Hodgkin Lymphoma—The Effect of Chemotherapy on Gonadal Function and Fertility Is Strongly Related to the Treatment Regimen, Age, and Sex: A Systematic Review and Meta-Analysis
Mareike Roth-Hochreutener, Maria Karakitsiou, Angela Vidal, Susanna Weidlinger, Janna Pape, Tanya Karrer, Karolin Behringer, Michael von Wolff

TL;DR
This study shows that chemotherapy for Hodgkin lymphoma affects fertility differently based on treatment type, age, and sex, guiding personalized fertility counseling.
Contribution
The paper provides the first comprehensive meta-analysis of chemotherapy-induced infertility in Hodgkin lymphoma patients, stratified by regimen, age, and sex.
Findings
Presumed infertility rates are 21% in women and 45% in men after Hodgkin lymphoma chemotherapy.
Regimens like BEACOPP have high infertility risks (38% in women, 81% in men), while ABVD has much lower risks (6% in both sexes).
Male adolescents treated for Hodgkin lymphoma face particularly high infertility risks (67%).
Abstract
Hodgkin lymphoma (HL) mainly affects people during their reproductive years, making fertility an important part of survivorship. Although cure rates are high, chemotherapy can impair gonadal function, with the extent of damage depending on the specific regimens used, as well as on age and sex. To provide clearer, evidence-based counselling, we systematically reviewed studies published since 2000 and combined data from more than 7000 patients. Overall, the likelihood of presumed infertility after treatment was approximately 21% in adult women and 45% in adult men. Infertility risk varies widely by regimen: it is low after ABVD but substantially higher after regimens containing alkylating agents. Men are generally at greater risk than women, and boys treated during childhood/adolescence show particularly high vulnerability. These findings highlight the importance of personalized fertility…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
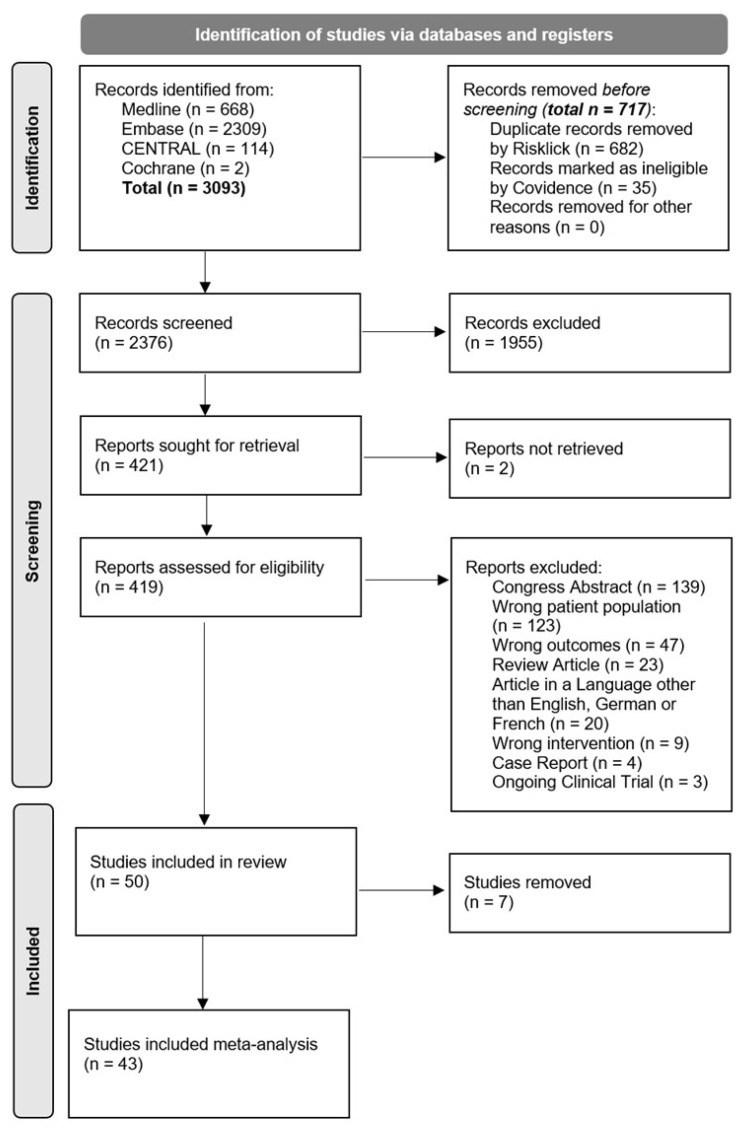 Figure 1
Figure 1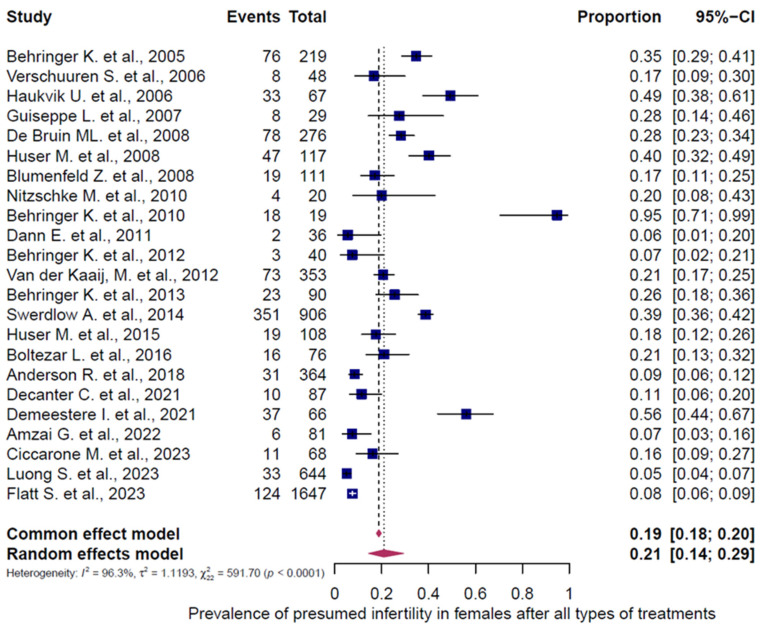 Figure 2
Figure 2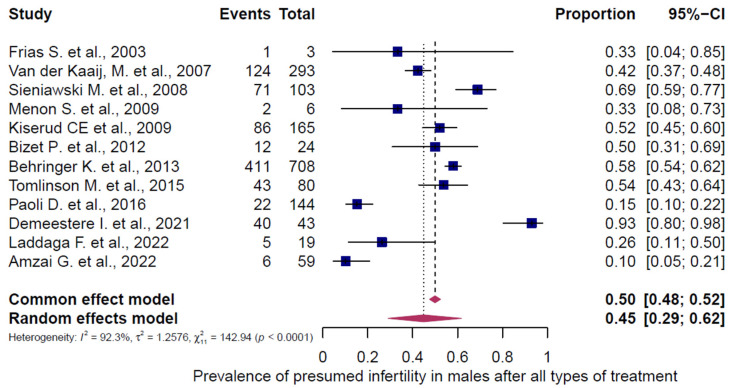 Figure 3
Figure 3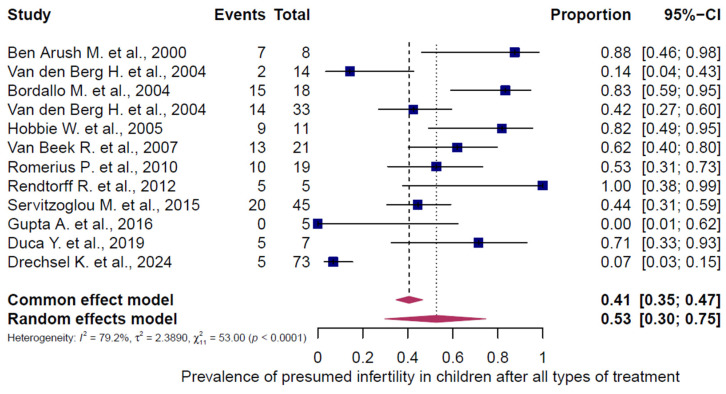 Figure 4
Figure 4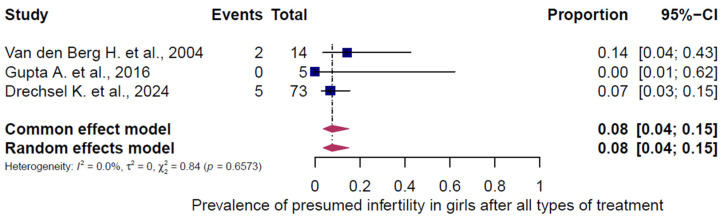 Figure 5
Figure 5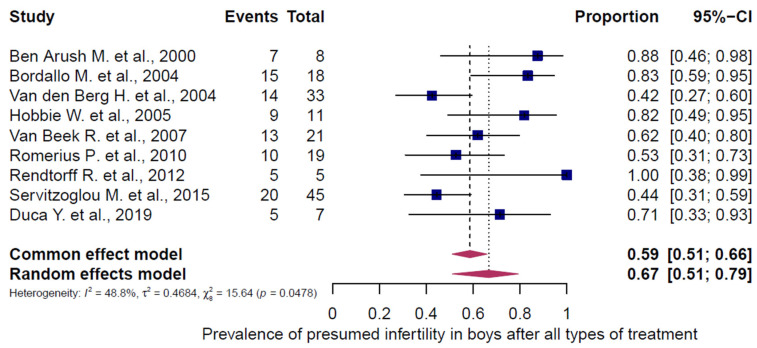 Figure 6
Figure 6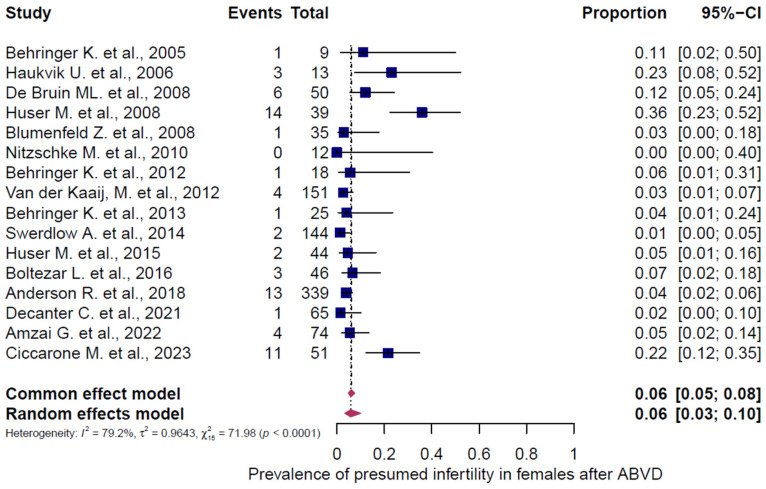 Figure 7
Figure 7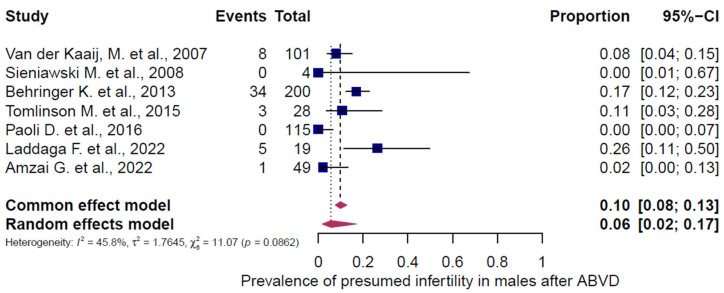 Figure 8
Figure 8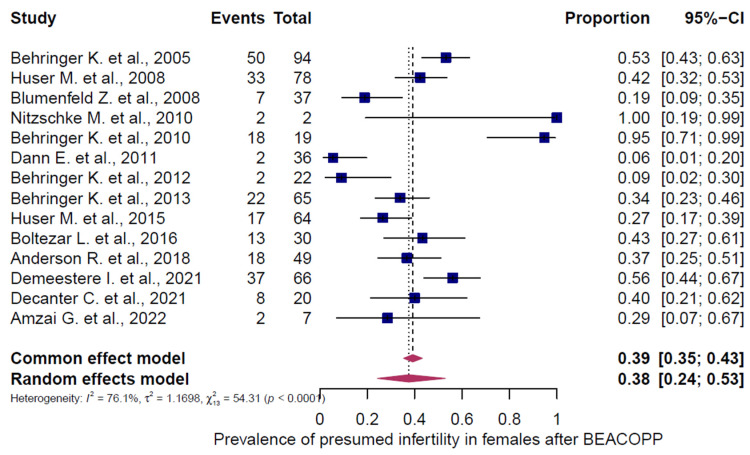 Figure 9
Figure 9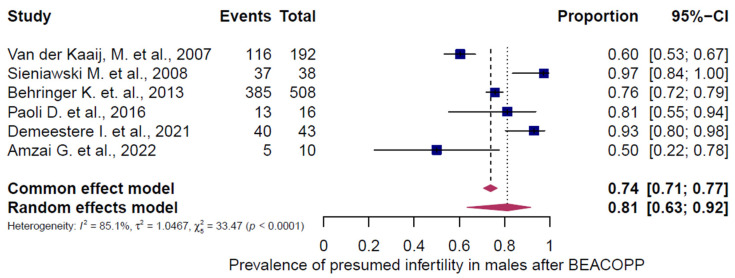 Figure 10
Figure 10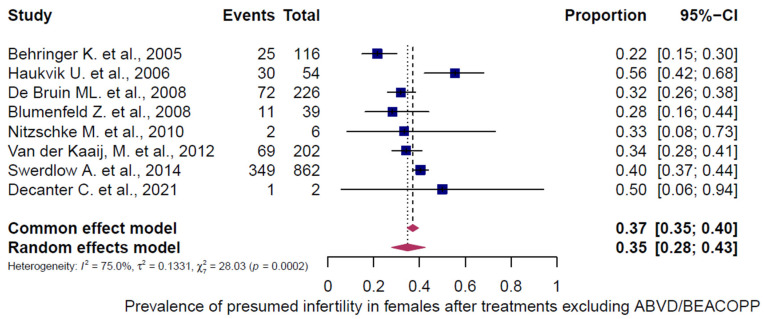 Figure 11
Figure 11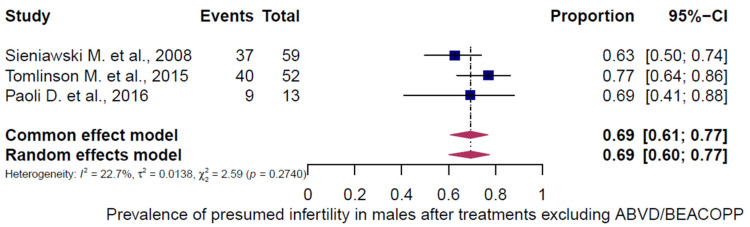 Figure 12
Figure 12| First Author, Year of Publication | Country | Study Design | Number of Participants of Interest (Females, Adults) | Age of Participants of Interest at Diagnosis/Therapy | Age (Years, Mean +/− SD) at Outcome/ | Follow-Up After Treatment, Length in Years (Range) | Tumor Type | Chemotherapy, Details | Infertility as Assumed | Infertility Parameter | Comments |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Behringer et al. 2005 [ | Germany | Retrospective | 219 | 16–40 | Not specified | 3.2 (0.58–6.3) | HL, | HD7: Arm A: no chemotherapy (excluded), Arm B: ABVD; | 76/219 (34.7%) *, 1/9 (11.1%) ▲, 25/116 (21.6%) ◦, 50/94 (53.2%) □ | * Calculated in women with secondary amenorrhea, all chemotherapy regimens; ▲ ABVD; ◦ other chemotherapies (COPP/ABVD); □ BEACOPP | |
| Verschuuren et al. 2006 [ | The Netherlands | Retrospective | 48 | 27 (18–44) | Not specified | 10 (1.1–15) | HL, | ABVD, EBVP, MOPP/ABV, BEACOPP | 8/48 (16.7%) * | * Calculated in women with POF (no spontaneous menstrual cycle within 5 years after antitumor treatment), all chemotherapy regimens | |
| Haukvik et al. 2006 [ | Norway | Retrospective | 67 | Complete cohort (N = 99 patients; N = 67 with chemotherapy, N = 32 without chemotherapy): POF-group: 27 (17–39), Non-POF-group: 25 (9–39) | 44 | 20 (10–25) | HL, Ann arbor stage I: 18.7%, stage II: 47.7%, stage III: 22.4%, stage IV: 11.2% | ABOD or EBVP (no alkylants): 19.4%, MVPP or ChlVPP (alkylants): 80.6% | 33/67 (49.3%) *, 3/13 (23.1%) ▲, 30/54 (55.6%) ◦ | * Calculated in women with POF (amenorrhea < 41 years, after other possible causes for amenorrhea have been excluded; no FSH values available), all chemotherapy regimens; ▲ ABVD; ◦ other regimens (MVPP, ChlVPP) | |
| Giuseppe et al. 2007 [ | Italy | Prospective | 29 | 24.3 (+/−SD 6.6) | 28.5 (± SD 7.3); <30 years: 69%, 30–36 years: 17.2%, | 4.2 (+/−SD 2.8) | HL, | MOPP/ABVD (44.8%), | 8/29 (27.6%) * | * Calculated in women with amenorrhea, all chemotherapy regimens | Co-treatment with GnRH-a: 14/29 (48%): all with amenorrhea in non-GnRH-a group; no significant difference in hormonal values (AMH, FSH, LH, Inhibin B) between GnRH-a/no GnRH-group |
| Huser et al. 2008 [ | Czech Republic | Prospective with historical controls | 117 | 30.4 (18–35) | Not specified | 0.5–1 | Newly diagnosed HL | Group A: ABVD, Group B: ABVD+ | 47/117 (40.2%) * 14/39 (35.9%) ▲ 33/78 (42.3%) □ | * Calculated in women with POF (FSH > 15 IU/L and no regular bleeding, 1 year after end of treatment), all chemotherapy regimens, | Case group (N = 72): Chemotherapy plus GnRH analogues; Control group (N = 45): same chemotherapy protocol but without GnRH analogues; POF rate in case group: 20.8%, POF rate in control group: 71.1% |
| Blumenfeld et al. 2008 [ | Israel | Prospective | 111 | GnRH-a/Chemotherapy group: 23.96 (SD +/− 5.47); Chemotherapy only group: 25.46 (SD +/− 6.41) | Not specified | 8 (2–15) | Classical HL, mostly stages II–III | ABVD, BEACOPP, MOPP-ABV(D) | 19/111 (17.1%) *, 1/35 (2.9%) ▲, 7/37 (18.9%) □, 11/39 (28.2%) ◦ | * Calculated in women with POF (hypergonadotropic amenorrhea: FSH > 40 U/L on at least 2 occasions and low E2 levels), all chemotherapy regimens; ▲ ABVD, □ BEACOPP, | Pregnancies (spontaneous conception): GnRHa-/CT group: N = 26, CT only group: N = 20, all healthy neonates, no congenital anomalies; POF incidence was significantly lower in the GnRHa group than in the chemotherapy-only group |
