Real-World Treatment Patterns and Survival in Uveal Melanoma: A Multicenter Cohort Study by the Turkish Oncology Group (TOG)
Sercan On, Selin Cebeci, Zeynep Hande Turna, Zeynep Gülsüm Güç Sevgen, Deniz Can Guven, Sadettin Kılıçkap, Mehmet Nuri Başer, Bilgin Demir, Sedat Biter, Ertuğrul Bayram, Berkay Yeşilyurt, Doğan Uncu, Ahmet Melih Arslan, Elif Atağ Akyürek, Hayati Arvas, Zuhat Urakçı

TL;DR
This study examines treatment patterns and survival outcomes in metastatic uveal melanoma patients in Türkiye, highlighting the limited efficacy of chemotherapy and potential benefits of liver-directed and immunotherapy approaches.
Contribution
The study provides real-world evidence on treatment patterns and survival outcomes in metastatic uveal melanoma from a non-Western population in Türkiye.
Findings
Liver-directed treatments, such as radioembolization, were associated with longer overall survival in metastatic uveal melanoma patients.
Dual immune checkpoint blockade emerged as an independent favorable prognostic factor for survival.
HLA-A*02:01 positivity was low, and access to tebentafusp was limited in the studied population.
Abstract
Uveal melanoma is a rare but aggressive malignancy with a strong tendency to metastasize, particularly to the liver. Once metastasis occurs, treatment options are limited, and survival outcomes remain poor. This multicenter study evaluates real-world outcomes of patients with metastatic uveal melanoma treated across various institutions in Türkiye. We examined both systemic treatment options, including immune checkpoint inhibitors, chemotherapy, and targeted therapies, as well as local treatment approaches, such as liver-directed therapies. By analyzing their effectiveness and survival impact in routine clinical practice, our findings provide a comprehensive overview of current therapeutic strategies. This study offers valuable insights to help clinicians optimize treatment selection and highlights areas where further research and improved therapeutic approaches are needed.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
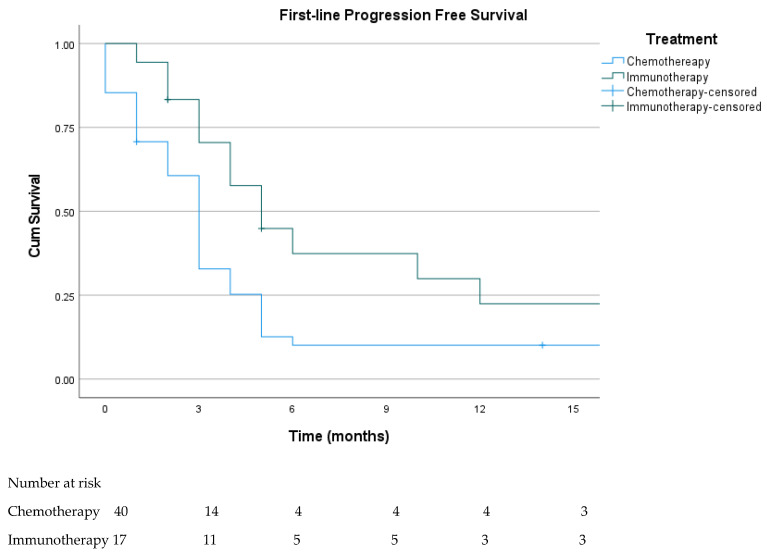 Figure 1
Figure 1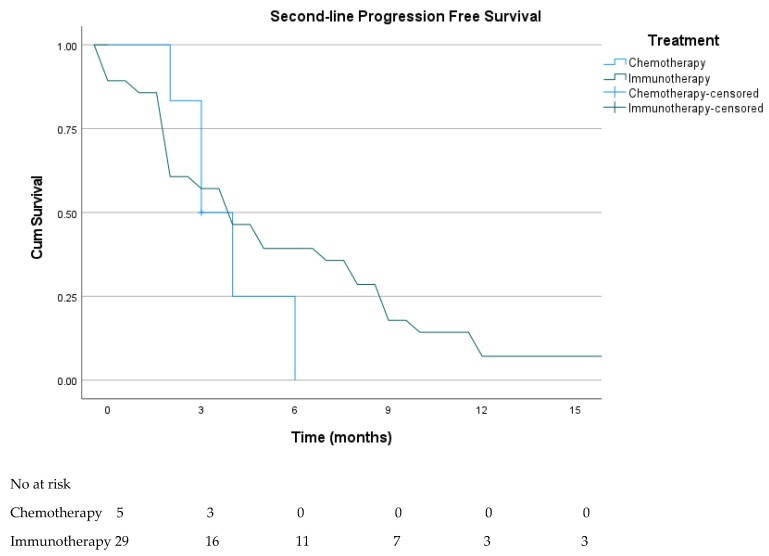 Figure 2
Figure 2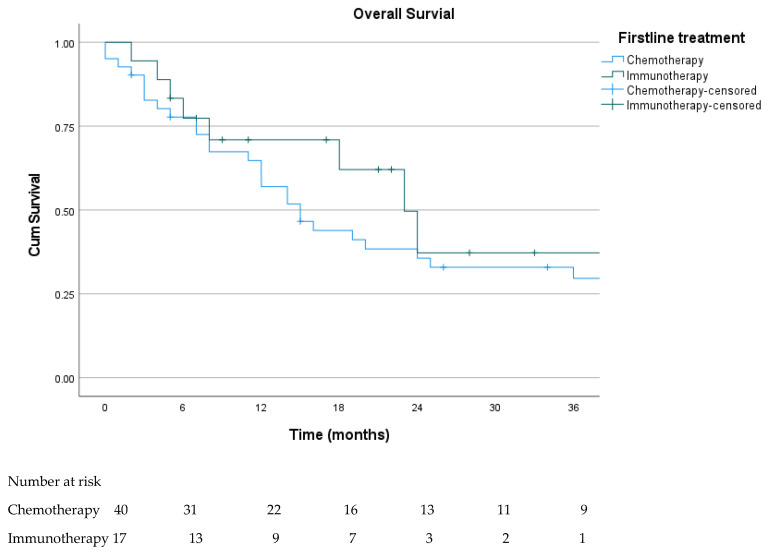 Figure 3
Figure 3| All Patients N (%) | |
|---|---|
| Age (years) | 56.2 (SD ± 12.2) |
| Sex | |
| Male | 62 (54.9) |
