Impact of Fusion Partners and Transplantation Benefit in Intensively Treated KMT2A-Rearranged Acute Myeloid Leukemia
Heng Shen, Jiayuan Chen, Xiaoyuan Gong, Chunlin Zhou, Dong Lin, Kaiqi Liu, Benfa Gong, Guangji Zhang, Yan Li, Yuntao Liu, Shaowei Qiu, Bingcheng Liu, Ying Wang, Yingchang Mi, Qiuyun Fang, Jianxiang Wang, Hui Wei

TL;DR
This study shows that KMT2A-rearranged AML patients with specific fusion partners, like KMT2A::ELL, have better survival, and that stem cell transplantation benefits older patients more than younger ones.
Contribution
The study identifies age-dependent HSCT benefits and KMT2A::ELL as a favorable subtype in KMT2A-rearranged AML.
Findings
Patients with KMT2A::ELL fusion had significantly better 3-year overall survival (59.8%) compared to other subtypes (39.3%).
Hematopoietic stem cell transplantation (HSCT) significantly improved survival in patients over 20 years old but not in those aged 20 or younger.
Age and HSCT in first complete remission were independently associated with better overall and event-free survival.
Abstract
Acute myeloid leukemia with KMT2A rearrangements is challenging, characterized by diverse clinical outcomes. Given the varied clinical outcomes across different KMT2A fusion subtypes, the specific benefit of hematopoietic stem cell transplantation (HSCT) for each subgroup remains under-investigated, which is critical for making precise treatment decisions in the era of emerging targeted therapies. In this study, we analyzed 181 KMT2A-rearranged patients to determine how different fusion partners affect clinical outcomes. We found that patients with KMT2A::ELL had better outcomes compared to others. Crucially, our research revealed that the benefit of HSCT is highly dependent on patient age. While HSCT significantly improved survival for patients over the age of 20, it did not provide a statistically significant survival advantage for patients aged 20 or younger. We suggest that…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
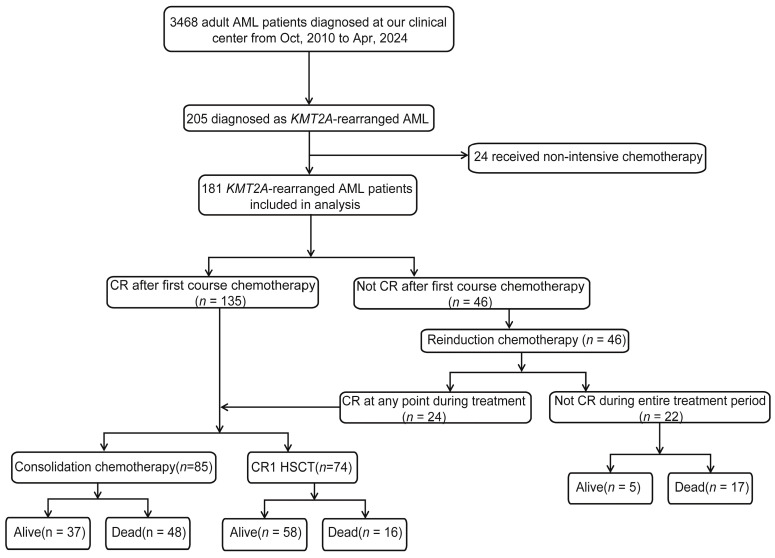 Figure 1
Figure 1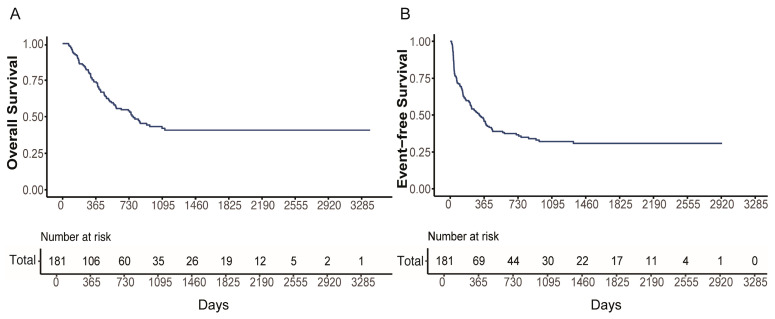 Figure 2
Figure 2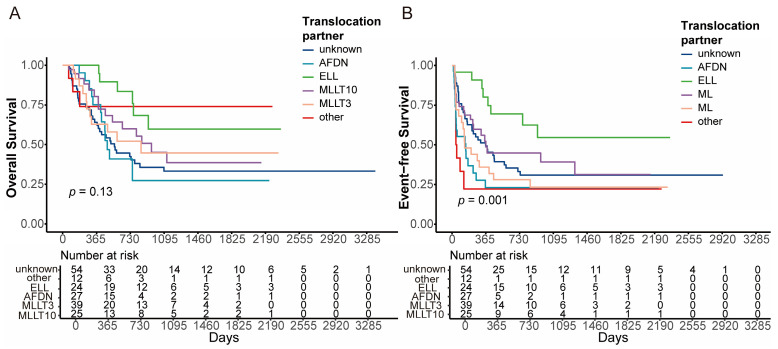 Figure 3
Figure 3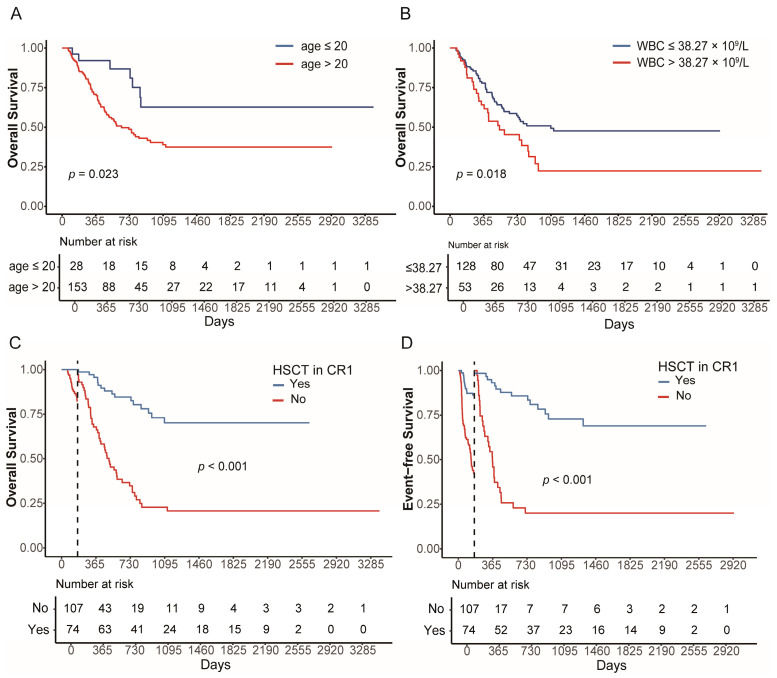 Figure 4
Figure 4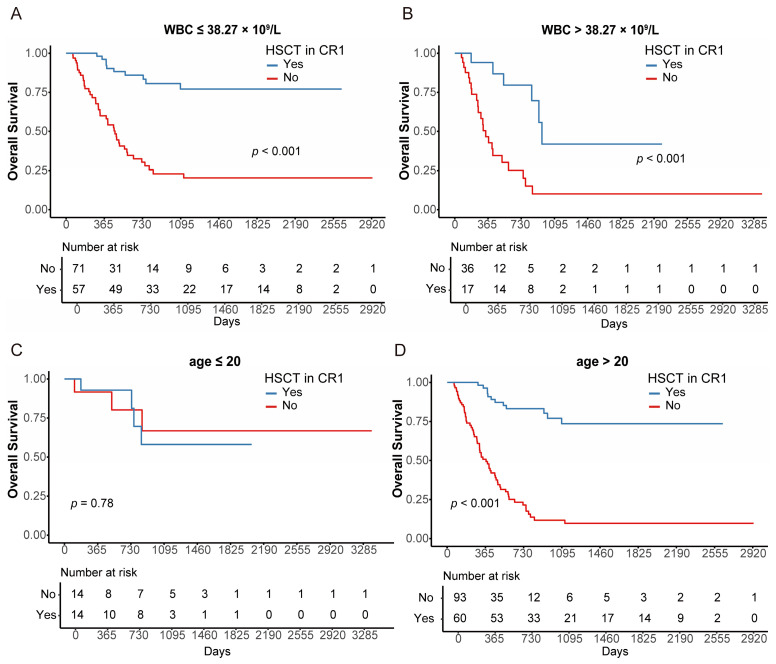 Figure 5
Figure 5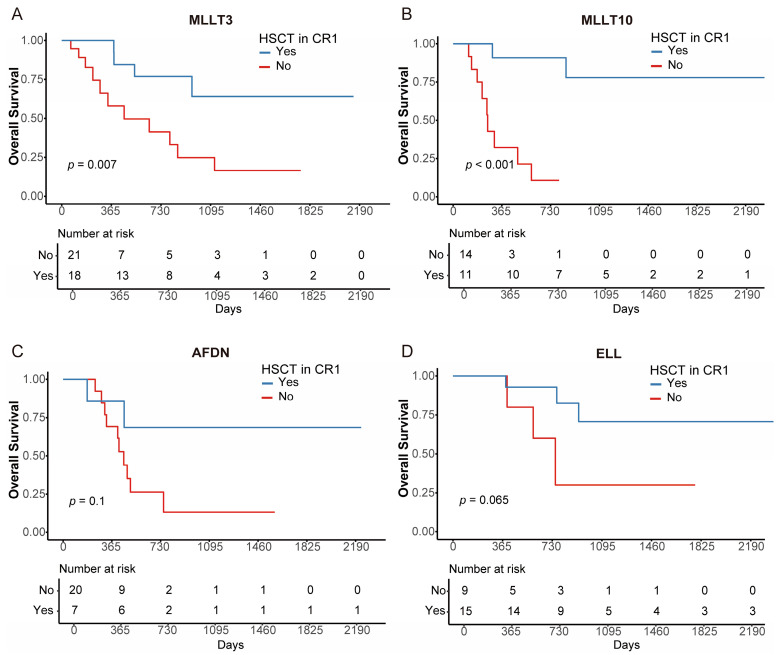 Figure 6
