First Clinical Experiences with the Ultra-Fast Time-of-Flight BIOGRAPH One Next-Generation Hybrid PET/MRI System
Otto M. Henriksen, Kirsten Korsholm, Annika Loft, Johanna M. Hall, Annika R. Langkilde, Vibeke A. Larsen, Thomas S. Kristensen, Caroline Ewertsen, Frederikke E. Høi-Hansen, Patrick M. Lehmann, Karen Kettless, Flemming L. Andersen, Thomas L. Andersen, Ian Law

TL;DR
This paper shares early clinical results using a new ultra-fast PET/MRI system, showing good image quality and potential for broader use.
Contribution
First clinical evaluation of the BIOGRAPH One PET/MRI system across multiple tracers and body regions.
Findings
PET image quality was rated as good or very good in 93% of scans.
Diagnostic concordance was observed in 99% of readings.
Image noise was comparable to digital PET/CT and better than first-generation PET/MRI.
Abstract
Objective: We present the first clinical experience with the BIOGRAPH One next-generation PET/MRI system scanner, evaluating its performance for body and brain imaging in patients across multiple tracers. Methods: A total of 59 patients were scanned on the BIOGRAPH One PET/MRI following standard clinical PET/CT (n = 52) or first-generation PET/MRI (Biograph mMR, n = 7). Scans comprised 30 total body (TB), whole body (WB), or regional scans with [18F]FDG, and 29 brain scans with either [18F]FDG (n = 5), [18F]FE-PE2I (n = 