| Female | 51 (45.1) |
| T category | |
| Tx | 38 (33.6) |
| T1 | 13 (11.5) |
| T2 | 26 (23) |
| T3 | 19 (16.8) |
| T4 | 17 (15.1) |
| N category | |
| Nx | 20 (17.7) |
| N0 | 88 (77.9) |
| N1 | 4 (3.5) |
| M category | |
| M0 | 101 (89.4) |
| M1 | 12 (10.6) |
| Tumor localization | |
| Choroid and ciliary body | 81 (71.7) |
| Iris | 8 (7.1) |
| Unknown | 24 (21.2) |
| Primary treatment | |
| Enucleation | 67 (59.3) |
| Plaque brachytherapy | 40 (35.4) |
| No local treatment | 6 (5.3) |
| Recurrence | |
| No | 48 (47.5) |
| Local | 4 (4) |
| Distant | 49 (48.5) |
| All Metastatic Patients | Recurrence Metastatic Patient | Denovo Metastatic Patient N (%) | ||
|---|---|---|---|---|
| Age (years) | ||||
| Median (IQR) | 56 (47–64) | 54 (44.5–63.5) | 61.5 (53.7–67.5) | |
| Sex | ||||
| Male | 37 (60.7) | 29 (59.2) | 8 (66.7) | |
| Female | 24 (39.3) | 20 (40.8) | 4 (33.3) | |
| Metastatic site | ||||
| Isolated hepatic | 37 (60.7) | 31 (63.3) | 6 (50) | |
| Isolated extrahepatic | 4 (6.5) | 3 (6.1) | 1 (8.3) | |
| Both | 20 (32.8) | 15 (30.6) | 5 (41.7) | |
| Hepatic metastasis number | ||||
| 1–3 lesions | 17 (29.8) | 16 (34.8) | 1 (9.1) | |
| ≥4 lesions | 40 (70.2) | 30 (65.2) | 10 (90.9) | |
| Hepatic involvement pattern | ||||
| Unilobar | 14 (24.6) | 12 (26.1) | 2 (20) | |
| Bilobar | 43 (75.4) | 34 (73.9) | 8 (80) | |
| HLA 02*01 status | ||||
| Positive | 5 (8.2) | 5 (10.2) | 0 (0) | N/A |
| Negative | 12 (19.7) | 11 (22.4) | 1(8.3) | |
| Unknown | 44 (72.1) | 33 (67.3) | 11 (91.7) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Oncology and Treatments · Veterinary Oncology Research · Multiple and Secondary Primary Cancers
1. Introduction
Uveal melanoma (UM) is the most common primary intraocular malignancy in adults, accounting for 3–5% of all melanomas and affecting 5–7 individuals per million annually [1]. UM originates from any component of the uveal tract, but the vast majority arise in the choroid or ciliary body, whereas iris tumors account for only a small minority [2]. Most patients present with localized disease; fundoscopic examination can detect the lesion. Although it is not mandatory to perform a biopsy to confirm the diagnosis, a biopsy is recommended to enable molecular testing for the patient. Staging was performed according to the AJCC 8th edition criteria for uveal melanoma [3].