Figure 6- —National Key Research and Development Program of China
- —National Natural Science Foundation of China
- —CAMS Innovation Fund for Medical Sciences
- —Tian Jin Natural Science Foundation
- —Haihe Laboratory of Cell Ecosystem Innovation Fund
- —Beijing Xisike Clinical Oncology Research Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myeloid Leukemia Research · Genomics and Rare Diseases · Chronic Myeloid Leukemia Treatments
1. Background
Acute myeloid leukemia (AML), the most prevalent acute leukemia in adults, is stratified into different risk groups based on the 2022 European Leukemia Net (ELN) and National Comprehensive Cancer Network (NCCN) guidelines [1,2,3]. The KMT2A (lysine methyltransferase 2A) gene, also known as the MLL (mixed lineage leukemia) gene, is located in the 11q23.3 region of human chromosomes. KMT2A rearrangements are a reproducible genetic abnormality in acute myeloid leukemia (AML) [3,4,5,6]. To date, more than 130 different recombinations in MLL have been identified. AFF1, MLLT3, MLLT1, MLLT10, AFDN, and ELL were the most common fusion partners identified in KMT2A-rearranged AML, observed in over 90% of cases [7,8,9,10]. According to the ELN 2022 and NCCN guidelines, AML with KMT2A::MLLT3 is classified as intermediate-risk, while those with other KMT2A-rearranged subtypes are classified as adverse-risk [3,8].
While recent studies largely support the prognostic stratification proposed by the ELN 2022 guidelines, clinical outcomes for specific fusion partners remain heterogeneous, and the benefit of allogeneic HSCT across these diverse subgroups requires further investigation [11,12,13]. Previous studies have demonstrated that adult patients with KMT2A-rearranged AML could benefit from allogeneic hematopoietic stem cell transplantation (allo-HSCT) [14,15,16,17]. However, few studies have explored the potential benefit of HSCT for each KMT2A-rearrangement partner subgroup. Particularly in the era of emerging targeted therapies such as menin inhibitors, it is vital to understand the baseline benefit of HSCT in different subtypes to make precise therapeutic decisions.
Consequently, our study sought to investigate outcomes and potential factors influencing prognosis in AML patients with KMT2A rearrangements. Additionally, we conducted a subgroup analysis to identify populations of KMT2A-rearranged AML patients who might benefit from allo-HSCT for improved survival.
