Cancer Prevention Clinical Trials: Advances and Challenges
Elizabeth R. Francis, Farzeen Z. Syed, Arun Rajan, Eva Szabo

TL;DR
This paper reviews the challenges and recent advances in cancer prevention clinical trials, focusing on new strategies to translate scientific insights into effective public health solutions.
Contribution
The paper highlights recent innovations in trial design and immune-based prevention methods that could transform cancer prevention from theory into practice.
Findings
Prevention trials require large populations and long durations to demonstrate effectiveness, posing significant logistical and financial challenges.
Recent advances in trial methodology and immunopreventive strategies offer promising new approaches for cancer prevention.
Early-phase trials are critical for refining interventions and generating preliminary data to support larger phase III trials.
Abstract
Cancer affects millions worldwide, and preventing the disease before it develops is a more favorable approach than treating established cancer. Despite significant advances in understanding how cancer forms, creating effective prevention strategies has proven challenging. Prevention trials require large populations followed for many years to show benefit, which is both costly and complex. Recent innovations in trial design and immune-based prevention methods offer new opportunities to overcome these obstacles. This review examines the challenges in cancer prevention and the emerging strategies that could transform prevention from theory into practice. Prevention of cancer is an appealing strategy to reduce the burden of illness associated with cancer, but despite the rapidly advancing understanding of the early phases of carcinogenesis, translation of biologic insights into actionable…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
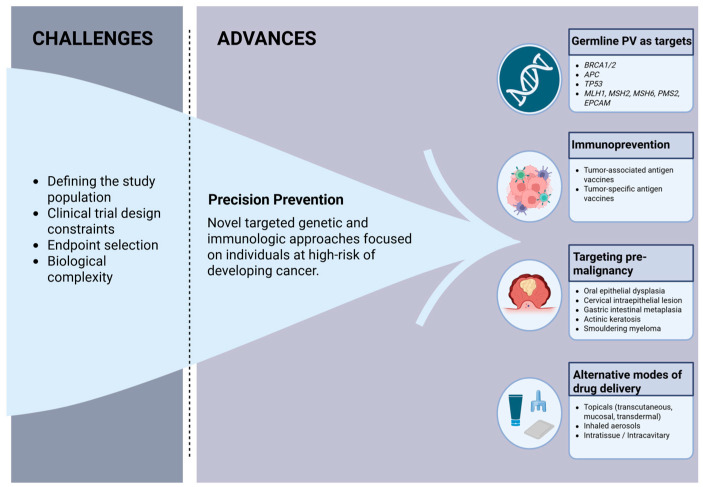 Figure 1
Figure 1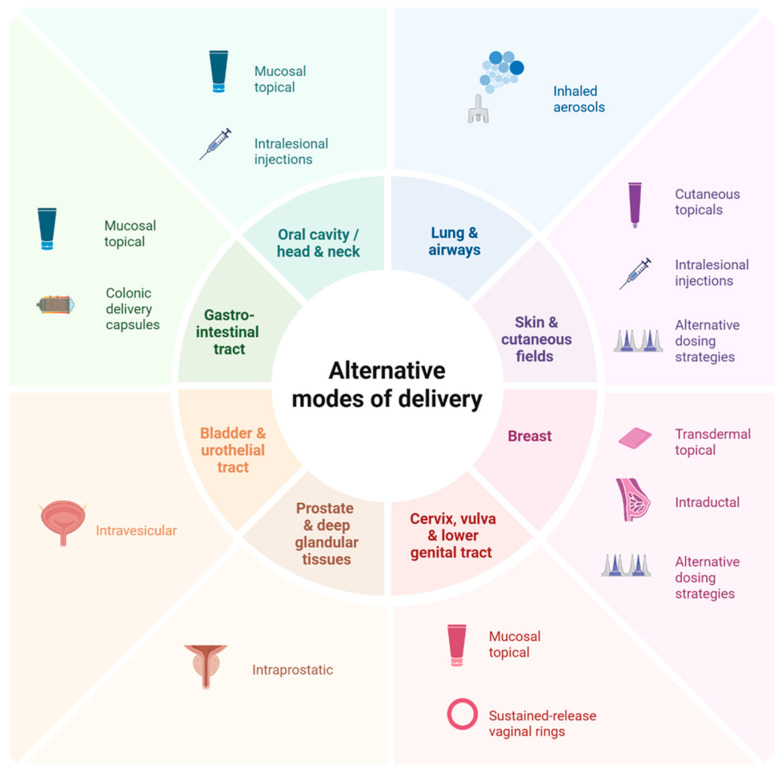 Figure 2
Figure 2- —Intramural Research Program of the National Institutes of Health (NIH), National Cancer Institute, Center for Cancer Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEthics in Clinical Research · Biological Research and Disease Studies · Health, Environment, Cognitive Aging
1. Introduction
While recent decades have witnessed immense progress in the treatment and early detection of cancer, reducing the global burden of cancer remains a daunting challenge [1]. Demographic predictions indicate that by 2050, there will be 35 million new cancer cases worldwide, so substantial investments in prevention, to include risk factor mitigation (e.g., smoking, alcohol, overweight/obesity, and infection), are needed to avert this large number of cancer cases and deaths. A multi-pronged approach to targeting the process of carcinogenesis throughout its life cycle, from initiation through metastasis, is understood to be key to making cancer a manageable chronic disease.