Primary UM is typically managed with surgery or radiotherapy, both of which achieve excellent local control in contemporary practice [1]. Although local recurrence is uncommon, metastatic spread remains frequent, typically emerging within a few years of initial treatment, with occasional relapses occurring more than a decade later [4]. The liver is the most frequent, and often the sole, site of metastasis, and unlike cutaneous melanoma, lymph node and brain involvement is uncommon [5]. This makes liver-directed locoregional therapies a rational strategy; however, while improving hepatic disease control, these approaches have not consistently translated into a meaningful survival advantage [6].
Metastatic UM carries a poor prognosis, with a median survival typically around one year and fewer than 15% of patients alive at five years [7]. Tebentafusp, a gp100-targeted TCR–CD3 bispecific agent, is the only systemic therapy proven to extend overall survival in a randomized trial, increasing median survival to nearly two years, but its benefit remains limited to HLA-A02:01–positive patients [8]. For HLA-A02:01–negative patients, therapy relies mainly on immune checkpoint inhibitors (ICIs), although responses remain modest and evidence derives primarily from non-randomized studies [9,10,11,12]. Importantly, much of the existing evidence in metastatic UM is based on small observational cohorts or phase II studies, and robust randomized data remain limited. Current literature is further constrained by heterogeneous treatment practices and the lack of comprehensive real-world datasets that capture the whole clinical trajectory from diagnosis through multiple lines of therapy, including the interplay between local and systemic treatments.
To address these knowledge gaps, this multicenter study, coordinated by the Turkish Oncology Group (TOG) and conducted across 19 tertiary oncology centers, presents a nationwide real-world evaluation of UM. By incorporating data from both localized and metastatic disease settings, the study provides a comprehensive assessment of treatment patterns, surveillance outcomes, and the effectiveness of systemic therapies in routine clinical practice.
2. Materials and Methods
This multicenter retrospective cohort study, coordinated by the Turkish Oncology Group (TOG), included patients with histopathologically or clinically confirmed uveal melanoma who were evaluated, followed, or treated at 19 tertiary oncology centers between January 2012 and June 2025. Patients receiving only local treatment or surveillance were also included. Follow-up and surveillance of patients managed in the localized disease setting were conducted according to the routine clinical practice and institutional protocols of each participating center. Patients who were never referred to medical oncology clinics, were managed entirely outside oncology centers, or were diagnosed with an active concurrent malignancy were excluded. June 2025 served as the data cutoff. A minimum contribution of two patients per center was required for inclusion in the study. Patient contribution varied across participating centers, ranging from two to 13 patients per center.
Baseline demographic and clinical characteristics were summarized using descriptive statistics. Categorical variables were reported as frequencies and percentages, while continuous variables were presented as means with standard deviation (SD) or medians with interquartile range (IQR), as appropriate. Group comparisons were performed using the chi-square or Fisher’s exact test for categorical variables and Student’s t-test or Mann–Whitney U test for continuous variables.
Treatment response was assessed using RECIST v1.1. Objective response rate (ORR) was defined as the proportion of patients who achieved a complete or partial response, and disease control rate (DCR) was defined as the proportion who achieved a complete response, a partial response, or stable disease.
Systemic treatments were grouped into immunotherapy (nivolumab, ipilimumab, nivolumab–ipilimumab, pembrolizumab, tebentafusp) and cytotoxic chemotherapy. Treatment efficacy was evaluated across all applicable therapy lines.