2. Methods
2.1. Patient Selection
We retrospectively assessed 3468 consecutive adolescent and adult patients with newly diagnosed AML treated at the Institute of Hematology and Blood Diseases Hospital of the Chinese Academy of Medical Sciences (Tianjin, China) between October 2010 and April 2024. The enrolled patients had to meet the following criteria: (1) diagnosed as KMT2A-rearranged AML through karyotype, Fluorescence In Situ Hybridization (FISH), Reverse Transcription Polymerase Chain Reaction (RT-PCR), or transcriptome sequencing; (2) receiving intensive chemotherapy. This study was approved by the Ethics Committee of the Institute of Hematology and Blood Diseases Hospital of the Chinese Academy of Medical Sciences (Tianjin, China) and conducted in accordance with the Declaration of Helsinki.
2.2. FISH, RT-PCR and NGS
Fluorescence in situ hybridization (FISH) was performed on bone marrow mononuclear cells by our clinical center laboratory. Split-signal assays were conducted using the Vysis LSI MLL Dual Color, Break Apart Rearrangement Probe (Abbott Molecular, Des Plaines, IL, USA) to detect 11q23/KMT2A gene rearrangements. The assay was performed according to the manufacturer’s instructions.
For RT-PCR, total RNA was extracted from bone marrow. Supplementary Table S1 lists the panel of fusion genes detected by RT-PCR, which were associated with hematologic malignancies. PCR amplification was performed as described previously [18,19].
All the targeted NGS data mentioned in this article was obtained from our clinical center. The targeted sequencing panel covered 267 common genes (Supplementary Table S2) in hematologic malignancies. The panel design was undertaken at the Clinical Testing Center of the Institute of Hematology and Blood Diseases Hospital (Tianjin, China), and the detailed protocol has been described previously [19,20]. The sequencing data was processed into vcf files with the reference genome hg19 at the Clinical Testing Center. ANNOVAR software (version: 8 Jun 2020. Center for Applied Genomics, Children’s Hospital of Philadelphia, Philadelphia, PA, USA) [21] was used for variant annotation. All mutation sites were filtered using Integrative Genomics Viewer (IGV, version: 2.15.1 Broad Institute, Cambridge, MA, USA) [22] to eliminate false positives.