However, after the initial enthusiasm of targeting the carcinogenic process when it is less complex and accompanied by less immunosuppression than metastatic disease, the inherent difficulties in preventing ‘that which is not yet present’ have become evident. Cancer treatment has evolved to target the vastly different biological processes giving rise to different cancer types (e.g., targeting a variety of actionable driver mutations in non-small cell lung cancer and other cancers) to harness the power of genomic analysis to bring precision oncology to clinical practice. In an analogous fashion, precision prevention aims to use the mechanistic understanding of the carcinogenic process to bring preventive strategies to individuals who are most likely to benefit from the interventions and less likely to experience negative effects [2], albeit without the benefit of easy genomic analysis to assess which pathway to carcinogenesis is or will be occurring in a given individual.
The field of cancer prevention is at a crossroads. The promise of a rapidly increasing understanding of carcinogenesis has identified a number of gaps that need to be addressed prior to successful translation to routine clinical care. As discussed below, carcinogenesis is a complex process occurring via different mechanisms and at different rates throughout the body. The incomplete understanding of this process and the inability to assess the extent of ongoing carcinogenesis in any given individual at any given time limit our ability to identify rational prevention targets and to precisely match individuals with the right interventions. Risk assessment often requires invasive procedures to identify individuals at high risk for cancer and to assess the effect of interventions on biomarkers of malignancy. These procedures are generally not part of the standard of care, complicating accrual to clinical trials and adding significantly to trial cost. There is a need to develop noninvasive biomarkers, both for risk and endpoint assessment. Furthermore, there is a lack of validated surrogate endpoints to replace cancer incidence and thereby shorten trial duration. In this review, we summarize the challenges facing the development of interventions to target ongoing carcinogenesis, and we discuss recent advances with the potential to bring interventions to public health benefit.
2. Challenges in Cancer Prevention Trial Design
2.1. Biological Complexity
The challenges of cancer prevention begin with the fundamental biology of carcinogenesis. Carcinogenesis is inherently a heterogeneous process driven by multiple independent clones that coexist within the same anatomical region, creating a field of genetically and epigenetically altered epithelium [3]. Not only is there heterogeneity in the driving processes that lead to cancers arising in different organs and between individuals with a cancer arising from the same organ, but there is also considerable evolutionary clonal variation within each individual [4]. In head and neck mucosa, for example, carcinogen exposure produces a broad field of injury in which distinct premalignant clones develop and evolve independently, making it difficult to target a single lesion or pathway [5]. This concept of field cancerization extends across multiple organ systems and reflects widespread molecular alterations that are not clinically visible or necessarily targetable by the same intervention [6]. As a result, sampling a single lesion often fails to capture the biological diversity present within the entire field. Furthermore, spatial patterns of early cancer growth demonstrate that premalignant lesions may contain multiple subclones with different evolutionary trajectories and signaling profiles, forming a mosaic of risk rather than a uniform premalignant population [7]. Even within a single field, genetically distinct clones diverge early, potentially making the response to a single targeted preventive agent highly variable [5].
Biological heterogeneity also makes it far more difficult to evaluate efficacy in prevention than in treatment. Cancer incidence endpoints occur years after the intervention begins, and imaging does not reliably capture early biological changes. As a result, prevention trials rely heavily on mechanistic understanding, animal models, and epidemiologic signals to identify rational targets [8]. Where possible, efforts focus on biologically defined high-risk groups where initiating pathways are clear, such as individuals with germline syndromes or oncogenic drivers, because the known initiating mutation provides a more precise and potentially actionable target for prevention.
In summary, this heterogeneity has profound implications for preventive trial design and successful intervention, particularly in non-germline cohorts. As difficult as it is to obtain at-risk or premalignant tissue (which often requires invasive procedures to obtain tissue), there is a real possibility that tissue sampling may miss the pertinent molecular target(s). Interventions will need to be broad enough to account for clonal evolution, which suggests that targeting single molecular abnormalities or pathways downstream of germline mutations or oncogenic drivers may be difficult to accomplish without the emergence of resistance bypass mechanisms. Furthermore, since phase II trial designs depend on assessing the effect of an intervention on intermediate or surrogate endpoints (see Section 2.3 below), the choice of the primary efficacy endpoint is particularly critical. A positive result may be misleading if the endpoint is not intrinsically involved in carcinogenic progression, but a negative result may lead to apparent trial failure despite underlying biological activity. Similar issues of biologic heterogeneity and clonal evolution complicate the development of cancer treatments, although they are magnified in preventive agent development due to the difficulties in tissue sampling and prediction of events and abnormalities that have not yet become biologically apparent.
2.2. Risk and Benefit Constraints
Cancer prevention trials have to operate within a narrower risk versus benefit window in comparison to treatment-focused trials, as they enroll largely healthy or asymptomatic individuals who may be exposed to long-term interventions and who may not develop cancer during the duration of the trial, or ever. In this setting, even modest toxicities can be deemed unacceptable when the potential benefit is a reduction in future cancer risk for only a subset of the exposed individuals rather than control of an active disease in the majority. While frequent but not life-threatening adverse events (e.g., low-grade diarrhea or nausea) limit participant compliance with long-term treatment, rare but serious events become unacceptable in the prevention setting.