| De Bruin et al. 2008 [ | The Netherlands | Retrospective | 276 | Complete cohort (N = 518): 25 (14–39); Subdivision in age groups: 14–21: 33.2%; | Not specified | 9.4 | HL, | ABVD, EBVP, others (MOPP, MOPP/ABV) | 78/276 (28.3%) *, 6/50 (12%) ▲, 72/226 (31.9%) ◦ | * Calculated in women with premature menopause (cessation of menses < age 40 years), all chemotherapy regimens; ▲ ABVD + EBVP; ◦ other therapies (MOPP, MOPP/ABV) | |
| Nitzschke et al. 2009 [ | Switzerland | Cross-sectional | 20 | Not specified | 25.1 (17–35) | Group A: 2.55 (1.55–3.75), Group B: 2.68 (0.5–4.83) | HL, | ABVD, BEACOPP-14/s, OPPA + COPP/s | 4/20 (20%) *, | * Calculated in women with amenorrhea, FSH > 10 U/L and/or AMH not detectable, all chemotherapy regimens, ▲ ABVD, □ BEACOPP, | No significant difference between Group A and B (GnRHa use or not) in terms of AMH, Inhibin B, FSH, and amenorrhea |
| Behringer et al. 2010 [ | Germany | Prospective | 19 | 25.6 (18–40) | Not specified | 1.52 (1.04–2.78) | Advanced stage HL with risk factors | BEACOPPesc | 18/19 (94.7%) * | * Calculated in women with AMH not detectable, FSH > 10 U/L or amenorrhea 12 months after the end of treatment | Random assignment to receive daily oral contraception (OC) or GnRH-a; Study closed prematurely due to no protection of the ovarian reserve with hormonal co-treatment (OC or GnRHa) during BEACOPPesc |
| Dann et al. 2011 [ | Israel | Prospective | 36 | 27 (18–37) | Not specified | 7.42 (0.42–12) | Classical HL with adverse prognostic factors; | Escalated BEACOPP or standard BEACOPP | 2/36 (5.6%) * | * Calculated in women with POF | Two patients with POF treated with GnRH-analogues (triptorelin); patient 1: stBEACOPP × 6; patient 2: stBEACOPP × 2 + eBEACOPP × 4 |
| Behringer et al. 2012 [ | Germany | Prospective | 40 | 18–29 | Not specified | HD-14 Arm A: 3.5 +/− SD 1.67 (1–6.92); | HL, | HD-14 Arm A: ABVD; | 3/40 (7.5%) *, 1/18 (5.6%) ▲, 2/22 (9.1%) □ | * Calculated in women with FSH > 10 U/L, all chemotherapy regimens; | Pregnancies: HD-14 Arm A: 13%, HD-14 Arm B: 22%; |
| Van der Kaaij et al. 2012 [ | The Netherlands | Retrospective | 353 | 15–39 | Not specified for POI evaluation group; | 15 (5–45) | HL, | Nonalkylating agents: ABVD, EBVP; | 73/353 (20.7%) *, 4/151 (2.6%) ▲, 69/202 (34.2%) ◦ | * Calculated in women with POF (defined as menopause before age of 40 years), all chemotherapy regimens; ▲ ABVD + EBVP; ◦ MOPP, MOPP/ABV, stBEACOPP | Live births: Women with POF: 22% with ≥1 children after treatment (age at treatment: n = 9: <25 years; N = 8 25–32 years; Women without POF: 41% with ≥1 children |
| Behringer et al. 2013 [ | Germany | Prospective | 90 | Complete cohort: 28 +/− SD 7 (18–39), | Complete cohort: 32 +/− SD 7 (20–45) | 3.8 (1–8) | HL, | HD 13: ABVD or AVD; | 23/90 (25.6%) *, 1/25 (4%) ▲, 22/65 (33.8%) □ | * Calculated in women with FSH > 10 U/L and without hormonal contraception at the time of the study, all chemotherapy regimens; | Birth rates: HD13: 7% (1/15), HD14 Arm A: 14% (6/43), HD14 Arm B: 13% (6/48), HD15 Arm A: 5% (2/38), Arm B: 12% (3/26), Arm C: 4% (1/27) |
| Swerdlow et al. 2014 [ | United Kingdom | Retrospective | 906 | Not specified, Study inclusion criteria: Age < 36 years, Age at first treatment: | Not specified | 17.8 (0.3–48.4) | HL | ABVD, ChlVPP, LOPP, MVPP, MOPP | 351/906 (38.7%) *, | * Calculated in women with menopause < 40 years, all chemotherapy regimens, no or <10% with pelvic radiotherapy (RT); ▲ ABVD, no pelvic RT; ◦ other regimens (alkylants, ChlVPP, LOPP, MVPP, MOPP) with no or <10% pelvic RT | |
| Huser et al. 2015 [ | Czech Republic | Prospective | 108 | 27 (18–40) | Not specified | 1–2 | HL, Group A: Ann-Arbor Stage IA, IB, IIA or IIB without GHSG risk factors; Group B: Stages IA, IB, IIA or IIB with ≥1 GHSG risk factors; Group C: advanced HL (Stages III and IV or stage IIB with extranodal disease or large mediastinal mass) | Group A: ABVD; Group B: ABVD + BEACOPP (2 + 2); | 19/108 (17.6%) *, 2/44 (4.5%) ▲, 17/64 (26.6%) □ | * Calculated in women with FSH ≥ 15 IU/L (defined as chDOR (chemotherapy induced diminished ovarian reserve) according to the study, one year after the end of chemotherapy, all chemotherapy regimens; ▲ ABVD; □ BEACOPP | Monthly triptorelin i.m. for all patients; Pregnancy achievement: within 2 years follow-up N = 23 (21.3%); no protection of the ovarian follicle pool with GnRH-a treated with regimen C (escBEACOPP) in this study |
| Boltezar et al. 2016 [ | Slovenia | Retrospective | 76 | ABVD group: 26 (18–39), BEACOPP group: 26.5 (20–36) | Not specified | 9 (2–16) | HL, | ABVD, BEACOPP | 16/76 (21.1%) *, 3/46 (6.5%) ▲, 13/30 (43.3%) □ | * Calculated in women with secondary amenorrhea, all chemotherapy regimens; ▲ ABVD; □ BEACOPP | Number of patients attempting conception post-treatment: ABVD group: 91.3%, BEACOPP group: 86.7%; Having children after treatment: ABVD: 45.2%, BEACOPP: 34.6%, |
| Anderson et al. 2018 [ | United Kingdom | Prospective | 364 | ABVD-group: 26 (19–44), BEACOPP group: 31 (19–43) | Not specified | AMH measurements: 1–3; | Classical HL, stages IIB-IV or IIA with adverse features | ABVD-AVD, BEACOPP | 31/364 (8.5%) *, 13/339 (3.8%) ▲, 18/49 (36.7%) □ | * Calculated in women with AMH not detectable and/or FSH > 25 U/L, all chemotherapy regimens; | |
| Demeestere et al. 2021 [ | Belgium, France | Prospective | 66 | Standard group: 25 (P25–P75: 22–31), Study group: 27 (P25–P75: 22–31) | Not specified | Checkup (hormones, sperm analyses) at baseline, end of treatment, and every year during 5 years of follow-up | HL, | All patients: BEACOPPesc (2 cycles), Standard arm: additional BEACOPPesc (2 cycles), Study arm: if PET was negative: additional ABVD, if PET was positive: additional BEACOPPesc (2 cycles) | 37/66 (56.1%) * | * Calculated in women with AMH not detectable, 10–14 months after end of treatment, all chemotherapy regimens | Pregnancy rates: no significant differences between study and standard group |
| Decanter et al. 2021 [ | France | Prospective | 87 | Complete cohort (N = 122) with HL and non-HL, subdivision in AYA (adolescent and young adult) and Non-AYA; | Not specified | Serial AMH measurements from baseline up to 24 months after end of treatment | HL | ABVD, | 10/87 (11.5%) *, 1/65 (1.5%) ▲, 1/2 (50%) ◦, 8/20 □ | * Calculated in women with AMH not detectable, 18 months after end of chemotherapy, all chemotherapy regimens; ▲ ABVD; | All patients received monthly GnRH agonist co-treatment during chemotherapy |