2.3. Treatments
Enrolled patients received intensive induction therapy with one of the following regimens: (1) DA: Daunorubicin (60 mg/m^2^/day, IV, days 1–3) and cytarabine (100 mg/m^2^/day, IV, days 1–7); (2) HAD: Homoharringtonine (2 mg/m^2^/day, IV, days 1–7), daunorubicin (40 mg/m^2^/day, IV, days 1–3), and cytarabine (100 mg/m^2^/day, IV, days 1–7); and (3) DAV: Venetoclax was initiated with a 2-day ramp-up phase (100 mg and 200 mg) prior to chemotherapy, followed by 400 mg daily on days 1–7, in combination with daunorubicin (60 mg/m^2^/day, IV, days 1–3) and cytarabine (100 mg/m^2^/day, IV, days 1–7). As detailed in our previous studies [19,23], the therapeutic protocols were consistent with the standard of care at our center. Post-remission management was stratified based on transplant eligibility. For transplant-eligible patients, donor searching was initiated immediately. During the interval, patients received one or two courses of intermediate- or high-dose cytarabine as bridging therapy to sustain remission. HSCT was performed as soon as a donor became available. Patients precluded from HSCT due to donor unavailability or patient preference received standard consolidation chemotherapy for a total of 3 courses. Routine prophylaxis against central nervous system (CNS) leukemia was administered via intrathecal injection. The regimen consisted of methotrexate (10 mg), cytarabine (50 mg), and dexamethasone (10 mg) per dose. In general, two doses were administered during induction and each consolidation course, as described in our previous studies [18,19]. Supportive care regarding infection management was described in our previous studies [23]. Antifungal prophylaxis, such as posaconazole, voriconazole, or caspofungin, was administered based on the attending physician’s clinical experience and judgment. Routine antibacterial prophylaxis was not employed; instead, antibiotic treatment was administered upon the onset of symptoms, based on pathogenic microbiological examination and drug susceptibility results.
2.4. Statistical Analysis
Descriptive statistics were employed to outline patients’ baseline characteristics. Differences in baseline characteristics were assessed using the Chi-squared test or two-sided Fisher’s exact test for categorical variables and the Mann–Whitney U test for continuous variables. OS was defined as the interval from the date of diagnosis to death from any cause or the last follow-up. EFS was defined as the time from diagnosis to induction failure, relapse, death in CR, or last follow-up, whichever occurred first. The optimal cutoff values for continuous variables, including age and WBC count, were determined using the “surv_cutpoint” function in R. Landmark analysis was utilized to prevent bias introduced by patients who experienced early relapse or death before HSCT when analyzing the effect of HSCT. The landmark day was set as the median time from the date of first CR to HSCT. OS and EFS were evaluated by the Cox or Kaplan–Meier method and compared with the Log-rank test. HSCT was treated as a time-dependent variate in the Cox regression model. A p-value of less than 0.05 was deemed statistically significant. All statistical analyses were conducted using IBM SPSS version 26 (IBM Corp, Armonk, NY, USA) and R version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria).
3. Results
3.1. Patient Characteristics
The incidence of KMT2A-rearranged AML in our cohort with newly diagnosed AML was 5.9% (205/3468). Of the 205 identified KMT2A-rearranged patients, 24 patients were excluded from the final analysis as they received non-intensive chemotherapy including hypomethylating agents or palliative care. Consequently, a total of 181 patients who underwent intensive induction chemotherapy between 1 October 2010 and 1 April 2024 were included in this study. The screening process and criteria are shown in Figure 1. Among these 181 patients, 89 (49.2%) were male and 92 (50.8%) were female, with a median age of 33 (range 13–65) years. According to the partner genes of KMT2A fusions, 24 (13.3%) patients were ELL, 27 (14.9%) were AFDN, 39 (21.5%) were MLLT3, 25 (13.8%) were MLLT10, and 12 (6.6%) had other rare types of KMT2A rearrangement. The type of KMT2A rearrangements could not be determined in 54 (29.8%) patients, because their results were only available for FISH detection. The detailed distribution of these fusion partners is illustrated in Supplementary Figure S1. Genetic testing information via targeted NGS was evaluable in 128 patients from our cohort. The most common concomitant mutations included K-RAS (n = 41, 32.0%), N-RAS (n = 40, 31.3%), PTPN11 (n = 20, 15.6%) and FLT3 (n = 19, 14.8%). A total of 74 (40.9%) patients underwent HSCT following the first complete remission (CR1). Detailed clinical characteristics are shown in Table 1.
To assess whether baseline clinical characteristics were balanced among different KMT2A-rearrangement subtypes, we summarized in Supplementary Table S3. The ‘Unknown’ group (n = 54) was excluded due to missing mutation data for 39 patients. Age and gender distributions were balanced across the KMT2A::MLLT3, KMT2A::AFDN, KMT2A::MLLT10, KMT2A::ELL, and “other” groups. However, the initial WBC count in the KMT2A::AFDN group was significantly higher than other groups (p < 0.001). Notably, there was no significant difference in the distribution of intensive induction chemotherapy regimens among the subtypes (p = 0.330).