The Adenoma Prevention with Celecoxib (APC) and Adenomatous Polyp Prevention on Vioxx (APPROVe) trials reflect this challenge. Although celecoxib and rofecoxib (Vioxx) significantly reduced colorectal adenoma recurrence, both were associated with dose-related increases in serious cardiovascular events [9,10,11]. The adverse events from the APPROVE and other trials ultimately led to market withdrawal of rofecoxib, and, similarly, the risk-benefit balance of celecoxib for cancer prevention was not deemed acceptable for long-term use for cancer prevention [12].
Similarly, in prostate cancer, the Prostate Cancer Prevention Trial (PCPT) showed that finasteride reduced overall cancer incidence but raised concerns for high-grade disease and caused sexual dysfunction [13]. Collectively, these examples highlight how a relatively small increase in serious adverse outcomes can outweigh the potential benefit of reducing cancer incidence.
An example of how tolerability restricts prevention strategies is illustrated by the breast cancer prevention trials, such as NSABP P-1 [14]. While tamoxifen significantly reduced invasive breast cancer in high-risk women, real-world use has remained modest due to a low but real absolute risk of endometrial cancer (albeit without increasing mortality), venous thromboembolism, and menopausal symptoms associated with treatment [15]. These challenges highlight that, unlike the treatment setting where patients and physicians may accept substantial toxicity for disease control, prevention agents must offer both risk reduction and a benign toxicity profile for acceptance by otherwise healthy individuals. The same agent used for different indications has considerably lower acceptance in the prevention setting.
Furthermore, there are no standard criteria for acceptable toxicity thresholds across cancer prevention settings. Instead, tolerability depends on baseline risk, anticipated benefit, and treatment duration, with evidence derived from individual trials rather than systematic cross-cancer comparisons [16,17]. Patient-reported outcomes (PROs) and adherence data help bridge this gap by providing insight into how patients experience preventive interventions. However, these measures remain underused as decision drivers in prevention trials, which complicates risk-benefit assessment [18].
Within prevention settings, low-grade symptoms, even if clinically mild, can disproportionately affect quality of life in asymptomatic populations and impact long-term adherence [19]. Because clinician-reported adverse events may underestimate symptom burden, PROs help capture symptoms that influence adherence [20]. Inconsistent adherence complicates efficacy assessment, as reduced drug exposure can mask treatment benefits, making it difficult to distinguish biological inefficacy from inadequate exposure [21]. Despite their relevance, PROs and adherence metrics are rarely used as primary or key secondary endpoints in early-phase cancer prevention trials. Challenges in standardization and lack of consensus thresholds limit their influence on trial design and regulatory use [22].
2.3. Measuring Preventive Efficacy
Assessing efficacy in cancer prevention trials is challenging because definitive (and approvable) endpoints such as cancer incidence and mortality occur years after an intervention begins and require large sample sizes for proper evaluation [23]. Unlike treatment settings, where response can be measured with CT or other imaging, these tools rarely detect the early biological effects of preventive agents, which occur at the level of dysplasia or molecular alterations that are not captured reliably by imaging [24]. As a result, many trials rely on intermediate or surrogate endpoints such as lesion regression, histologic grade, or biomarker modulation, even though the extent to which these measures reflect true cancer risk often remains uncertain. To be a good surrogate, a marker should be intrinsic to the process of carcinogenesis and to the mechanism of action of the intervention, such that modulating marker expression would also affect the course of the disease. Marker expression should differ between normal and diseased or at-risk epithelium, and measurements should be reproducible. To be a true surrogate, validation is critical [25,26]. Similar challenges are seen in cancer screening, where surrogate endpoints can shorten trial duration but require extensive validation to ensure they truly reflect true reductions in cancer incidence or mortality [27].
Thus far, no true surrogates have been validated for cancer prevention. Biomarkers assessed in most early-phase prevention trials remain exploratory, although they can be informative and help develop the body of evidence needed for subsequent phase III trials. Premalignant lesions are often used as endpoints even though their natural history remains highly variable. Oral leukoplakia, for example, may regress, persist, or progress to cancer, and reported malignant transformation rates have varied across studies. This variability complicates efforts to interpret changes in lesion size or dysplasia grade as definitive evidence of prevention [28]. Similar challenges arise elsewhere within the aerodigestive tract, where dysplasia endpoints in bronchial or esophageal prevention trials fluctuate over time and may improve without altering long-term cancer risk [5]. These uncertainties demonstrate that intermediate changes in histology or biomarkers do not reliably predict whether an intervention reduces cancer incidence and generally cannot be used as approvable endpoints in phase III trials, although they can be indicators of preliminary efficacy that subsequently need to be confirmed in larger phase III studies with cancer incidence endpoints [29]. Similarly, molecular endpoints such as methylation signatures, signaling pathway modulation, or immune profiling can be highly informative but are not sufficient for regulatory approval.