| Amzai et al. 2022 [ | North Macedonia | Retrospective | 81 | 27.3 (14–49) | Not specified | 10 | HL, | ABVD, BEACOPP | 6/81 (7.4%) *, 4/74 (5.4%) ▲, 2/7 (28.6%) □ | * Calculated in women with amenorrhea, all chemotherapy regimens; ▲ ABVD; □ BEACOPP | |
| Ciccarone et al. 2023 [ | Italy | Prospective | 68 | 28.0 (18–40) | Not specified | 0.5–1 | Classical HL, Stage I: 6.3%, Stage II: 56.9%, Stage III: 16.3%, Stage IV: 20.6% | ABVD, BEACOPP | 11/68 (16.2%) * 11/51 (21.6%) ▲ | * Calculated in women with AMH not detectable 12 months after end of treatment, all chemotherapy regimens; | 51.1% of all patients undergoing chemotherapy received GnRHa during treatment |
| Flatt et al. 2023 [ | Canada | Retrospective | 1647 | 26 (+/−SD 6.7) | Not specified | Not specified (follow up until 40th birthday, end of the study (31 December 2018), bilateral oophorectomy, subsequent cancer diagnosis or death) | HL | Not specified | 124/1647 (7.5%) * | * Calculated in women with POI (amenorrhea < 40 years, FSH > 25 IU/L) | |
| Luong et al. 2023 [ | Canada | Retrospective | 644 | 25.5 +/− SD 6.6 (15–39) | Not specified | Not specified (maximum follow-up 31/12/2019) | HL | Chemotherapy was given, but no information on regimens | 33/644 (5.1%) * | * Calculated in women with POI | 49% of patients had radiation therapy, but no details on radiotherapy localization available; POI risk in chemotherapy only group: 15/328 (4.6%), POI risk in chemotherapy + radiation group: 18/316 (5.7%) |
| First Author, Year of Publication | Country | Study Design | Number of Participants of Interest | Age of Participants of Interest at Diagnosis/ | Age | Follow-Up After Treatment, Length in Years (Range) | Tumor Type | Chemotherapy, Details | Infertility as Assumed | Infertility Parameter | Comments |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Frias et al. 2003 [ | USA | Prospective | 3 | 27–40 | 28–42 | 1–2 | HL | NOVP | 1/3 (33.3%) * | * Calculated in men with azoospermia or oligozoospermia, treatment with NOVP | |
| Bizet et al. 2012 [ | France | Retrospective | 24 | 25 (+/−SD 7.6) | Not specified | 4.1 (+/−SD 3) | HL | Not specified, treatment with chemotherapy assumed | 12/24 (50%) * | * Calculated in men with azoospermia or oligozoospermia, treatment with chemotherapy assumed | |
| Van der Kaaij et al. 2007 [ | The Netherlands | Prospective | 293 | 30 (15–69) | Not specified | 2.7 (1–11.3) | HL, | ABVD, EBVP, MOPP, MOPP/ABV, BEACOPP | 124/293 (42.3%) *, | * Calculated in men with FSH > 10 U/L, all chemotherapy regimens; ▲ ABVD and EBVP; □ MOPP, MOPP/ABV, BEACOPP | |
| Sieniawski et al. 2008 [ | Germany | Prospective | 38 | 26 (16–58) | 27 (16–52) | 1.45 (0.08–7.8) | HL, | ABVD, COPP/ABVD, BEACOPP baseline or BEACOPP escalated | 71/103 (68.9%) *, 0/4 (0%) ▲, | * Calculated in men with azoospermia, all chemotherapy regimens; ▲ ABVD; | Median time to spermatogenesis recovery: 27 months |
| Kiserud et al. 2009 [ | Norway | Cross-sectional | 165 | Complete cohort of HL and NHL patients: | Complete cohort of HL and NHL patients: | Complete cohort of HL and NHL patients: | HL, | ABVD/EBVP, OEPA, LVPP, BEACOPP, COPP, CHOP/COP | 86/165 (52.1%) * | * Calculated in men with FSH > 12 U/L and/or low testosterone, all chemotherapy regimens | |
| Menon et al. 2009 [ | France | Retrospective | 6 | 17.81 +/− 0.14 (13–20) | 27.36 +/− 1.23 | 4.5 +/− 0.68 | HL | Treatment with polychemo-therapy combined with radiotherapy in 79% of cases | 2/6 (33.3%) * | * Calculated in men with azoospermia, all therapies | |
| Behringer et al. 2013 [ | Germany | Prospective | 708 | 34 (18–49) | 38 (19–57) | 4 (1.5–4.1) | HL, | HD 13: ABVD or AVD; | 411/708 (58.1%) *, | * Calculated in men with FSH > 10 U/L, all chemotherapy regimens; | Birth after natural fertilization: |
| Tomlinson et al. 2015 [ | United Kingdom | Retrospective and prospective; prospective arm concentrated on encouraging patients whose samples had been stored for a minimum of 18 months to attend for follow-up semen analysis | 80 | 26 (13–49) | Not specified | 3.33 (0.58–18.2) | HL | ABVD, | 43/80 (53.8%) *, 3/28 (10.7%) ▲, 40/52 (76.9%) ◦ | * Calculated in men with azoospermia, all chemotherapy regimens; ▲ ABVD; | |
| Paoli et al. 2016 [ | Italy | Retrospective | 144 | 26 (13–51) | Not specified | Spermiogram at baseline (T0), 6 (T6), 12 (T12) and 24 (T24) months after end of treatment | HL | Group A: ABVD, Group B: escalated BEACOPP, COPP/ABVD, OPP/ABVD or MOPP | 22/144 (15.3%) *, 0/115 (0%) ▲, 9/13 (69.2%) ◦, 13/16 (81.3%) □ | * Calculated in men with azoospermia, all chemotherapy regimens; ▲ ABVD, 24 months after end of treatment, | |
| Demeestere et al. 2021 [ | Belgium, France | Prospective | 43 | Standard group: 29 (P25–P75: 23–36), | Not specified | 2.42 (2–2.92) | HL, | All patients: BEACOPPesc (2 cycles), | 40/43 (93%) * | * Calculated in men with azoospermia or oligozoospermia in standard and study group, 20–30 months after end of chemotherapy, all treated with BEACOPP | Pregnancy rates: higher likelihood of achieving pregnancy in PET-driven group (study group) (OR, 3.7; 95% CI, 1.4 to 9.3; |
| Laddaga et al. 2022 [ | Italy | Prospective | 19 | 26 (15–37) | Not specified | 8.7 (4.42–14.3) | HL, Stages I–II: 68%, Stages III–IV: 32% | ABVD | 5/19 (26.3%) * | * Calculated in men with azoospermia or oligozoospermia, all treated with ABVD | Birth of child: N = 1/19 (5.3%), all treated with ABVD; no usage of cryopreserved semen |
| Amzai et al. 2022 [ | North Macedonia | Retrospective | 59 | ABVD group: 24.8 (15–43); BEACOPP group: 29.2 (19–38) | Not specified | 10 | HL, complete cohort (N = 287, males and females): Stage I: 17%, II: 33.1%; III: 22.3%; IV: 25.8%; undefined: 1.8% | ABVD, BEACOPP | 6/59 (10.2%) *, 1/49 (2%) ▲, 5/10 (50%) □ | * Calculated in men with azoospermia or oligozoospermia, all chemotherapy regimens; ▲ ABVD; □ BEACOPP |