Of 181 patients, the median follow-up for survivors was 17.53 months (1.47–112.57), and the 3-year OS and EFS of the entire cohort were 42.0% (95% CI, 34.1–51.8%) and 32.1% (95% CI, 25.3–40.6%), respectively (Figure 2A,B).
3.2. Impact of KMT2A Rearrangement Subtypes on Outcomes
According to the partner genes of KMT2A rearrangement, the 3-year OS was 59.8% (95% CI, 38.7–92.3%), 27.3% (95% CI, 10.3–72.3%), 45.1% (95% CI, 28.7–71.0%), and 44.7% (95% CI, 26.7–74.9%) in the ELL (n = 24), AFDN (n = 27), MLLT3 (n = 39), and MLLT10 (n = 25) groups, respectively (global p = 0.130, Figure 3A). The 3-year EFS was 54.7% (95% CI, 35.0–85.4%), 23.0% (95% CI, 10.9–48.8%), 39.2% (95% CI, 24.6–62.7%) and 23.3% (95% CI, 11.3–48.1%) in the ELL, AFDN, MLLT3, and MLLT10 groups, respectively (global p = 0.001, Figure 3B). KMT2A::ELL was associated with better OS and EFS compared to those with other partner genes (OS, p = 0.023; EFS, p = 0.003, Supplementary Figure S2A,B). No significant differences in either OS or EFS were observed in the MLLT3 subgroup compared to the other groups (OS, p = 0.640; EFS, p = 0.430, Supplementary Figure S2C,D).
After setting HSCT as a censoring event, the 3-year OS and EFS for the entire cohort were 21.9% (95% CI, 13.5–35.3%) and 15.6% (95% CI, 8.7–28.2%), respectively (Supplementary Figure S3A,B). The 3-year OS was 30.0% (95% CI, 6.3–100.0%), 13.3% (95% CI, 2.5–71.4%), 18.9% (95% CI, 5.6–64.7%), and 11.9% (95% CI, 1.9–73.8%) in the ELL (n = 24), AFDN (n = 27), MLLT3 (n = 39), and MLLT10 (n = 25) groups, respectively (p = 0.27, Supplementary Figure S4A). The 3-year EFS was 25.7% (95% CI, 5.3–100.0%), not reach (NR), 19.8% (95% CI, 6.2–62.8%) and NR in the ELL, AFDN, MLLT3, and MLLT10 groups, respectively (p < 0.001, Supplementary Figure S4B). Patients with KMT2A::ELL demonstrated superior EFS and a trend towards OS compared with non-ELL subtypes (OS, p = 0.053; EFS, p = 0.001; Supplementary Figure S4C,D). KMT2A::MLLT3 still did not exhibit significant differences in OS or EFS when compared to other groups (OS, p = 0.470; EFS, p = 0.560; Supplementary Figure S4E,F).
3.3. Prognostic Factors for KMT2A-Rearranged AML
To exclude the potential confounding effect of historical advances in supportive care, we stratified the patients into two cohorts based on year of diagnosis: the earlier era (2010–2016) and the recent era (2017–2024). Patients diagnosed in the recent era exhibited significantly superior OS compared to those in the earlier era (3-year OS: 33.2% [95%CI, 23.0–48.1%] vs. 48.1% [95%CI, 37.4–62.0%], p = 0.045, Supplementary Figure S5A). However, no significant difference was observed in EFS between the two eras (3-year EFS: 29.8% [95%CI, 20.0–44.4%] vs. 33.5% [95%CI, 24.8–45.3%], p = 1.000, Supplementary Figure S5B).
We further performed univariate Cox analysis to explore other prognostic factors, including year of diagnosis and co-mutations (Supplementary Table S4). Regarding the year of diagnosis, patients treated in the recent era (2017–2024) showed superior OS compared to the earlier era (HR = 0.641, 95% CI 0.414–0.994, p = 0.047), whereas no significant association was observed with EFS (HR = 0.999, 95% CI 0.687–1.474, p = 0.998). Notably, the five most frequently mutated genes, including KRAS, NRAS, PTPN11, FLT3, and WT1, were not significantly associated with OS or EFS. Age and initial WBC were significant prognostic factors for both OS and EFS (Age: OS, HR = 1.020, 95% CI 1.000–1.043, p = 0.045; EFS, HR = 1.021, 95% CI, 1.004–1.038, p = 0.013; WBC: OS, HR = 1.003, 95% CI 1.000–1.007, p = 0.050; EFS, HR = 1.005, 95% CI, 1.002–1.008, p = 0.001). Setting KMT2A::ELL as a reference, univariate analysis confirmed its favorable prognostic role. The KMT2A::AFDN subgroup exhibited the poorest outcomes, with a significantly increased risk for both OS (HR = 2.926, 95% CI 1.093–7.831, p = 0.033) and EFS (HR = 4.322, 95% CI 1.884–9.916, p = 0.001). The KMT2A::MLLT10 subgroups also showed significantly inferior EFS (HR = 3.310, 95% CI 1.448–7.569, p = 0.005), whereas no significant difference was observed in OS (HR = 2.275, 95% CI 0.841–6.155, p = 0.106). While the outcome of KMT2A::MLLT3 was comparable to KMT2A::ELL (OS, HR = 2.039, 95% CI 0.791–5.259, p = 0.141; EFS, HR = 2.188, 95% CI, 0.969–4.944, p = 0.060).