Evaluating endpoints also frequently requires tissue, which introduces additional limitations. Many cancer prevention studies depend on serial biopsies of premalignant tissue to assess histologic or molecular changes, leading to repeated invasive procedures over months or years. This requirement contributes to slow accrual, lower retention, and added procedural risk in otherwise healthy participants, and it limits the generalizability of trial results. Reliance on invasive endpoints is one of the key barriers to efficient chemoprevention research [23]. Although emerging noninvasive biomarkers, including circulating DNA assays and methylation-based signatures, are under investigation, they remain unvalidated and have not yet replaced tissue-based measures in most prevention settings.
2.4. Cohort Identification
Cohort selection is another difficult aspect of prevention trial design because very high-risk groups are not necessarily the most generalizable populations. High-risk hereditary syndromes such as BRCA1/2, Lynch, or Li-Fraumeni allow cancer endpoints to be reached sooner and can justify exposure to preventive agents. Where mechanisms of carcinogenesis are shared between high-risk (e.g., genetic) cohorts and individuals with sporadic cancers, trials initially in high-risk cohorts can offer a shortcut to drug development. However, in most cases, the mechanisms are not adequately understood and thus cannot be generalized to the population at large. The Metformin in Li-Fraumeni Syndrome (MILI) trial, for example, randomizes adults with Li-Fraumeni syndrome to metformin plus MRI surveillance versus surveillance alone, using five-year cancer-free survival as the primary endpoint. This design illustrates how very high-risk cohorts make event-driven prevention trials feasible and can justify long-term exposure to an oral agent that is regarded as safe but is not without any toxicities [29]. Should this trial be positive, it would be a major step forward for the care of these individuals who are at high risk for multiple different cancers, although it would not be generalizable to other populations since the rationale is partially based on the enhanced oxidative metabolism in p53-deficient cells from Li-Fraumeni patients and pertinent mouse models.
Equity and access limitations pose an additional challenge for cohort selection. Genomic-driven prevention trials offer biological precision, but access to genetic testing and specialized surveillance remains uneven. This raises concerns that such approaches could widen existing health disparities among socioeconomic, racial, and geographic groups [30]. Prevention strategies are often developed case-by-case, tailored to specific risks or molecular drivers, rather than designed for population-wide application [31]. While a targeted approach is necessary to demonstrate initial efficacy, extending these strategies to broader populations remains difficult, especially where genomic testing may be unavailable or inconsistently implemented [32].
Additionally, the identification of cohorts with premalignant lesions introduces a different set of selection challenges. Studies in these cohorts allow earlier, lesion-based endpoints, but these lesions may be relatively uncommon and show substantial variability within the underlying biology. Trials tend to accrue slowly due to the need to use invasive methods (e.g., colonoscopy or bronchoscopy, etc.) to screen multiple individuals to identify those who harbor the requisite lesions. These factors also limit their ability to represent broader at-risk populations. At the other end of the spectrum, trials in more broadly defined high-risk populations, such as postmenopausal women with elevated breast cancer risk, yield results that are more generalizable if they reach a cancer incidence endpoint, but this requires much larger sample sizes and longer follow-up to observe cancer events (e.g., phase III trial designs). The MAP.3 and IBIS-II trials, for instance, enrolled thousands of women at moderately increased risk and showed that exemestane and anastrozole, respectively, can reduce breast cancer incidence, but only with prolonged treatment and extended post-treatment follow-up [33,34].
Taken together, cancer prevention trials are limited by heterogeneous biology, narrow toxicity margins, unvalidated or invasive endpoints, and challenges in selecting appropriate cohorts. High genomic risk or lesion-based cohorts allow early endpoints but limit generalizability, whereas broader high-risk groups improve applicability at the cost of larger and longer trials. These constraints underscore the need for strategies that improve target selection, reduce toxicity, and make trial designs more feasible.
3. Advances in Prevention Trials: Transition to Precision Prevention
3.1. Overview of Precision Prevention
Advances in genomics and digital health [35], together with the recognition of the need to refine cancer prevention trial endpoints [16], are prompting a shift from traditional prevention trials to precision prevention studies, which use targeted genetic and immunologic approaches in individuals at high risk of developing cancer to halt or “intercept” the progression from premalignant to invasive cancer (Figure 1) [36]. Contrary to traditional phase III prevention trials, which focused on population-level risk factors such as diet and smoking and frequently used repurposed interventions or diet-derived agents [37,38,39], precision prevention focuses on individualized risk prediction and novel biologically informed interventions in a smaller high-risk population [40]. Precision studies utilize short-term surrogate endpoints such as cancer incidence (in extremely high-risk populations) and biomarker changes and favor an integrated approach with treatment or surveillance protocols [40]. In this way, precision prevention studies will allow for a more targeted and mechanistically informed approach that is more likely to be cost-effective and faster to conduct than traditional prevention trials, which on average require 10–15 years to complete [40].
Though precision prevention trials allow for more targeted and efficient interventions, there are certain limitations to consider. For instance, over-stratification and small sample sizes diminish statistical power and increase variability, necessitating multi-center designs and adaptive analytics. Moreover, as surrogate endpoints may not reliably predict long-term reductions in disease risk, incorporating post-trial surveillance and leveraging population-level registry data with linked tissue resources [41] are important considerations. Given this, precision prevention trials complement rather than replace population-level prevention trials, which offer greater statistical stability and generalizability and benefit from established post-trial surveillance infrastructure.