10), [18F]FET (n = 4), or [68Ga]Ga-DOTATOC (n = 10). The PET image quality was visually assessed using a 5-point Likert scale (1 = very good to 5 = very bad) and compared with clinical scans acquired on either a current-generation digital PET/CT or a first-generation PET/MRI system, including evaluation of diagnostic concordance. PET quantification and image noise was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
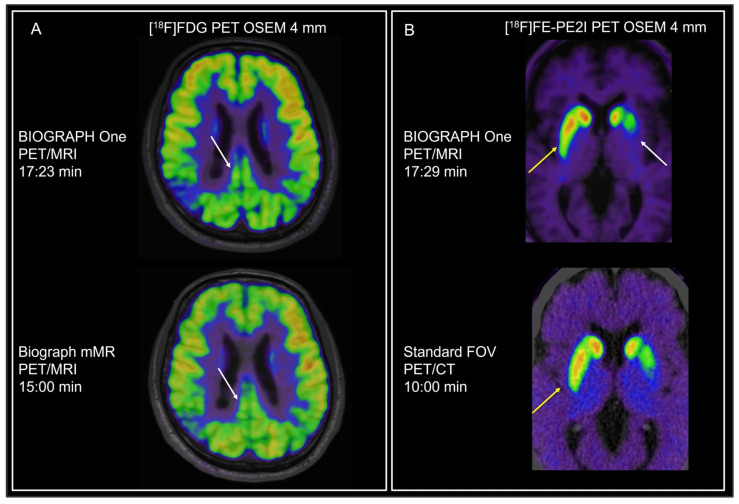 Figure 1
Figure 1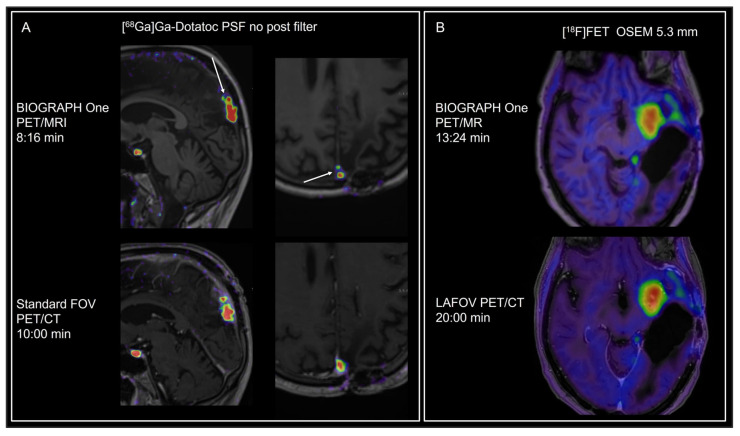 Figure 2
Figure 2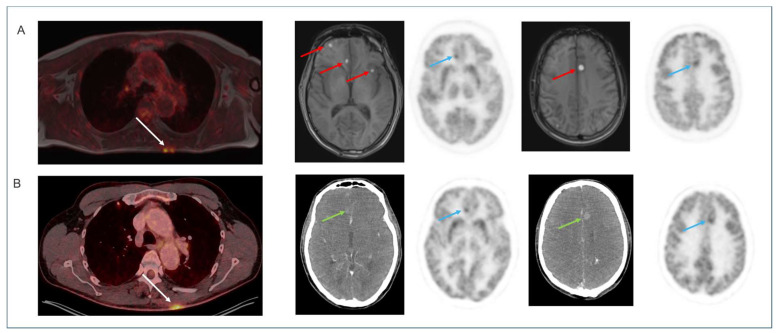 Figure 3
Figure 3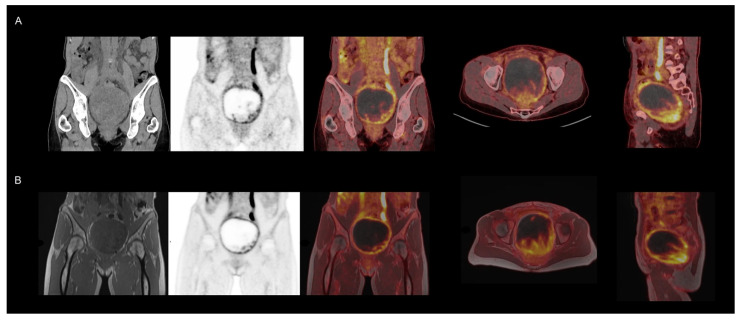 Figure 4
Figure 4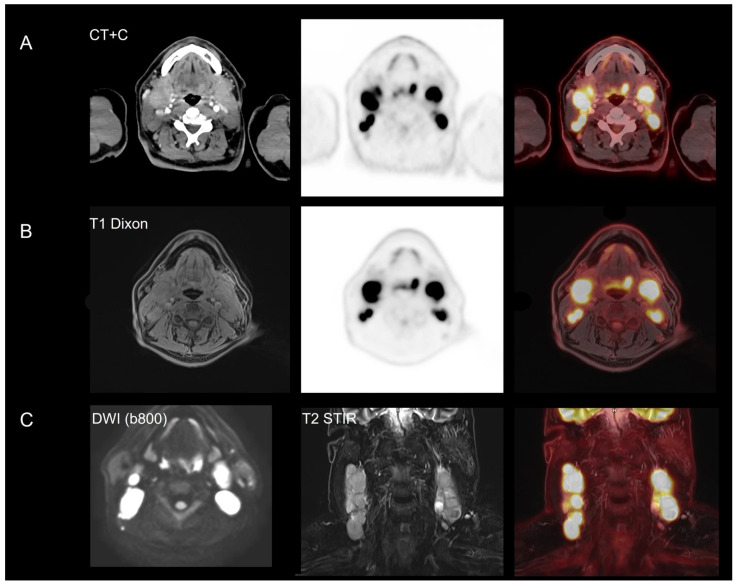 Figure 5
Figure 5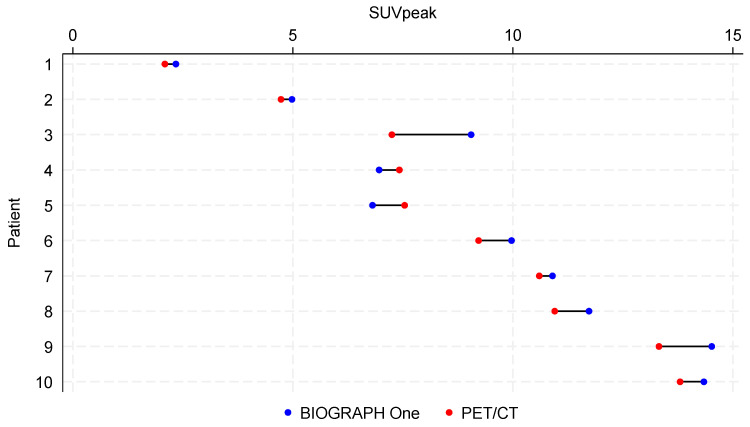 Figure 6
Figure 6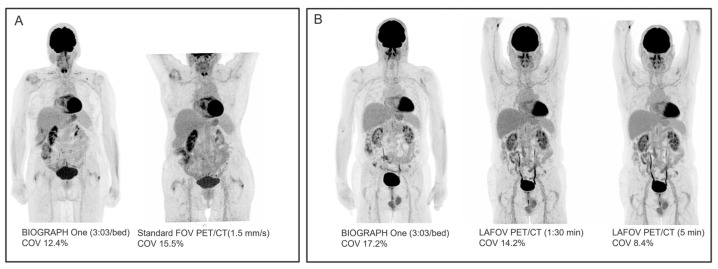 Figure 7
Figure 7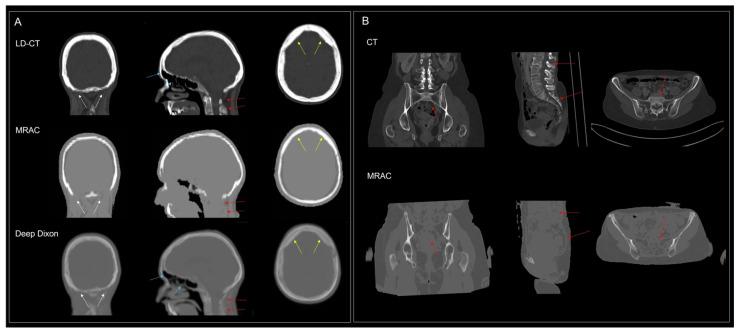 Figure 8
Figure 8- —Siemens Healthineers
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedical Imaging Techniques and Applications · Radiation Detection and Scintillator Technologies · Advanced MRI Techniques and Applications
1. Introduction
Since the introduction of the first commercial integrated hybrid PET/MRI system in 2010 [1,2], a growing number of installations and numerous publications have demonstrated the value of simultaneous PET and MRI. Recent systematic reviews and meta-analyses have concluded that PET/MRI provides similar or superior diagnostic accuracy to PET/CT for a range of malignancies [3,4] including gynecological [5], head–neck [6], prostate [7], breast [8], lung [9], and multiple myeloma [10]. Further, international society practice guidelines have recently been published [11]. PET/MRI has also gained general acceptance for brain imaging as a convenient alternative to separate imaging sessions and is included in current practice guidelines for dementia [12], epilepsy [13], and brain tumors [14].
However, it has become increasingly evident that first-generation hybrid PET/MRI systems are falling behind in terms of MRI performance, PET detector technology, and software capabilities when compared to state-of-the-art stand-alone systems. The first commercial hybrid PET/MRI system (the Siemens Healthineers Biograph mMR, Forchheim, Germany) was equipped with analogue PET detectors lacking time-of-flight (TOF) capability and the MRI system was based on the Magnetom Verio 3T scanner introduced in 2007. Additionally, this system does not use the same software or sequence platform as the vendor’s existing MRI systems. In a PET/MRI user survey, responders raised concerns about the benefit of body imaging using PET/MRI compared to PET/CT, long acquisition times, attenuation correction challenges, and higher operating and maintenance costs as hurdles for daily use [15].