Overall survival (OS) was defined as the time from metastatic diagnosis to death or last follow-up, and progression-free survival (PFS) as the time from systemic therapy initiation to progression or death. Survival outcomes were estimated using the Kaplan–Meier method and compared using the log-rank test. Prognostic factors for OS were analyzed using Cox proportional hazards models, with results expressed as hazard ratios (HRs) and 95% confidence intervals (CIs). Variables included in the multivariate Cox regression model were predefined a priori based on established clinical relevance in the literature and data availability across centers [3,6,7,10].
All statistical analyses were conducted using SPSS version 27 (IBM Corp., Armonk, NY, USA). A two-sided p-value < 0.05 was considered statistically significant. The study was approved by the institutional review boards of all participating centers and conducted in accordance with the Declaration of Helsinki. Informed consent was waived due to the retrospective study design.
During the editing of the manuscript, the authors used ChatGPT 5.2 (OpenAI) exclusively for language editing, grammar correction, and improving clarity of expression. The tool was not used for data analysis, study design, result interpretation, generation of scientific content, or creation of figures/tables. The authors entirely produced all scientific interpretations, analyses, and conclusions. The authors reviewed and verified all AI-assisted text and take full responsibility for the final content.
3. Results
3.1. All Cohort
A total of 113 patients were included in the study. Of these, 62 patients (54.9%) were male, and the mean age was 56.2 years (SD ±12.2). At diagnosis, 101 patients (89.4%) presented with localized disease, whereas 12 (10.6%) had de novo metastatic disease. Baseline characteristics are summarized in Table 1. The choroid or ciliary body was the most common primary tumor site (71.7%), followed by the iris (7.1%), while tumor localization was not reported in 21.2% of cases. Most melanomas arose de novo, whereas six patients (5.3%) developed melanoma from a pre-existing nevus.
With respect to local treatment, enucleation was performed in 67 patients (59.3%), plaque brachytherapy in 40 (35.4%), and six patients (5.3%) did not receive any local treatment. Radiotherapy was additionally administered to 27 patients, primarily for positive surgical margins or local recurrence. Among the 101 patients under surveillance following local treatment, the median follow-up was 42.8 months (IQR, 22.1–79.8). Over the course of follow-up, four patients (4%) experienced isolated local recurrence, all treated with salvage radiotherapy, whereas 49 patients (48.5%) developed distant metastases.
3.2. Metastatic Cohort
Sixty-one patients had metastatic disease, including 12 (10.7%) with de novo metastases and 49 (43.4%) who developed metastases during follow-up. The liver was the predominant site of metastasis (93.5%), with isolated extrahepatic disease observed in only four patients (6.5%). Among patients with liver involvement, 70% had ≥4 lesions and 75% demonstrated bilobar distribution. The most common extrahepatic metastatic sites were the lung (20.4%), bone (18.4%), and lymph nodes (18.4%).
Patients with de novo and recurrent metastatic disease did not differ significantly in terms of age, sex, or baseline disease characteristics (Table 2). Among the 57 patients with liver metastases, 27 (47.4%) underwent liver-directed treatment, most commonly transarterial radioembolization (44.4%), followed by radiofrequency ablation (29.6%), surgical resection or hepatic arterial infusion (each 11.1%), and radiotherapy (3.2%). In most cases, locoregional therapy was administered as first-line treatment (25 of 27 patients). The number of procedures varied, with 14 patients treated once, seven twice, and the remainder three or more times, reaching up to ten procedures in a single patient. Approximately one-third of patients received concurrent systemic therapy, most commonly chemotherapy. The median PFS following liver-directed treatment was 4.1 months (95% CI, 2.8–5.2), and the addition of concurrent systemic therapy did not result in a significant improvement in PFS (log-rank p = 0.43).
HLA-A*02:01 testing was performed in 17 patients, of whom 5 (29.4%) were positive.
3.3. First-Line Treatment
Two patients with metastatic disease died before initiation of systemic therapy, whereas 59 received at least one line of treatment. The median follow-up among treated patients was 11.5 months (IQR: 2.7–24.7). In the first-line setting, most patients received cytotoxic chemotherapy (41/59, 69.5%), predominantly temozolomide (49.2%) or carboplatin/paclitaxel (18.6%). Immunotherapy was administered to 18 patients (30.5%), including nivolumab (n = 10), ipilimumab (n = 2), nivolumab–ipilimumab (n = 5), and tebentafusp (n = 1). Immunotherapy was administered to 18 patients (30.5%), including nivolumab (n = 10), ipilimumab (n = 2), nivolumab–ipilimumab (n = 5), and tebentafusp (n = 1). Although ORR (38.9%) and DCR (55.6%) were numerically higher in the immunotherapy group than in the chemotherapy group, the differences did not reach statistical significance (Table 3). Median PFS was significantly longer with immunotherapy (5.3 months) compared with chemotherapy (3.1 months), as shown in Figure 1 (log-rank p = 0.007). The single patient treated with tebentafusp achieved a partial response and remained progression-free at six months.