| First Author, Year of Publication | Country | Study Design | Number of Participants of Interest | Age of Participants of Interest at Diagnosis/ | Age | Follow-Up After Treatment, Length in Years (Range) | Tumor Type | Chemotherapy, Details | Infertility as Assumed | Infertility Parameter | Comments |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Van den Berg et al. 2004 [ | The Netherlands | Retrospective | 14 | Complete cohort of males and females (N = 76): MOPP group: 10.8 (5–14.3); ABVD group: 11.7 (3.8–15.2); ABVD/MOPP group: 13 (5–17.2) | Not specified | Complete cohort of males and females (N = 76): MOPP group: 16.3 (2–24.2); ABVD group: 12.3 (4.9–15.6); ABVD/MOPP group: 5.8 (0.6–11.3) | HL, Complete cohort of males and females: Stage I: 39.5%, Stage II: 26.3%, Stage III: 27.6%, Stage IV: 6.6% | MOPP, ABVD, MOPP/ABVD | 2/14 (14.3%) * | * Calculated in women with irregular periods, all chemotherapy regimens | Pubertal status not mentioned |
| Gupta et al. 2016 [ | Canada | Prospective | 5 | 13.6 (12–14.3) | Not specified | 1.67 (1.58–2.17) | HL | Cyclo-phosphamide, doxorubicin, cisplatin | 0/5 (0%) * | * Calculated in women without menstruation resumption and/or AMH not detectable, all chemotherapy regimens | All patients were post-menarchal at the time of diagnosis/therapy |
| Drechsel et al. 2024 [ | The Netherlands | Prospective | 73 | 15.6 (7.3–18.8) | 17.8 (IQR 15.8–19.1) at T4 (2 years post-diagnosis) | 2 | Classical HL; early stage: 17.3%, intermediate stage: 48.1%, advanced stage: 34.6% | All treatment arms initially 2 cycles of OEPA induction treatment; Early stages: +1 cycle of COPDAC-28; intermediate stages: +2 cycles COPDAC-28 OR DECOPDAC-21; advanced stages: +4 COPDAC-28 OR DECOPDAC-21; 66% of the girls received COPDAC-28- and 34% received DECOPDAG-21 | 5/73 (6.8%) * | * Calculated in females 2 years post-diagnosis and AMH < 0.5 mg/L, all chemotherapy regimens | Menarchal age median (IQR) 13.0 (11.0; 16.0) |
| First Author, Year of Publication | Country | Study Design | Number of Participants of Interest | Age of Participants of Interest at Diagnosis/ | Age | Follow-Up After Treatment, Length in Years (Range) | Tumor Type | Chemotherapy, Details | Infertility as Assumed | Infertility Parameter | Comments |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ben Arush et al. 2000 [ | Israel | Retrospective | 8 | 14.1 (2.1–16.4) | 23.3 (14.8–24.3) | 7.9 (4.1–17.3) | HL, Stages | MOPP, MOPP/ABVD | 7/8 (87.5%) * | * Calculated in men with azoospermia, oligozoospermia and/or FSH > 10 U/L, all chemotherapy regimens | Complete cohort (N = 12 HL, N = 8 NHL): N = 9 prepubertal (Tanner I), N = 3 intrapubertal (Tanner II–III), N = 8 postpubertal (Tanner V); Prepubertal status does not protect from treatment-related gonadotoxicity, as severe impairment of spermatogenesis was observed in most patients treated before puberty. |
| Bordallo et al. 2004 [ | Brazil | Cross-sectional | 18 | 10 (6–19) | 18 (17–23) | 3–11 | HL | C-MOPP/ABV | 15/18 (83.3%) * | * Calculated in men with azoospermia or severe oligozoospermia, all chemotherapy regimens | 14 prepubertal, 7 postpubertal out of complete HL cohort |
| Van den Berg et al. 2004 [ | The Netherlands | Retrospective | 33 | Complete cohort of males and females (N = 76): MOPP group: 10.8 (5–14.3); ABVD group: 11.7 (3.8–15.2); ABVD/MOPP group: 13 (5–17.2) | Not specified | Complete cohort of males and females (N = 76): MOPP group: 16.3 (2–24.2); ABVD group: 12.3 (4.9–15.6); ABVD/MOPP group: 5.8 (0.6–11.3) | HL, complete cohort of males and females: Stage I: 39.5%, Stage II: 26.3%, Stage III: 27.6%, Stage IV: 6.6% | MOPP, ABVD, MOPP/ABVD | 14/33 (42.4%) * | * Calculated in men with FSH > 10 U/L, all chemotherapy regimens | All prepubertal |
| Hobbie et al. 2005 [ | USA | Retrospective | 11 | 13 (6–19) | 21 (18–31) | 6.5 (1.5–21) | HL | COPP/ABV | 9/11 (81.8%) * | * Calculated in men with azoospermia, oligozoospermia, low testosterone < 350 NG/DL and/or FSH > 10 U/L, all chemotherapy regimens | 3/11 prepubertal, 8/11 intra- or postpubertal |
| Van Beek et al. 2007 [ | The Netherlands | Retrospective | 21 | 11.4 (3.7–15.9) | 27 (1.7–42.6) | 15.5 (5.6–30.2) | HL, | ABVD or EBVD with or without MOPP | 13/21 (61.9%) * | * Calculated in men with azoospermia or oligozoospermia, all chemotherapy regimens | Pubertal status for complete cohort: N = 37 prepubertal, N = 15 pubertal, N = 4 (ages 12.3–13.7 years) no data on pubertal status |
| Romerius et al. 2010 [ | Sweden | Retrospective | 19 | Complete cohort of childhood cancer survivors (N = 129): | Complete cohort of childhood cancer survivors (N = 129): | Complete cohort of childhood cancer survivors (N = 129): | HL | Not specified; agents used for complete cohort of childhood cancer survivors: Carmustine, Lomustine, Chlorambucil, Cisplatin, Cyclophosphamide, Melphalan, Procarbazine | 10/19 (52.6%) * | * Calculated in men with azoospermia | Other childhood cancers: Leukemias, brain tumors, HL, NHL, testicular cancer, Wilm’s tumor; Pubertal stage: n = 4: age ≤ 10 years (prepubertal, according to the authors); n = 15: age > 10 years (postpubertal) |
| Rendtorff et al. 2012 [ | Germany | Retrospective | 5 | 14 (10–17) | 27 (24–30) | 14 (10–18) | HL | Not specified, only oncological treatment in childhood or adolescence | 5/5 (100%) * | * Calculated in men with oligozoospermia or azoospermia | Significantly higher rate of azoospermia/oligozoospermia observed in patients who had been treated during or after puberty |
| Servitzoglou et al. 2015 [ | France | Retrospective | 45 | Complete cohort of HL and NHL (N = 171): | Complete cohort of HL and NHL (N = 171): | Complete cohort of HL and NHL (N = 171): | HL | MOPP alone or with ABVD or ABVP; VBVP with OPPA or with COPP | 20/45 (44.4%) * | * Calculated in men with FSH level > 10 IU/L, treatment with procarbazine containing chemotherapy | Complete cohort (N = 171): 63.2% prepubertal, 27.5% during puberty, 9.3% postpubertal |
| Duca et al. 2019 [ | Italy | Cross-sectional | 7 | 10.3 +/− 4.1 | 24.1 +/− 5.4 | Not specified | HL | Treatment with at least chemotherapy | 5/7 (71.4%) * | * Calculated in men with FSH level > 10 IU/L | Subjects aged <10 years probably prepubertal, no further information |