3.2. Germline Pathogenic Variants as Therapeutic Targets
Germline pathogenic variants (PV) are heritable DNA changes present in all cells that predispose an individual to develop certain diseases, including cancer [42]. Well-established oncologic syndromes with associated germline PVs include hereditary breast and ovarian cancer (BRCA1/2), Lynch syndrome (MLH1, MSH2, MSH6, PMS2, and EPCAM), Li-Fraumeni syndrome (TP53), and Cowden syndrome (PTEN). Recent studies have focused on therapeutically targeting these germline PVs, fundamentally changing the management of certain cancer predisposition syndromes [8].
The use of PARP inhibitors (PARPi) in hereditary breast and ovarian cancer (HBOC) is the first key example of a germline PV as therapeutically actionable [43]. Germline and somatic mutations in BRCA1/2 lead to an inability to perform homologous repair of DNA defects [44]. PARPi, like olaparib, capitalize on this weakness as they block the repair of single-strand DNA breaks by inhibiting PARP enzymes on DNA, causing replication-associated double-strand breaks that are lethal to cells lacking functional homologous recombination [45]. In the late 2000s, the synthetic lethality of PARPi was confirmed in humans with advanced BRCA1/2-mutated advanced breast, ovarian, and prostate cancers [46]. This led to PARPi use for maintenance therapy in BRCA-mutated and homologous recombinant-deficient ovarian cancer [47,48,49] and expanded use of PARPi from the metastatic breast cancer setting [50,51] to early-stage germline BRCA breast cancer [50,52], where a significant improvement in overall survival was observed [53]. Though PARPis are not approved for the prevention of cancer in individuals with BRCA1/2 germline PV, this is an active area of investigation [54]. The development of next-generation PARP1-selective inhibitors, such as saruparib, offers the potential for more tolerable agents that may be better suited for cancer prevention [55].
When considering a drug for cancer prevention in such high-risk populations, several factors must be assessed, including the penetrance of the germline pathogenic variant, the drug’s tolerability and late effects, and the response of the agent in patients with germline PV who have developed cancer [56]. Using HBOC and PARPi again as an example, the penetrance of BRCA1/2 is high (68–80% for BRCA1 and 75–88% for BRCA2 for breast cancer; 60–65% for BRCA1 and 30–37% for BRCA2 for ovarian cancer) [57], and PARPi are well tolerated, albeit not without any side effects, as evidenced by a relatively low (<12%) permanent discontinuation of PARPi due to toxicity in pivotal maintenance trials [50,58]. Although our understanding of PARPi late effects is still evolving, the significant impact of PARPi on the management of early-stage and metastatic BRCA1/2 breast and ovarian cancer makes PARPi a potential agent for continued investigation for precision prevention in populations at very high cancer risk.
Though not reviewed in detail here, it is also important to recognize prevention trials pertaining to therapeutic agents in other cancer predisposition syndromes (Table 1). Due to their high cancer risk, individuals with cancer predisposition syndromes are frequently studied early during preventive drug development to enrich for the cancer incidence endpoint, as long as the underlying mechanisms are potentially similar to those giving rise to sporadic carcinogenesis. Thus, the trials in Table 1 do not necessarily reflect targeting the abnormal predisposition gene.
In contrast, many germline PVs (e.g., APC I1307 K and ATM) confer a modest increase in cancer risk and often act in concert with other genetic and environmental factors, making it difficult to justify the initiation of preventive therapeutics in these populations. A polygenic risk score (PRS) offers a quantitative measure of an individual’s risk for a disease [71,72,73], providing insight on which individuals may benefit from early preventive intervention. However, PRS determination has multiple limitations, including uncertain clinical thresholds, variable accuracy across populations, nonstandardized analytic approaches, and lack of prospective validation, constraining PRS use in prevention trials [74,75]. Though PRS shows promise as a personalized precision prevention strategy, providing insight not only on who is at greatest risk for disease development but also possibly guiding when and how intense to initiate therapy, more rigorous refinement and standardization are needed.
3.3. Immunoprevention
Since the 1980s, the field of immunoprevention, or the use of vaccines or immune-modulating strategies to prevent cancer [76,77], has enveloped three main phases—viral vaccines, antigen-based vaccines, and precision immunoprevention [36,63]. Vaccines against oncogenic viruses such as the human papillomavirus and hepatitis B virus [64] significantly reduced the incidence of cervical cancer and hepatocellular carcinoma, respectively [78,79,80,81]. Building on this success, the next phase of immunoprevention centers on antigen-based approaches, which established the groundwork for precision immunoprevention.