3.4. Second-Line Treatment
A total of 36 patients received second-line therapy, of whom 30 (83.3%) were treated with immunotherapy (nivolumab n = 24, ipilimumab n = 2, nivolumab–ipilimumab n = 4), while only six patients (16.7%) received chemotherapy. Among those treated with immunotherapy, the ORR and DCR were 26.7% and 46.7%, respectively, whereas no objective responses were observed in the chemotherapy cohort (DCR 16.7%). These differences were not statistically significant (p = 0.30 and p = 0.36). Median PFS was 4.4 months (95% CI, 1.9–6.9) for immunotherapy and 3.2 months (95% CI, 1.6–4.4) for chemotherapy, with no statistically significant difference observed between groups (log-rank p = 0.40; Figure 2).
3.5. Later-Line Treatment
Later-line therapy was administered to 19 patients, including chemotherapy in 11 (57.9%), immune checkpoint inhibitors in four (21%), tebentafusp in two (10.5%), and olaparib in one patient with a RAD54 mutation. Across all third-line treatments, the ORR was 15.8% and the DCR was 52.6%, with a median PFS of 4.1 months (95% CI, 2.8–5.2).
Among the two patients treated with tebentafusp, one achieved stable disease and remained on treatment for five months, while the other achieved a partial response but progressed after 13 months. Seven patients received fourth-line therapy, with no further treatments administered thereafter. A partial response was observed in one patient treated with ipilimumab, while no other objective responses were recorded.
3.6. Overall Survival
All metastatic patients were included in the Kaplan–Meier analysis. At the time of data cutoff, 18 patients (29.5%) were alive. Median overall survival (OS) was 16.0 months (95% CI: 9.3–22.7). In patients who were able to access immunotherapy in the first-line setting, median overall survival was 23.0 months (95% CI, 15.9–30.1), versus 15.0 months (95% CI, 10.2–19.8) in patients treated with first-line chemotherapy, with no statistically significant difference observed (log-rank p = 0.544) (Figure 3).
In univariate analysis, the presence of multiple liver metastases and extrahepatic involvement was associated with significantly worse OS (p = 0.02 for each), whereas liver-directed therapy and combination immunotherapy administered at any treatment line were associated with improved OS (p < 0.001 and p = 0.03, respectively). In multivariate analysis, local liver-directed therapy (HR 0.40, 95% CI, 0.19–0.84; p = 0.02) and combination immunotherapy (HR 0.31, 95% CI, 0.10–0.95; p = 0.04) remained independent favorable prognostic factors (Table 4).
4. Discussion
In this large multicenter national cohort, consistent with global epidemiologic trends, most patients presented with localized disease [1]. The choroid and ciliary body were the predominant primary sites (71.7%), while iris tumors were uncommon (7.1%), mirroring international patterns [2]. A notable proportion of missing T and N classifications limited complete AJCC staging, an essential constraint given the wide prognostic variation across stages [13]. Although plaque brachytherapy is the preferred local modality worldwide, enucleation remained the most frequently used approach in our cohort, likely reflecting institutional practice differences and treatment availability [14].
Despite effective local therapy, almost half of the patients eventually developed distant metastases, reflecting the well-known long-term relapse risk in uveal melanoma [5]. Monosomy 3, BAP1 mutations, and gene expression profiling class are recognized indicators of aggressive disease and increased recurrence risk in localized uveal melanoma, but these data were unavailable in our cohort [15]. Hepatic involvement was observed in 93.5% of patients with recurrent disease, consistent with the well-recognized hepatic tropism of UM [5]. A high liver metastatic burden (≥4 lesions) was present in nearly 70% of patients and was associated with poorer overall survival on univariate analysis, but this association was not retained after multivariate adjustment. Additional metastatic sites included the lung, bone, and lymph nodes, which are consistent with the literature [5].