| First Author, Year of Publication | (1) Were the Two Groups Similar and Recruited from the Same Population? | (2) Were the Exposures Measured Similarly to Assign People to Both Exposed and Unexposed Groups? | (3) Was the Exposure Measured in a Valid and Reliable Way? | (4) Were Con-Founding Factors Identified? | (5) Were Strategies to Deal with Con-Founding Factors Stated? | (6) Were the Groups/Participants Free of the Outcome at the Start of the Study (or at the Moment of Exposure)? | (7) Were the Outcomes Measured in a Valid and Reliable Way? | (8) Was the Follow-Up Time Reported and Sufficient to Be Long Enough for Outcomes to Occur? | (9) Was Follow-Up Complete, and If Not, Were the Reasons for Loss to Follow-Up Described and Explored? | (10) Were Strategies to Address Incomplete Follow-Up Utilized? | (11) Was Appropriate Statistical Analysis Used? | Total Score | Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ben Arush et al. 2000 [ | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 6 | moderate |
| Frias et al. 2003 [ | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 9 | high |
| Van den Berg et al. 2004 [ | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 7 | moderate |
| Bordallo et al. 2004 [ | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 5 | low |
| Behringer et al. 2005 [ | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 8 | moderate |
| Bizet et al. 2012 [ | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 5 | low |
| Hobbie et al. 2005 [ | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 6 | moderate |
| Verschuuren et al. 2006 [ | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 8 | moderate |
| Haukvik et al. 2006 [ | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 8 | moderate |
| Giuseppe et al. 2007 [ | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | high |
| Van der Kaaij et al. 2007 [ | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 9 | high |
| Van Beek et al. 2007 [ | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 9 | high |
| Huser et al. 2008 [ | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 9 | high |
| Blumenfeld et al. 2008 [ | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | high |
| De Bruin et al. 2008 [ | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 10 | high |
| Sieniawski et al. 2008 [ | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 9 | high |
| Nitzschke et al. 2009 [ | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 8 | moderate |
| Kiserud et al. 2009 [ | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 8 | moderate |
| Menon et al. 2009 [ | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 5 | low |
| Behringer et al. 2010 [ | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | high |
| Romerius et al. 2010 [ | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | high |
| Dann et al. 2011 [ | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | high |
| Behringer et al. 2012 [ | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | high |
| Van der Kaaij et al. 2012 [ | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 10 | high |
| Rendtorff et al. 2012 [ | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 7 | moderate |
| Behringer et al. 2013 [ | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | high |
| Swerdlow et al. 2014 [ | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 10 | high |
| Huser et al. 2015 [ | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | high |
| Tomlinson et al. 2015 [ | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 6 | moderate |
| Servitzoglou et al. 2015 [ | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 9 | high |
| Boltezar et al. 2016 [ | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 7 | moderate |
| Paoli et al. 2016 [ | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 7 | moderate |
| Gupta et al. 2016 [ | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | moderate |
| Anderson et al. 2018 [ | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | high |
| Duca et al. 2019 [ | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 7 | moderate |
| Demeestere et al. 2021 [ | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 11 | high |
| Decanter et al. 2021 [ | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 8 | moderate |
| Amzai et al. 2022 [ | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 7 | moderate |
| Laddaga et al. 2022 [ | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 7 | moderate |
| Ciccarone et al. 2023 [ | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 9 | high |
| Flatt et al. 2023 [ | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 9 | high |
| Luong et al. 2023 [ | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 8 | moderate |
| Drechsel et al. 2024 [ | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 9 | high |
- —public university
- —Swiss Cancer League
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive Biology and Fertility · Lymphoma Diagnosis and Treatment · Ovarian function and disorders
1. Introduction
Hodgkin lymphoma (HL) represents a distinct malignancy of the lymphatic system, with peak incidence during the prime reproductive years (ages 15–35) [1]. This temporal overlap between disease onset and family planning poses critical challenges for the increasing number of survivors, particularly as incidence rates continue to rise in younger populations and among women [2]. Given current 5-year survival rates exceeding 95% in early-stage disease, fertility preservation has become a key quality-of-life consideration [3].
In early stages, patients between the ages of 18 and 60 years are commonly treated with two cycles of Adriamycin, Bleomycin, Vinblastine, and Dacarbazine (ABVD) followed by involved site radiotherapy (IS-RT), leading to 5-year survival rates of 97% [4,5]. In intermediate stages and among adults, combination chemotherapy, consisting of two cycles of Bleomycin, Etoposide, Adriamycin (doxorubicin), Cyclophosphamide, Oncovin (vincristine), Procarbazine, and Prednisone (BEACOPP), followed by two cycles of ABVD, is commonly administered. Treatment may be followed by involved site radiotherapy (IS-RT), with a reported 5-year survival rate of 99% [6]. In advanced stages, chemotherapy regimens such as BEACOPP and, more recently, Brentuximab vedotin, Etoposide, Cyclophosphamide, Doxorubicin, Dacarbazine, and Dexamethasone (BrECADD) are applied [7,8]. Treatment decisions are guided by interim staging using positron emission tomography/computed tomography (PET/CT), and both approaches are associated with high survival rates.