We used the “surv_cutpoint” function in R to identify the optimal cutoff value for age and WBC. Consequently, we divided the cohort into two groups: age > 20 (n = 153) and age ≤ 20 (n = 28). Significant differences in OS were identified between the two groups, with 3-year OS of 38.9% (95% CI, 30.5–49.5%) and 62.6% (95% CI, 43.7–89.9%), respectively (Figure 4A). Similarly, we divided the cohort into two groups according to WBC: WBC > 38.27 × 10^9^/L (n = 53) and WBC ≤ 38.27 × 10^9^/L (n = 128). The 3-year OS of the two groups was 22.4% (95% CI, 11.3–44.4%) and 47.7% (95% CI, 38.4–59.3%), respectively (Figure 4B). Concomitant mutations did not have a significant impact on the prognosis of KMT2A-rearranged AML patients. No significant differences were observed in baseline clinical characteristics between transplanted and non-transplanted patients (Table 1). The time-dependent univariate Cox analysis indicated that HSCT in CR1 significantly improved OS and EFS (OS: HR = 0.221, 95% CI 0.125–0.391, p < 0.001; EFS: HR = 0.194, 95% CI, 0.101–0.371, p < 0.001). The landmark day was set as the median time from the date of first CR to HSCT. Landmark analysis also showed that HSCT significantly improved OS and EFS in KMT2A-rearranged AML patients (OS: p < 0.001; EFS: p < 0.001, Figure 4C,D).
Finally, we included age, WBC, KMT2A-rearrangement subtype, the year of diagnosis and HSCT in CR1 in the multivariate analysis. Notably, the multivariate analysis indicated that the year of diagnosis was not independently associated with either OS (HR = 0.660, 95% CI 0.392–1.192, p = 0.118) or EFS (HR = 1.036, 95% CI 0.659–1.629, p = 0.878). The results indicated that age and HSCT in CR1 were independently associated with OS and EFS (OS: HR = 1.022, 95% CI 1.002–1.042, p = 0.029 [age]; HR = 0.233, 95% CI 0.129–0.422, p < 0.001 [HSCT in CR1]; EFS: HR = 1.027, 95% CI 1.010–1.044, p = 0.002 [age]; HR = 0.155, 95% CI 0.078–0.308, p < 0.001 [HSCT in CR1], Supplementary Table S4).
3.4. The Impact of HSCT in Subgroups of KMT2A-Rearranged AML
To identify which patients would benefit from HSCT, we performed a subgroup analysis. We found that both patients with WBC > 38.27 × 10^9^/L and WBC ≤ 38.27 × 10^9^/L could significantly benefit from HSCT (both p < 0.001; Figure 5A,B). In addition, patients aged > 20 years were more likely to benefit from HSCT than those aged ≤ 20 years (p < 0.001 [age > 20], p = 0.780 [age ≤ 20]; Figure 5C,D). Regarding KMT2A-rearranged subtypes, significant advantages were observed in the MLLT3 and MLLT10 groups, with a trend in ELL and AFDN groups (HSCT vs. non-HSCT (3-year OS [95% CI]): 64.1% [40.2–100%] vs. 24.8% [9.4–65.6%], p = 0.007 [MLLT3]; 77.9% [54.6–100%] vs. 10.7% [1.7–67.7%], p < 0.001 [MLLT10]; 70.7% [47.1–100%] vs. 30.0% [6.31–100%], p = 0.065 [ELL]; 68.6% [40.3–100%] vs. 13.2% [2.45–71.1%], p = 0.1 [AFDN], Figure 6A–D).
4. Discussion
Our study presents a retrospective analysis of 181 patients with KMT2A-rearranged AML treated with intensive chemotherapy. We assessed the prognostic impact of heterogeneity within KMT2A rearrangements and investigated the survival benefit conferred by allo-HSCT. The outcomes of KMT2A-rearranged AML were dismal and were influenced by partner genes. HSCT in CR1 improved outcomes; however, the magnitude of benefit varied across patient age groups.