Multiple liver-directed approaches have demonstrated improvements in response rates and PFS in phase II–III studies (HAI [16], TACE [17], radioembolization [18,19], IHP [6], PHP [20]), though a consistent overall survival benefit remains uncertain [7,21]. In our study, nearly half of the metastatic patients received liver-directed therapy, most commonly radioembolization, and this group demonstrated significantly longer overall survival, suggesting a potential benefit in real-world practice. However, as treatment allocation was not randomized, patients selected for liver-directed approaches were likely those with more favorable clinical characteristics, including better performance status and lower extrahepatic disease burden; therefore, these findings should be interpreted cautiously and should not be considered evidence of a causal treatment effect. Given the heterogeneity of liver-directed modalities and varying institutional practices, the observed survival benefit likely reflects outcomes in selected patients rather than a uniform treatment effect and should not be generalized across all liver-directed treatments. Evidence regarding the addition of concurrent systemic therapy remains limited. A recent CHOPIN trial reported improved PFS with nivolumab–ipilimumab combined with percutaneous hepatic perfusion; in contrast, our small subgroup treated concurrently did not show a clear advantage [22].
For many years, metastatic UM was managed with conventional chemotherapy, yet response rates consistently remained below 10%, and no survival benefit was demonstrated [23,24]. Our findings similarly confirmed the limited activity of cytotoxic agents. Uveal melanoma differs fundamentally from cutaneous melanoma, being primarily driven by GNA11 and GNAQ mutations that activate MAP kinase and YAP1 signaling pathways [25] and characterized by a low tumor mutational burden and an immunologically “cold” microenvironment [26]. These features likely underlie the limited efficacy of ICIs reported in the literature, with single-agent ICI achieving objective response rates below 10% and a median overall survival of approximately 10 months [10]. In our cohort, immunotherapy was predominantly administered as a single agent in the second and subsequent treatment lines, mainly due to reimbursement constraints. Although immunotherapy resulted in numerically higher ORR and DCR than chemotherapy, these differences were not statistically significant, which may partly be due to the limited sample size. Kaplan–Meier analysis did not demonstrate a statistically significant difference in OS between patients receiving first-line immunotherapy and those treated with chemotherapy, indicating that treatment sequence alone may not be an important determinant of survival in this population. However, the immunotherapy-treated subgroup was heterogeneous, including different immunotherapy strategies with distinct efficacy profiles, which represents a substantial limitation for interpreting our findings.
By simultaneously targeting complementary immune inhibitory pathways, dual blockage with anti-PD-1 and anti-CTLA-4 may partially overcome intrinsic immune resistance. Dual ICI has shown modest but superior activity compared with monotherapy in previous phase II trials, with median PFS of 3.0–5.5 months and OS of 12.7–19.1 months [9,27]. More recent evidence reinforces this pattern: a large systematic review of 1414 patients reported limited efficacy of ICIs overall but consistently better outcomes with dual therapy [10], and a real-world comparison showed higher ORR and longer PFS with nivolumab–ipilimumab versus anti–PD-1 alone, despite similarly limited OS (12–13 months) [11]. While doublet ICI was associated with improved survival in multivariate analysis in our cohort, the limited number of treated patients and the likelihood of preferential treatment of clinically fitter individuals warrant cautious interpretation.
Tebentafusp, a bispecific T-cell engager that redirects polyclonal T cells to gp100-expressing melanoma cells via CD3 binding and induces tumor cell apoptosis independently of tumor mutational burden, represents a significant therapeutic advance in metastatic uveal melanoma [8]. However, its global use remains limited by access constraints and ethnic variability in HLA-A02:01 prevalence. Reported frequencies range from ~40–50% in European/North American populations to ~20% in South American cohorts and as low as 10–15% in African ancestry groups, highlighting substantial geographical disparities in eligibility [28]. Although Türkiye-specific data are lacking, our study provides valuable early insight: among the 17 patients tested, only 5 (29.4%) were HLA-A02:01-positive. Consequently, only three patients received tebentafusp, preventing meaningful assessment of treatment outcomes. Real-world evidence suggests a potential benefit when sequencing tebentafusp with immune checkpoint inhibitors, and phase II data in previously treated patients report a median OS of 16.8 months [29,30]. Additionally, a propensity-score–adjusted analysis demonstrated superior OS with tebentafusp compared with nivolumab–ipilimumab in the first-line setting, reinforcing its role as the preferred frontline option where available [31].
In meta-analyses prior to the standard use of tebentafusp, the median survival was around 12 months, while in studies after tebentafusp, a median survival of approximately 20 months was achieved [32,33]. In our study, with the limited access of new treatments to patients, a median survival of 16 months was obtained, which is better than traditional survival but lower than studies where all patients had access to tebentafusp.