Chemo- and radiotherapy carry the risk of infertility. The effect of chemotherapy on gonadal function depends on the treatment regimen and the age of the patient and is different in females and males. In particular, the alkylating agents procarbazine and cyclophosphamide, are highly gonadotoxic [9,10,11].
For young HL patients, family planning is often not yet complete or has not yet been discussed at the time of initial diagnosis. Accordingly, around 20% of women counseled for fertility preservation measures are diagnosed with lymphoma, mostly HL [12].
To avoid under- or overtreatment in terms of fertility preservation measures, it is crucial to evaluate the potential risk of infertility prior to the initiation of gonadotoxic therapies. Many studies, including those conducted by the German Hodgkin Study Group (GHSG), have investigated the impact of different chemotherapies on gonadal function. Various parameters such as hormone levels, sperm analyses, and menstrual cycle history in women were used [7,13,14]. The knowledge provided by these studies needs to be consolidated by systematically and comprehensively analyzing and summarizing all studies published since 2000.
The objective of our systematic review and meta-analysis is to perform such a systematic and comprehensive summary and to provide a precise assessment of presumed infertility associated with different chemotherapies and the age of patients with HL. The study is part of the FertiTOX project (www.fertitox.com, accessed on 3 August 2025), which aims to close the data gap regarding the risk of infertility of anticancer therapies to provide more accurate advice about fertility preservation measures [15,16,17,18,19,20,21,22]. It serves as a comprehensive reference for oncologists and reproductive physicians to inform their patients regarding the advisability of fertility preservation prior to chemotherapy.
2. Materials and Methods
2.1. The Registration of Protocols
The protocol for this study was registered with the International Prospective Register of Systematic Reviews (PROSPERO; registry number: CRD42023384052). The study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [23].
2.2. Search Strategy
A systematic literature search was conducted in February 2024 across MEDLINE, Embase, the Cochrane Database of Systematic Reviews, and CENTRAL (Figure 1). An initial search strategy for Embase was developed by an experienced medical librarian and validated against a test reference set. Following refinement and consultation, tailored search strategies were constructed for each database using a combination of controlled vocabulary (e.g., thesaurus terms and subject headings) and free-text terms, including synonyms, acronyms, and related expressions. The search was restricted to publications from 2000 to February 2024 and encompassed all subtypes of HL.
A double-negative strategy incorporating the Ovid “humans-only” filter was applied to exclude animal-only studies. Detailed search strategies for each database are available in Supplementary File S1. In addition to database searches, the reference lists of relevant articles and reviews were manually screened to identify further eligible studies. All retrieved citations were imported into Covidence and duplicate records were identified and removed [24].
2.3. Inclusion and Exclusion Criteria
Study selection was performed independently by three reviewers (MR, MK, AV) using Covidence (www.covidence.org, accessed on 3 August 2025) [25]. Original articles were included if they reported on HL, treatment modality (at least treatment with chemotherapy), and fertility outcomes measured at least one year after treatment cessation, with the provision that sufficient data was available to calculate prevalence estimates. Presumed infertility, the primary outcome of this study, was defined as reproductive impairment based on surrogate markers rather than confirmed live birth outcomes. Table 1 outlines the specific clinically relevant surrogate markers used to define presumed infertility in this meta-analysis. Studies in which presumed infertility could not be assessed according to these predefined criteria were excluded. For studies reporting the parameters listed in Table 1 in a non-extractable form or only as median/mean values, corresponding authors were contacted to obtain original data. Studies were excluded if the reported mean or median age of female participants at diagnosis or treatment was 30 years or older. Studies with mean or median ages below 30 years were included even if they contained some patients aged 30 years or older, as individual-level exclusion was not feasible in aggregated data. The age threshold of 30 years was chosen to minimize confounding by age-related decline in ovarian reserve, which becomes increasingly relevant from the thirties onward and may independently affect fertility outcomes. This approach aimed to better isolate chemotherapy-associated gonadotoxicity from physiological age-related fertility decline. Patients who had undergone pelvic radiation or stem cell transplantation, as well as those receiving recurrence therapy, were not considered if they represented more than 10% of the total cohort.
2.4. Data Extraction
Data were extracted and independently reviewed by two investigators (MR and MK). The primary variables of interest included study population characteristics such as age at diagnosis and at outcome assessment, duration of follow-up, type of oncological treatment (especially chemotherapy regimens), and parameters used to define presumed infertility (Tables 2–5). Any discrepancies were resolved through discussion and consensus. If multiple surrogate markers of presumed infertility (as listed in Table 1) were available, the most unfavorable outcome was used. Chemotherapy regimens were grouped as all regimens combined, ABVD only, BEACOPP (including all regimens containing BEACOPP irrespective of cycle number, dose, or whether baseline or escalated), and other regimens. For studies lacking specific treatment details, it was assumed that patients had received chemotherapy.
