynecology 20232984485010.1097/SPV.000000000000135337093577 PMC 10521785 · doi ↗ · pubmed ↗
- 8do Rêgo A.D. Peterson T.V. Bernardo W.M. Baracat E.C. Haddad J.M. Comparison of stress urinary incontinence between urban women and women of indigenous origin in the Brazilian Amazon Int. Urogynecol. J.20213239540210.1007/s 00192-020-04439-632681348 · doi ↗ · pubmed ↗