Antigen-based vaccines target either tumor-associated antigens (TAA), non-mutated self-proteins expressed in tumors, or tumor-specific antigens (TSA), typically mutation-derived neoantigens expressed in tumor cells [82]. Though they have had limited success in treating advanced cancers [82,83,84,85,86], these vaccines show promise in primary and secondary prevention (Table 2), which is our focus herein, and variable success in tertiary prevention and as adjuvant treatments [87,88,89]. Success in these settings is attributed to low disease burden [88,89], limited clonal heterogeneity, and a potentially less suppressed immune system [90,91]. Additional strategies employed by successful preventive antigen-based vaccines include concomitant administration of additional immunomodulatory drugs to overcome immunosuppression, careful consideration of the selected target antigen, and focus on high-risk populations such as those with premalignant lesions or germline pathologic variants (Table 2). For instance, the presence of the transmembrane glycoprotein mucin 1 (MUC1) in premalignant lesions as well as in several cancers such as colon and lung, Refs. [92,93] has made it a desirable TAA vaccine target, with promising results in the preclinical [94,95] and early clinical settings [96,97,98] in healthy individuals at risk of cancer development. Similarly, given the role of cancer stem cells (CSC) in cancer onset and metastasis [99,100], CSC antigens such as crypto-1 and cystine-glutamate antiporter xCT [101,102], which are expressed in early and invasive breast cancer, have emerged as compelling TAA vaccine targets that have shown promising anti-metastatic effects in preclinical analyses [102,103,104,105].
Tumor neoantigens, highly immunogenic tumor-specific proteins not expressed on normal cells [112], represents another promising target for prevention and forms the basis for TSA vaccines [113]. The possible success of TSAs as cancer prevention vaccines is predicated on utilizing neoantigens with high diversity, such as those formed by frameshift mutations [114] and gene fusions [115], rather than single-nucleotide variations, as the former produce a higher immunogenic response. Utilizing neoantigens that are less individualized, such as those from common oncogenic driver mutations like KRAS, TP53, and BRAF, allows for large-scale, cost-effective vaccine production [82] and could possibly prevent tumor evolution with antigen-loss variants [116]. For instance, a novel Lynch syndrome frameshift peptide vaccine is a first-in-kind precision preventive vaccine that targets neoantigens from recurrent microsatellite mutations common in Lynch syndrome patients, leveraging the active immune microenvironment of Lynch polyps associated with colorectal cancer [117,118]. Preclinical studies demonstrated robust immunogenic responses, reduced intestinal tumor burden, and prolonged overall survival in mice [119,120], providing strong support that neoantigen vaccines may be effective in Lynch syndrome and prompting initiation of an early phase clinical trial, which is ongoing, but has already confirmed feasibility, tolerance, and immunogenicity (NCT05078866) [110,111,121]. In addition to assessing late effects and long-term safety, future research will focus on confirming whether this vaccine does prevent Lynch-associated cancers.
Though a form of antigenic vaccines, TSAs reflect a broader transition in immunoprevention clinical trials to precision interception, an evolution made possible due to advances in sequencing and multi-omics [113] and a greater understanding of immunotherapy. It remains to be seen if TSA vaccines will outperform TAAs, but their role as cancer preventive agents remains an active area of investigation. Further, although the late effects of these vaccines remain unknown, they are currently administered to populations with a history of cancer or at high risk for developing a primary malignancy or recurrence. An extended follow-up will be required before considering their use in the general population at average cancer risk.
3.4. Targeting Known Premalignancy
Focusing on premalignant lesions in an attempt to prevent invasive cancer is not a new concept [122,123,124,125]. However, what has shifted is the framing of premalignant lesions as a targetable disease state with biologically defined risk, which can be modulated via multiple advanced modalities that consider molecular and immunological principles. For instance, the risk of progression from a premalignant state to invasive cancer can be quantified by considering multiple factors, including genomic characteristics [126], the immune microenvironment [127,128] and pathological features [129] such as TP53 loss, aneuploidy, PD-L1 expression, and histological grade, as well as the presence of biomarkers like ctDNA [130] and targetable mutations such as BRCA1/2 [131]. Currently, only clinical and pathological features are used for clinical decisions; however, there is strong biological support to pursue the development of a multimodal risk system that incorporates other factors.
Artificial intelligence (AI) has primarily used single-modality data to risk-stratify premalignant lesions. For instance, AI deep learning has been applied to assess the histopathology of biopsied precursor lesions [132] and to non-invasively infer biological aggressiveness from imaging phenotypes [133,134]. Emerging multimodal AI approaches now integrate diverse data types to enhance predictive accuracy. Indeed, tissue-specific models such as TissueCypher, a multi-institutionally validated fluorescence imaging platform which uses AI to integrate various factors, including biomarkers (e.g., loss of tumor suppressor genes, amplification of oncogenes, alterations in lipid metabolism) [135,136] and tissue morphology, provides a 5-year risk score predictive of progression from nondysplastic or low-grade dysplastic Barrett’s esophagus to high-grade dysplasia or esophageal adenocarcinoma [129,137,138,139,140]. TissueCypher has superior risk stratification predictability than traditional approaches and has exhibited a meaningful impact on clinical management, affecting 55% of cases in a small prospective observational study [141]. While this represents a single, tissue-specific example, broader generalizations across cancers and tissue types remain challenging.
Efforts to understand and map out the multidimensional nature of multiple premalignant lesions have been the focus of the PreCancer Atlas (PCA) project [142], an initiative launched in 2018 as part of the Cancer Moonshot’s Human Tumor Atlas Network (HTAN) [143,144]. As of November 2025, HTAN teams have constructed 14 atlases using data from 20 organs and 64 cancer types. Precancer atlases have been reported on sporadic colorectal cancer [145,146,147], familial adenomatous polyposis-related colorectal cancer [148,149,150], lung cancer [151,152,153], breast cancer [154,155,156,157], melanoma [158,159], and pancreatic cancer [160]. By integrating multi-omic features such as genomic, transcriptomic, epigenetic, and immune microenvironmental profiles with established histological characteristics, PCA aims to provide clarity on why some premalignant lesions progress to invasive cancer, whereas others stabilize or regress. This multidimensional view may permit a more accurate risk stratification of multiple premalignant lesions, which can be utilized to develop targeted precision-prevention and early interception strategies [142,161].