2.5. Quality Assessment
The methodological quality of each included study was assessed using the Joanna Briggs Institute Critical Appraisal Checklist for Cohort Studies [27]. Each item was rated as “yes” (1 point), “no” (0 points), “unclear” (0 points), “partly” (0 points), or “not applicable” (0 points). Based on the total score, studies were classified as high quality (9–11 points), moderate quality (6–8 points), or low quality (0–5 points). Two authors (MR and MK) independently evaluated the risk of bias for each study. Any discrepancies were resolved through discussion and consensus. The quality ratings for all included studies are presented in Table 6.
2.6. Data Synthesis
The primary outcome of this systematic review and meta-analysis was the prevalence of presumed infertility in male and female patients with HL after chemotherapy. Subgroup analyses were conducted according to sex, chemotherapy regimen, and age at the time of treatment. To estimate prevalence, the number of individuals meeting the criteria for presumed infertility was divided by the total number of patients at risk, as reported in the respective studies. For pooled prevalence estimates, statistical analyses were performed using the “metafor” package in R (version 4.2.3; R Core Team, Vienna, Austria, 2013). Heterogeneity across studies was assessed using Cochran’s Q test and the I^2^ statistic. In cases of substantial heterogeneity, random-effects models were applied.
3. Results
3.1. Results of the Systematic Review
In total, 419 studies were assessed following screening of titles, abstracts, and full texts. Of these, 368 were excluded as they did not meet the predefined inclusion criteria, resulting in 50 studies being included in the systematic review and 43 in the meta-analysis (Figure 1).
3.2. Study Characteristics
The characteristics of the 43 studies included in the meta-analysis are presented in Table 2, Table 3, Table 4 and Table 5, stratified by adult females, adult males, female children/adolescents, and male children/adolescents. The studies comprised retrospective (n = 21), prospective (n = 19), and cross-sectional (n = 4) designs. The reviewed studies reported relevant outcomes used to define presumed infertility, as summarized in Table 1. In females, premature ovarian insufficiency or menstrual cycle disorders were the most commonly assessed outcomes, followed by abnormal hormonal parameters (elevated follicle-stimulating hormone (FSH), undetectable anti-Müllerian hormone (AMH)). In males, presumed infertility was predominantly defined by azoospermia or oligozoospermia, with some studies also applying elevated FSH levels. Methodological quality assessment classified 22 studies as high, 18 as moderate, and 3 as poor (Table 6). The studies originated from Europe (n = 34), Asia (n = 3), the United States (n = 2), Canada (n = 3), and South America (n = 1).
Sample sizes ranged from 3 to 1647 patients (adult females: 19–1647; adult males: 3–708; female children/adolescents: 5–73; male children/adolescents: 5–45). At diagnosis or therapy, the pooled median age was 27 years in both adult females (range 9–49) and adult males (range 6–69). Among female children/adolescents, the pooled median age was 13 years (range 3.8–18.8), and among male children/adolescents 11 years (range 0.1–19). Pubertal status was inconsistently reported: in female children/adolescents, most were post-menarchal, whereas in male children/adolescents a substantial proportion were prepubertal (up to 63%). At study participation, median age was infrequently reported, with pooled medians of 32 years in adult females (range 25–49), 28 years in adult males (range 27–49), and 23.3 years in children/adolescents (range 17.8–29). The pooled median follow-up was 7.4 years (range 1.5–20). Most studies specified the applied chemotherapy regimens; in four studies chemotherapy was reported without regimen details, and in three studies no treatment information was provided, with chemotherapy being assumed.
3.3. Results of the Meta-Analysis
Overall, 43 studies met the inclusion criteria and were included in the meta-analysis.
3.4. Pooled Overall Prevalence of Presumed Infertility After All Chemotherapy Regimens
All 43 studies were included in the analysis of presumed infertility prevalence across the reported chemotherapy regimens, comprising 5564 females (5472 adults, 92 children/adolescents) and 1631 males (1464 adults, 167 children/adolescents). The prevalence estimates of the individual studies and the pooled prevalence are presented in Figure 2, Figure 3, Figure 4, Figure 5 and Figure 6. The overall prevalence of presumed infertility was 21% (95% CI: 14–29%) in adult females, 45% (95% CI: 29–62%) in adult males, 53% (95% CI: 30–75%) in children/adolescents overall, 8% (95% CI: 4–15%) in female children/adolescents, and 67% (95% CI: 51–79%) in male children/adolescents. Significant heterogeneity was observed in adult females, adult males, and all children/adolescents combined (I^2^ = 96%, 92%, and 79%; all p < 0.0001), whereas no heterogeneity was detected in female children/adolescents (I^2^ = 0%, p = 0.6573) and moderate heterogeneity in male children/adolescents (I^2^ = 49%, p = 0.0478).
3.5. Subgroup Analysis of Presumed Infertility According to Chemotherapy Regimen and Gender
Three chemotherapy groups (ABVD, BEACOPP, and others) were evaluated in adult HL patients and stratified by sex (Figure 7, Figure 8, Figure 9, Figure 10, Figure 11 and Figure 12). Presumed infertility prevalence was lowest after ABVD, at 6% in both sexes (95% CI: 3–10% in females [n = 1115], 2–17% in males [n = 516]), with substantial heterogeneity among females (I^2^ = 79%, p < 0.0001) and moderate heterogeneity among males (I^2^ = 46%, p = 0.0862). Presumed infertility prevalence was highest after BEACOPP, with 38% in females (95% CI: 24–53%, n = 589), for whom the heterogeneity test indicated substantial heterogeneity (I^2^ = 76%, p < 0.0001). In males, presumed infertility prevalence reached 81% (95% CI: 63–92%, n = 809), likewise with significant heterogeneity (I^2^ = 85%, p < 0.0001). Treatment with other chemotherapy regimens was most frequently based on Meclorethamine, Oncovin (vincristine), Procarbazine, and Prednisone (MOPP); Meclorethamine, Oncovin (vincristine), Procarbazine, Prednisone combined with Adriamycin (doxorubicin), Bleomycin, and Vinblastine (MOPP/ABV); Chlormethine, Lomustine, Vinblastine, Procarbazine, and Prednisone (ChlVPP); or Cyclophosphamide, Oncovin (vincristine), Procarbazine, and Prednisone combined with ABVD (COPP/ABVD).
These regimens were associated with presumed infertility rates of 35% (95% CI: 28–43%) in females (I^2^ = 75%, p = 0.0002) and 69% (95% CI: 60–77%) in males (I^2^ = 23%, p = 0.2740).
4. Discussion
This systematic review and meta-analysis assessed the presumed infertility following chemotherapy for HL, aiming to improve fertility counselling, and is, to the best of our knowledge, the first to stratify results by age, sex, and treatment regimen. Our study revealed an overall pooled prevalence of presumed infertility in HL survivors, with risks in adults for women (21%) and adult men (45%), and in children/adolescents for females (8%) and males (67%). Stratification by chemotherapy regimen shows that the risk of presumed infertility in adults varies by treatment and sex. ABVD is associated with a low risk in both women (6%) and men (6%), BEACOPP confers an intermediate risk in women (38%) and a high risk in men (81%), while other regimens generally carry an intermediate risk in both women (35%) and men (69%).
Numerous studies, including those conducted by the German Hodgkin Study Group (GHSG), have investigated the gonadotoxicity of various therapies in both men and women [8,13,14,35,37] in 562 female HL survivors under 40 years at diagnosis.
Behringer et al. [14] reported that age ≥ 30 years and treatment with BEACOPP were associated with decreased AMH levels, elevated FSH levels, and less regular menstrual cycles, suggesting impaired fertility and highlighting the impact of both age and therapy on post-treatment ovarian function. Similarly, Demesteere et al. [43] found that advanced-stage HL patients (mean age ~27 years) receiving six cycles of BEACOPP had poorer hormone levels and higher rates of premature ovarian insufficiency compared with those treated with a PET-adapted BEACOPP–ABVD regimen, emphasizing the effect of chemotherapy intensity on ovarian function. In contrast secondary amenorrhea occurs infrequently following ABVD therapy without BEACOPP, with a rate of only 3.9% [13].
Our meta-analysis in adult women supports these findings, revealing substantially higher rates of presumed infertility following BEACOPP compared with ABVD treatment.
Other studies in men indicate that chemotherapy primarily affects spermatogenesis, which may already be impaired before treatment, especially in advanced stages, while testosterone production is generally less affected [67].