Our study underscores the significant influence of KMT2A rearrangement partner genes on survival outcomes in AML [24,25,26]. In line with prior literature, patients harboring KMT2A::AFDN and KMT2A::MLLT10 fusions exhibited the poorest survival in our cohort [13,15,27], and we found better outcomes in the KMT2A::ELL compared with other KMT2A-rearranged subtypes. Conflicting results were reported for the outcomes of KMT2A::ELL AML. Chen et al. demonstrated that KMT2A::ELL patients exhibited significantly lower 5-year OS and EFS (both 6%) [28]. Tamai et al. demonstrated the unfavorable prognosis of t (11;19) patients, with 1-year EFS of 12.8% and 2-year OS of 10.7% [29]. Conversely, some studies indicate a more favorable prognosis for KMT2A::ELL AML. Grimwade et al. have reported that KMT2A::ELL and KMT2A::MLLT3 patients have an OS comparable to those with normal karyotype AML [13]. Wu et al. reported the best OS for KMT2A::ELL than other subtypes [30]. Recently, Zhang et al. reported that the KMT2A::ELL subgroup exhibited a better OS (3-year OS, 65.3%), although there was no statistically significant difference compared to other KMT2A-rearranged subtypes [31].
The survival outcomes of KMT2A::MLLT3 patients in our cohort were comparable to those of other KMT2A-rearranged AML patients, although several studies have demonstrated that KMT2A::MLLT3 exhibited better survival than other subtypes. The survival outcomes of KMT2A::MLLT3 patients in our cohort aligned with previous studies, showing 3-year OS ranging from 35% to 45% [13,24,25,26,28]. In early reports from the Cancer and Leukemia Group B (CALGB), patients with KMT2A::MLLT3 displayed significantly superior EFS compared to those with other KMT2A-rearranged subtypes [12]. The most recent report from CALGB showed that patients under 60 years showed a significantly improved 3-year OS in the KMT2A::MLLT3 group than other subtypes (41% vs. 16%, p = 0.004) [25]. A study by Issa et al. reported a more favorable prognosis for the KMT2A::MLLT3 subgroup, with 5-year OS of 28%, although this difference did not reach statistical significance [26].
Early investigations have revealed that allo-HSCT in CR1 conferred a significant survival advantage for KMT2A-rearranged AML patients [28,32,33], and a recent study by Zhang et al. reported a notable survival advantage for KMT2A-rearranged AML patients who underwent HSCT, with OS of 77.3% compared to 31.7% in those receiving conventional chemotherapy (p < 0.001) [31]. However, Tamai et al. previously indicated that allo-HSCT in CR1 did not confer a substantial advantage in terms of disease-free survival (DFS) or OS for KMT2A-rearranged AML patients younger than 60 years [29]. These findings collectively highlight the need for further data on HSCT outcomes in relation to KMT2A-rearranged AML patients.
We explored the effects of HSCT across various KMT2A-rearranged subtypes. Our findings suggest that while the magnitude of benefit from HSCT may differ among distinct KMT2A-rearranged subtypes, HSCT in CR1 should generally be considered for all KMT2A-rearranged AML patients, regardless of the specific KMT2A fusion type. Specifically, our results support allo-HSCT for KMT2A::MLLT3 patients. This recommendation is also supported by a recent report from Bataller et al., which demonstrated a significantly improved 2-year overall survival (OS) of 67% for KMT2A::MLLT3 patients who underwent HSCT in CR1 [34], aligning with our observed survival outcomes. Additionally, our data indicated that KMT2A-rearranged patients aged 20 years or younger did not experience a significant survival advantage from HSCT. This finding challenges the assumption of HSCT benefit in KMT2A-rearranged AML, suggesting reduced transplant demand in younger patients with these genetic alterations. Our data advocate precision treatment strategy integrating genetic and clinical characteristics within this genetically diverse disease.
Since our study spanned 14 years, we examined the year of diagnosis to rule out any historical bias. We observed a significant improvement in OS for patients treated in the recent era (2017–2024) compared to the earlier era (2010–2016). This improvement likely reflects advances in supportive care and transplant techniques. To rule out potential bias, we included the year of diagnosis in our univariate and multivariate analyses. Although the year of diagnosis was significant for OS in the univariate analysis, this significance disappeared in the multivariate model for both OS and EFS. Additionally, in our KMT2A-rearranged cohort, there was no significant difference in the distribution of patients receiving different induction regimens across the various fusion partner subgroups. Therefore, we consider that the specific induction regimen did not significantly influence the survival outcomes in our survival analyses. This confirms that the survival differences among KMT2A subtypes are driven by the specific fusion partners, rather than by historical changes in treatment.
Furthermore, when comparing our results with cited historical cohorts, such as the research of CALGB and Grimwade et al. [12,13], several variations warrant consideration. Firstly, regarding analytical methods and sample size, our study utilized standard statistical techniques such as Kaplan–Meier and cox regression consistent with the cited literature [12,13,24,25,26,27,28,29,30,31]. Compared to referenced studies where KMT2A-rearranged cohorts typically ranged from 47 to 180 patients [12,13,24,25,26], our cohort (n = 181) represents a relatively large sample size with sufficient statistical power to yield robust prognostic insights. Secondly, regarding treatment heterogeneity, our cohort incorporated HHT-based induction (HAD regimen), which differs from the standard ‘7 + 3’ regimens typically used in Western cohorts [24,25,26,27]. While our internal analysis confirmed no significant survival difference between HAD and DA regimens in our cohort, these protocol variations preclude a direct head-to-head comparison of absolute survival rates. Thirdly, regarding follow-up duration, while some referenced studies reported 5-year outcomes, our study focused on 3-year OS and EFS. Given that KMT2A-rearranged AML is characterized by aggressive disease kinetics and early relapse [26,28,29], we consider our 3-year metrics sufficiently mature to capture the critical prognostic events and reflect the long-term survival trends. Despite these differences in sample sizes, therapeutic baselines, and analytical timepoints, the prognostic hierarchy of fusion partners observed in our cohort aligns with major international reports [30,31], underscoring that intrinsic biological characteristics are the principal driver of clinical outcomes.