3.5. Alternative Modes of Drug Delivery
Toxicity, including immediate adverse events and late effects, is critical to consider when considering an agent for cancer prevention, as discussed above, and tolerability and toxicity are major challenges to the long-term delivery of preventive interventions. Alternative dosing strategies are one approach to decreasing toxicity that has shown some success. For example, exemestane administration three times weekly was found to be noninferior to once daily dosing in a short window-of-opportunity pre-surgical trial, providing an approved agent as an alternative option for early-stage estrogen receptor-positive breast cancer patients intolerant to once daily dosing and providing the rationale for a larger, longer trial to assess breast cancer preventive efficacy [162]. Similarly, topical 5-fluorouracil (5-FU) was noted to have improved tolerance with biweekly dosing rather than with daily dosing or decreased concentrations [163,164,165].
Another approach to limit toxicity focuses on local organ-specific delivery rather than traditional systemic therapy (Figure 2) [166]. Regional drug delivery modalities include topical formulations, inhaled aerosols, and intra-tissue or intracavity approaches. Of these, topical agents (cutaneous, transdermal, and mucosal) are the most studied local preventive delivery modalities, for instance:
- Cutaneous topicals: Cutaneous cancer-prevention topicals leverage direct delivery to the skin for local action. Approved monotherapy topical treatments such as 5-FU and imiquimod, and the investigational combination of calcipotriol with 5-FU, have shown good clearance of actinic keratosis (AK), the precursor lesion to squamous cell carcinoma (SCC) of the skin [167,168]. Indeed, the combination of calcipotriol with 5-FU was noted to significantly lower the risk of SCC development within three years of treatment and produced a robust T-cell response [168], prompting investigation of its use in high-risk groups with AK, such as transplant recipients (NCT05699603) [169].
- Transdermal topicals: Transdermal topicals utilize the skin for systemic or loco-regional delivery of a drug, bypassing hepatic first-pass metabolism [170]. The transdermal tamoxifen metabolite 4-hydroxytamoxifen, delivered in gel form, was noted to have fewer systemic symptoms than oral tamoxifen, including reduced coagulation parameters, in patients with estrogen receptor-positive ductal carcinoma in situ of the breast, but has had mixed results on efficacy. One early randomized controlled trial noted that the gel matched the antiproliferative effect of oral tamoxifen [171], although this was not confirmed in a larger randomized trial by Khan et al., who suggested that future trials enhance metabolite delivery or use a more potent analog to improve response [172].
- Mucosal topicals: Mucosal topicals have been studied across various anatomical locations, including the cervix [164,171,173,174], vagina [175,176], vulva [177,178], anus [179], oral cavity [180,181], and the gastrointestinal tract. Of these, agents targeting vulvar intraepithelial neoplasia (VIN) and cervical intraepithelial neoplasia (CIN), precursors to vulvar and cervical carcinoma, respectively, have shown the most promise. For instance, imiquimod has been associated with high durable response rates for VIN [182] and has been effective at treating high-grade CIN [183]. Though not superior to surgical resection, imiquimod is estimated to prevent surgery in at least 40% of high-grade CIN cases and may represent a non-surgical option that mitigates the toxicities associated with surgery [183].
A promising emerging use for preventive topical mucosal agents is in the gastrointestinal tract, with the development of hydrogels containing thiolated mucoadhesive polymers, which create temporary bonds with mucosal surfaces, extending drug contact time [184,185]. When combined with stimulus-release hydrogel technology, such as pH or enzyme-sensitive activation, including azo-polymeric hydrogels [186] and nanoparticle systems [187], thiolated hydrogels have the potential for controlled release of a drug specifically within the colonic mucosa [188,189]. To date, no trials have examined thiolated hydrogels as a primary chemoprevention strategy for colorectal cancer; however, pre-clinical studies have shown promise [190].
Beyond topical agents, other regional drug delivery modalities are emerging. For instance, inhalable aerosols, which take advantage of the lungs’ large surface area, thin epithelial barrier, and high vascularization [191] to directly deliver drugs in the airway, are an approved drug modality used to treat multiple pulmonary conditions, such as asthma. Given their ability to directly deliver drugs to premalignant lung lesions, their use as a preventive drug modality is currently under exploration. Multiple preclinical studies have noted significant reductions in pulmonary tumor multiplicity, load, and formation with various aerosolized agents [192,193,194,195]; however, in early-phase clinical trials, aerosols have shown modest effects [196,197]. While not yet demonstrating clear preventive benefit, the aerosolized delivery approach nevertheless remains an intriguing modality under active investigation and highlights a point of intersection between therapeutic advancements and potential preventive application. Similarly, intra-tissue or intracavity approaches (e.g., intravesical, intraductal, intraprostatic, intralesional injections, colonic delivery capsules, and vaginal rings) (NCT06623110) [188,198,199,200,201,202,203,204,205] also aim to directly deliver drugs to the organ systems of concern, and are emerging preventive modalities that will be watched closely. As with aerosols, many of these modalities originate from approved therapeutic uses in these organ systems.