Behringer et al. [14] found that Inhibin B and FSH levels correlated with chemotherapy intensity, with preserved fertility after early-stage therapy but markedly higher rates of oligozoospermia following six to eight cycles of BEACOPP. Paoli et al. [55] examined sperm parameters and azoospermia rates following different chemotherapy regimens. ABVD caused a temporary reduction in sperm concentration, which normalized within 24 months, suggesting preserved fertility. In contrast, 2–8 cycles of BEACOPP resulted in azoospermia in 50% of cases, and regimens such as COPP, OPP, or MOPP in 85%, consistent with presumed infertility.
Our meta-analysis, incorporating abnormal hormone levels and semen parameters, including azoospermia and oligozoospermia, confirmed higher presumed infertility after BEACOPP, while infertility rates following ABVD aligned with the literature.
The evidence on infertility following chemotherapy for HL in children and adolescents is considerably more limited than in adults, with more data available for male than for female children and adolescents.
Van Beek et al. [11] studied 56 male children/adolescents with HL treated with ABVD/EBVD, with or without alkylating agents (MOPP), evaluating hormone parameters and semen analysis 15.5 years after therapy. Alkylating-agent-containing chemotherapy caused long-term gonadal damage, with 62% of patients showing azoospermia or oligozoospermia, whereas ABVD/EBVD was considerably less gonadotoxic (0% azoospermia/oligozoospermia). Van den Berg et al. [57] studied 17 female children/adolescents with HL. ABVD preserved regular menstrual cycles, whereas alkylating-agent therapy caused irregular cycles in a minority of patients.
These findings largely align with the presumed infertility rates reported in our meta-analyses, indicating a markedly higher risk among male than female survivors of childhood/adolescent HL.
According to current guidelines [4], all patients should be offered fertility preservation prior to potentially gonadotoxic therapy. Based on the results of our study, we recommend an individualized approach tailored to the expected risk of presumed infertility associated with each chemotherapy regimen.
In patients treated with ABVD, where the expected risk of presumed infertility is below 20%, as well as in female children and adolescents, primary (before cancer therapy) fertility preservation is usually not needed. If fertility preservation is not performed, post-treatment follow-up in reproductive medicine should be arranged to assess ovarian reserve and consider secondary (after cancer therapy) preservation options [68].
A presumed infertility risk above 20% is expected with several chemotherapy regimens, including BEACOPP, MOPP, OPPA, COPP, ChlVPP, LOPP, and MVPP. Primary fertility preservation is therefore strongly recommended.
The treatment of newly diagnosed, advanced-stage classical HL is currently undergoing changes based on the results of the HD21 study [7]. BrECADD has been demonstrated to be a more efficacious and better-tolerated alternative to BEACOPP. Across both sexes, FSH recovery four years after therapy was higher following BrECADD than BEACOPP (women: 95% vs. 73%; men: 86% vs. 40%) [8], with a correspondingly higher 5-year incidence of parenthood in BrECADD-treated patients, suggesting substantially lower presumed infertility. Although the BrECADD protocol appears to carry a comparatively lower risk of presumed infertility, long-term data are not yet available and additional studies are needed. Therefore, fertility preservation should be recommended as a precautionary measure for all patients prior to treatment with BrECADD, with counselling provided by specialized reproductive medicine specialists in coordination with the treating oncologists.
Despite rigorous methodology, our study has limitations. Importantly, presumed infertility represents a surrogate-marker-based construct rather than a direct measure of reproductive outcomes such as live birth. Accordingly, many included studies relied on heterogeneous surrogate endpoints, including hormonal parameters, menstrual function, or semen quality, rather than clinically documented infertility. This variability may introduce misclassification and lead to either under- or overestimation of clinically meaningful infertility. Therefore, pooled prevalence estimates should be interpreted as indicators of gonadal dysfunction rather than definitive measures of reproductive incapacity.
A substantial degree of heterogeneity was observed across pooled estimates, particularly in adult and mixed-regimen analyses. This heterogeneity warrants cautious interpretation of the reported prevalence of presumed infertility. Likely contributors include differences in cumulative chemotherapy doses, supportive care measures, duration of follow-up, and variability in outcome definitions across studies. In addition, treatment regimens were not uniformly specified in all cohorts, especially in older studies, further increasing clinical heterogeneity. Nevertheless, patients were treated for Hodgkin lymphoma during eras in which chemotherapy-based regimens constituted standard of care, supporting the assumption of systemic treatment exposure despite incomplete regimen-level detail.
In children and adolescent cohorts, it was often unclear whether treatment occurred pre- or postpubertally, reflecting limited and inconsistent reporting of pubertal status. This limits the assessment of gonadotoxicity, may have influenced infertility risk estimates—particularly among adolescents—and constrains recommendations for fertility preservation.
5. Conclusions
This first meta-analysis evaluating the pooled prevalence of presumed infertility after HL chemotherapy, stratified by age, sex, and treatment regimen, provides clinically relevant information to guide fertility counselling. Our results support a differentiated approach: for adult HL patients receiving ABVD and for female children or adolescents, a “wait-and-see” strategy to assess gonadal function post-therapy may be appropriate, with secondary fertility preservation considered if needed. In contrast, primary fertility preservation should be strongly recommended for patients receiving other treatment regimens, particularly those containing alkylating agents such as BEACOPP, and for adolescent males. These findings underscore the importance of personalized counselling and highlight the need for further studies, especially evaluating newer regimens such as BrECADD, to refine risk estimates and optimize fertility preservation strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kahn J. Dabaja B. Wu S. Kelly K. Berkahn L. Pavlovsky A. Sureda A. La Casce A. Classic Hodgkin lymphoma Hematol. Oncol.202442 e 323910.1002/hon.323938037872 · doi ↗ · pubmed ↗
- 2Huang J. Pang W.S. Lok V. Zhang L. Lucero-Prisno D. Xu W. Zheng Z.-J. Elcarte E. Wong M. Incidence, mortality, risk factors, and trends for Hodgkin lymphoma: A global data analysis J. Hematol. Oncol.2022155710.1186/s 13045-022-01281-935546241 PMC 9097358 · doi ↗ · pubmed ↗
- 3Robert Koch Institute, Department of Epidemiology and Health Monitoring Available online: https://www.krebsdaten.de/Krebs/DE/Content/Krebsarten/Morbus%20Hodgkin/morbus%20hodgkin_node.html(accessed on 3 February 2025)
- 4AWMF S 3-Leitlinie Version 3.2: Diagnostik, Therapie und Nachsorge des Hodgkin Lymphoms bei Erwachsenen Patienten, Stand Available online: https://register.awmf.org/assets/guidelines/018-029O Ll_S 3_Hodgkin-Lymphom_Erwachsene_Diagnostik_Therapie_Nachsorge_2022-10.pdf(accessed on 1 March 2025)
- 5Engert A. Plütschow A. Eich H.T. Lohri A. Dörken B. Borchmann P. Berger B. Greil R. Willborn K.C. Wilhelm M. Reduced treatment intensity in patients with early-stage Hodgkin’s lymphoma N. Engl. J. Med.201036364065210.1056/NEJ Moa 100006720818855 · doi ↗ · pubmed ↗
- 6Borchmann P. Goergen H. Kobe C. Lohri A. Greil R. Eichenauer D.A. Zijlstra J.M. Markova J. Meissner J. Feuring-Buske M. PET-guided treatment in patients with advanced-stage Hodgkin’s lymphoma (HD 18): Final results of an open-label, international, randomised phase 3 trial by the German Hodgkin Study Group Lancet 20173902790280210.1016/S 0140-6736(17)32134-729061295 · doi ↗ · pubmed ↗
- 7Borchmann P. Ferdinandus J. Schneider G. Moccia A. Greil R. Hertzberg M. Schaub V. Hüttmann A. Keil F. Dierlamm J. Assessing the efficacy and tolerability of PET-guided Br ECADD versus e BEACOPP in advanced-stage, classical Hodgkin lymphoma (HD 21): A randomised, multicentre, parallel, open-label, phase 3 trial Lancet 202440434135210.1016/S 0140-6736(24)01315-138971175 · doi ↗ · pubmed ↗
- 8Ferdinandus J. Schneider G. Moccia A. Greil R. Hertzberg M. Schaub V. Hüttmann A. Keil F. Dierlamm J. Hänel M. Fertility in patients with advanced-stage classic Hodgkin lymphoma treated with Br ECADD versus e BEACOPP: A secondary analysis of the multicentre, randomised, parallel, open-label, phase 3 HD 21 trial Lancet Oncol.2025261081109010.1016/S 1470-2045(25)00262-140652943 · doi ↗ · pubmed ↗