Several limitations of our study should be acknowledged. Firstly, specific fusion partners could not be identified in 29.8% of patients, and NGS data were available for 70.7% (128/181) of the cohort due to the retrospective nature of the study. Secondly, a substantial proportion of patients could not be assigned to specific KMT2A rearrangement subtypes due to the limitations of FISH testing, potentially limiting the ability to detect subtype-specific differences. Thirdly, the relatively small sample sizes within certain subtype groups may have restricted the statistical power to detect subtle differences in survival outcomes. Fourthly, specific data on co-morbidities were not available for all patients; however, all included patients were deemed fit for intensive chemotherapy, suggesting a generally adequate performance status.
5. Conclusions
Our study provides additional evidence of the clinical heterogeneity of KMT2A-rearranged AML and highlights the critical role of subtyping in risk stratification and therapeutic decision-making. HSCT in CR1 significantly improved outcomes across different KMT2A fusion subtypes; however, the magnitude of benefit varied across patient age and subtypes. This clinical cohort study delineates treatment efficacy and survival outcomes in KMT2A-rearranged AML patients receiving intensive chemotherapy and HSCT, providing an evidence base for optimizing therapeutic strategies. Recent studies have identified menin inhibitors as a promising novel therapeutic approach for KMT2A-rearranged leukemia, offering a new option for patients with suboptimal responses to conventional therapies [35,36]. Future research should focus on elucidating the specific molecular mechanisms underlying the observed subtype-specific differences in survival, as well as exploring novel therapeutic strategies to improve outcomes for patients with KMT2A-rearranged AML.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Becker M.M. Farina K.A. Mascarenhas J. Acute myeloid leukemia: Current understanding and management J. Am. Acad. Physician Assist.202437343910.1097/01.JAA.0000995680.52352.b 538128137 · doi ↗ · pubmed ↗
- 2Pollyea D.A. Bixby D. Perl A. Bhatt V.R. Altman J.K. Appelbaum F.R. de Lima M. Fathi A.T. Foran J.M. Gojo I. NCCN Guidelines Insights: Acute Myeloid Leukemia, Version 2.2021 J. Natl. Compr. Cancer Netw.202119162710.6004/jnccn.2021.000233406488 · doi ↗ · pubmed ↗
- 3Döhner H. Wei A.H. Appelbaum F.R. Craddock C. Di Nardo C.D. Dombret H. Ebert B.L. Fenaux P. Godley L.A. Hasserjian R.P. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN Blood 20221401345137710.1182/blood.202201686735797463 · doi ↗ · pubmed ↗
- 4Khoury J.D. Solary E. Abla O. Akkari Y. Alaggio R. Apperley J.F. Bejar R. Berti E. Busque L. Chan J.K.C. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms Leukemia 2022361703171910.1038/s 41375-022-01613-135732831 PMC 9252913 · doi ↗ · pubmed ↗
- 5Super H.J. Mc Cabe N.R. Thirman M.J. A Larson R. Le Beau M.M. Pedersen-Bjergaard J. Philip P. O Diaz M. Rowley J.D. Rearrangements of the MLL gene in therapy-related acute myeloid leukemia in patients previously treated with agents targeting DNA-topoisomerase II Blood 1993823705371110.1182/blood.V 82.12.3705.37058260707 · doi ↗ · pubmed ↗
- 6Bloomfield C.D. Archer K.J. Mrózek K. Lillington D.M. Kaneko Y. Head D.R. Cin P.D. Raimondi S.C. 11q 23 balanced chromosome aberrations in treatment-related myelodysplastic syndromes and acute leukemia: Report from an International Workshop Genes Chromosom. Cancer 20023336237810.1002/gcc.1004611921271 · doi ↗ · pubmed ↗
- 7Huang J. Zhu Y. Li J. Yang G. Zhang S. The KMT 2A rearrangement is an early event prior to KMT 2A-PTD in AML patients with both molecular aberrations Ann. Hematol.202210249549710.1007/s 00277-022-05074-536525029 · doi ↗ · pubmed ↗
- 8Meyer C. Burmeister T. Gröger D. Tsaur G. Fechina L. Renneville A. Sutton R. Venn N.C. Emerenciano M. Pombo-De-Oliveira M.S. The MLL recombinome of acute leukemias in 2017 Leukemia 20183227328410.1038/leu.2017.21328701730 PMC 5808070 · doi ↗ · pubmed ↗