4. Conclusions
With a rapidly increasing understanding of the biology of early carcinogenesis, cancer prevention is entering a new precision phase that promises to match the right intervention to the right individual. The past decade has seen major improvements in prevention target selection based on a deeper appreciation of premalignant biology at the epithelial as well as microenvironment and systemic immunity levels. The focus on homogeneous high-risk populations, such as those with germline mutations, enhances the likelihood of picking up an efficacy signal in early-phase clinical trials, although generalizability to the population at large remains to be determined. However, the possibility that many (maybe even most) preventive interventions will be limited to high-risk populations rather than average-risk individuals must be considered. Alternative approaches, such as screening or lifestyle interventions, may be needed for average-risk individuals.
The recognition of tremendous biological heterogeneity in tumor evolution, both between and within individuals, has reframed the approach to prevention in favor of targeting carcinogenic pathways over individual molecular abnormalities. Harnessing the immune system to eliminate premalignancy and prevent progression to invasive disease is an attractive approach being investigated in multiple cancer prevention settings. Additionally, attention to the delivery of effective therapies to optimize high compliance has resulted in multiple trials of localized drug delivery systems to optimize the risk-benefit calculation.
One of the largest challenges in cancer prevention is the uncertainty of who will develop cancer, when it will occur, and in which organ it will originate. However, individuals at high risk for one cancer remain at risk for other cancers and for other chronic diseases associated with similar exposures or aging. For instance, while heavy smoking is a risk factor for multiple tobacco-associated malignancies, an individual with such exposure still remains at risk for common non-tobacco-associated malignancies such as breast or prostate cancer. Approaches that target multiple cancer types by virtue of shared pathogenesis or shared molecular abnormalities, such as a MUC1 vaccine discussed above, are therefore very appealing, especially as more potent vaccines targeting multiple shared antigens are developed. Furthermore, individuals at risk for cancer are also at risk for multiple chronic diseases (e.g., heart disease and chronic obstructive pulmonary disease from heavy smoking), so approaches that target shared pathogenic mechanisms are particularly appealing [206]. It will take a multi-pronged effort addressing targets, cohort identification, trial design, optimal intervention delivery, and outcome assessment to make sustained progress, but recent advances make such progress within reach. Nevertheless, it must be recognized that preventive interventions cannot exist in a vacuum and must be integrated with population-level strategies such as lifestyle interventions (e.g., tobacco and alcohol cessation, obesity control) and appropriate screening strategies to optimally decrease cancer incidence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F. Laversanne M. Sung H. Ferlay J. Siegel R.L. Soerjomataram I. Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J. Clin.20247422926310.3322/caac.2183438572751 · doi ↗ · pubmed ↗
- 2Rebbeck T.R. Burns-White K. Chan A.T. Emmons K. Freedman M. Hunter D.J. Kraft P. Laden F. Mucci L. Parmigiani G. Precision Prevention and Early Detection of Cancer: Fundamental Principles Cancer Discov.2018880381110.1158/2159-8290.CD-17-141529907587 · doi ↗ · pubmed ↗
- 3Dakubo G.D. Jakupciak J.P. Birch-Machin M.A. Parr R.L. Clinical implications and utility of field cancerization Cancer Cell Int.20077210.1186/1475-2867-7-217362521 PMC 1838897 · doi ↗ · pubmed ↗
- 4De Bruin E.C. Mc Granahan N. Mitter R. Salm M. Wedge D.C. Yates L. Jamal-Hanjani M. Shafi S. Murugaesu N. Rowan A.J. Spatial and temporal diversity in genomic instability processes defines lung cancer evolution Science 201434625125610.1126/science.125346225301630 PMC 4636050 · doi ↗ · pubmed ↗
- 5Han S. Bommireddy R. Kim P. Selvaraj P. Shin D.M. Chemoprevention of Head and Neck Cancer: A Review of Current Approaches and Future Perspectives Cancer Prev. Res.20241744345510.1158/1940-6207.CAPR-24-0093 PMC 1184476938978394 · doi ↗ · pubmed ↗
- 6Willenbrink T.J. Ruiz E.S. Cornejo C.M. Schmults C.D. Arron S.T. Jambusaria-Pahlajani A. Field cancerization: Definition, epidemiology, risk factors, and outcomes J. Am. Acad. Dermatol.20208370971710.1016/j.jaad.2020.03.12632387665 · doi ↗ · pubmed ↗
- 7Lomakin A. Svedlund J. Strell C. Gataric M. Shmatko A. Rukhovich G. Park J.S. Ju Y.S. Dentro S. Kleshchevnikov V. Spatial genomics maps the structure, nature and evolution of cancer clones Nature 202261159460210.1038/s 41586-022-05425-236352222 PMC 9668746 · doi ↗ · pubmed ↗
- 8Tang T.-Y. Colbert Maresso K. Ngeow J. Vilar E. Yap T.A. Germline Mutations as Cancer Drug Targets Cancer Discov.2025152213223410.1158/2159-8290.CD-24-124141178351 · doi ↗ · pubmed ↗