This study, due to its retrospective design, includes selection bias related to patient registration methods, institutional practices, and reimbursement arrangements that may differ across centers. Metastatic surveillance and follow-up strategies are limited to patients referred only to medical oncology clinics and, therefore, may not fully represent the population-based sample. Additionally, detailed information regarding treatment doses, modifications, durations, and toxicity in these patients could not be clearly obtained from the registry data. Because of the limited number of patients receiving doublet ICI, the small number of events, and missing performance status data, the multivariate analyses are underpowered and should be regarded as exploratory. Despite these limitations, this study provides one of the most comprehensive real-world datasets on uveal melanoma in our region.
5. Conclusions
In this large multicenter real-world cohort, nearly half of patients with localized uveal melanoma eventually developed metastatic disease, with the liver remaining the dominant site. Liver-directed therapy and doublet ICI were independently associated with improved overall survival, highlighting their role in selected patients. Chemotherapy demonstrated limited efficacy, whereas immunotherapy provided modest but clinically meaningful benefit. The low rate of HLA-A*02:01 positivity and restricted access to tebentafusp underscore important challenges for implementing the only therapy with a proven survival advantage. Overall, these findings help clarify current treatment patterns in Türkiye and emphasize the need for broader access to effective systemic therapies and prospective studies to optimize management strategies for metastatic uveal melanoma.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Krantz B.A. Dave N. Komatsubara K.M. Marr B.P. Carvajal R.D. Uveal melanoma: Epidemiology, etiology, and treatment of primary disease Clin. Ophthalmol.20171127928910.2147/OPTH.S 8959128203054 PMC 5298817 · doi ↗ · pubmed ↗
- 2Rodríguez A. Dueñas-Gonzalez A. Delgado-Pelayo S. Clinical presentation and management of uveal melanoma Mol. Clin. Oncol.2016567567710.3892/mco.2016.103728101347 PMC 5228280 · doi ↗ · pubmed ↗
- 3Amin M.B. Greene F.L. Edge S.B. Compton C.C. Gershenwald J.E. Brookland R.K. Meyer L. Gress D.M. Byrd D.R. Winchester D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging CA A Cancer J. Clin.201767939910.3322/caac.2138828094848 · doi ↗ · pubmed ↗
- 4Kujala E. Mäkitie T. KiveläT. Very Long-Term Prognosis of Patients with Malignant Uveal Melanoma Investig. Ophthalmol. Vis. Sci.2003444651465910.1167/iovs.03-053814578381 · doi ↗ · pubmed ↗
- 5Collaborative Ocular Melanoma Study Group Assessment of Metastatic Disease Status at Death in 435 Patients with Large Choroidal Melanoma in the Collaborative Ocular Melanoma Study (COMS)Arch. Ophthalmol.200111967067610.1001/archopht.119.5.67011346394 · doi ↗ · pubmed ↗
- 6Bagge R.O. Nelson A. Shafazand A. All-Eriksson C. Cahlin C. Elander N. Helgadottir H. Kiilgaard J.F. Kinhult S. Ljuslinder I. Isolated Hepatic Perfusion with Melphalan for Patients with Isolated Uveal Melanoma Liver Metastases: A Multicenter, Randomized, Open-Label, Phase III Trial (the SCANDIUM Trial)J. Clin. Oncol.2023413042305010.1200/JCO.22.0170536940407 PMC 10414734 · doi ↗ · pubmed ↗
- 7Khoja L. Atenafu E. Suciu S. Leyvraz S. Sato T. Marshall E. Keilholz U. Zimmer L. Patel S. Piperno-Neumann S. Meta-analysis in metastatic uveal melanoma to determine progression free and overall survival benchmarks: An international rare cancers initiative (IRCI) ocular melanoma study Ann. Oncol.2019301370138010.1093/annonc/mdz 17631150059 · doi ↗ · pubmed ↗
- 8Nathan P. Hassel J.C. Rutkowski P. Baurain J.-F. Butler M.O. Schlaak M. Sullivan R.J. Ochsenreither S. Dummer R. Kirkwood J.M. Overall Survival Benefit with Tebentafusp in Metastatic Uveal Melanoma N. Engl. J. Med.20213851196120610.1056/NEJ Moa 210348534551229 · doi ↗ · pubmed ↗