In 2024, Rigshospitalet in Copenhagen was the first clinical site worldwide to install the next-generation BIOGRAPH One PET/MRI system (Siemens Healthineers, Forchheim, Germany). The BIOGRAPH One integrates the current-generation Biograph Vision 600 PET/CT platform (introduced in 2019; Siemens Healthineers, Hoffman Estates, IL, USA) with the 3T MAGNETOM Vida MRI scanners (introduced in 2020; Siemens Healthineers, Forchheim, Germany). Notably, BIOGRAPH One provides an extended PET axial field of view (FOV) of 35.0 cm, compared with 26.3 cm for the Biograph Vision 600 PET/CT and 25.3 cm for the Biograph mMR PET/MRI, thereby enabling higher sensitivity and improved anatomical coverage. The integration of fast TOF resolution and reduced crystal cross-sectional dimensions enables shorter acquisition protocols, improves signal-to-noise ratio (SNR), and enhances image resolution. Clinically, these advancements allow for faster imaging workflows, improved lesion detectability, and potentially reduced patient discomfort during scanning
Following initial testing and software improvements, we conducted a clinical trial for conformity assessment from March to June 2025. Patients were scanned on the BIOGRAPH One PET/MRI following a standard-of-care clinical scan. These data enable a direct comparison of BIOGRAPH One PET/MRI performance with state-of-the-art digital PET/CT and first-generation PET/MRI systems.
In this study, we present our initial clinical experience with brain, whole body (WB), and regional PET imaging, illustrating examples across a range of tracers for diverse clinical indications. Additionally, we discuss potential applications of the enhanced capabilities of BIOGRAPH One PET/MRI in both clinical practice and research settings.
2. Materialsand Methods
The aim of the study was to include a total of 60 adult patients referred to for WB (n = 30) and brain PET (n = 30). The study was approved by both The Medical Research Ethics Committees and The Danish Medicines Agency under Medical Device Regulation article 62 (Case nr: 2401738) and performed according to the Helsinki Declaration. All patients gave informed oral and written consent prior to the PET/MRI scan on the BIOGRAPH One PET/MRI.
All scans on the BIOGRAPH One PET/MRI were performed directly after a clinical scan on one of our standard FOV PET/CT (Biograph Vision 600), long-axis FOV (LAFOV, Biograph Vision Quadra) PET/CT (both Siemens Healthineers, Hoffman Estates, IL, USA), or first-generation PET/MRI (Biograph mMR) systems. Study scans were performed as WB (vertex to mid-femur), total body (TB, vertex to toe), or regional [^18^F]FDG PET scans or brain scans with tracers and indications as summarized in Table 1. PET acquisition and reconstruction protocols are summarized in Table 2. Long-lived tracers with relatively stable tracer binding were selected for the study to visualize pathology on delayed imaging.
PET acquisitions continued throughout the duration of all MRI sequences, thus exceeding the pre-defined minimum target duration for single-bed acquisition (Table 1). For multi-bed acquisitions, an overlap of 6.3 cm was applied resulting in an effective axial coverage of 31.9 cm and allowing WB and TB imaging to be performed by 4 and 7 (or 8) bed positions, respectively. PET imaging was reconstructed using vendor-provided MRI segmentation-based attenuation correction (MRAC), including a bone model. PET reconstruction parameters were chosen to match those of our clinical standard FOV PET/CT protocols
The MRI protocols were designed to simulate fast clinical protocols with both pre- and post-contrast imaging for both brain and female pelvis. All neuro and head and neck scans were acquired with a 20-channel head and neck coil (Biomatrix Head/Neck Pro PET/MR). Either one or two flexible 24-channel body coils (Biomatrix Contour XL) and a 32-channel spine coil (Biomatrix Spine Pro PET/MR) were used for non-brain imaging. Due to study restrictions, no MRI contrast was administered. Details of MRI protocols are provided in Supplementary Table S1.
2.1. Image Reading
Imaging was rated for PET and MRI image quality by a total of eight readers: four experienced nuclear medicine physicians (two readers evaluating brain imaging, and two readers evaluating TB/WB/regional [^18^F]FDG PET) and four experienced radiologists evaluating MRI (two neuro-radiologists and two whole-body radiologists evaluating brain and body imaging, respectively). As the shorter MRI protocols and sequences in the study were not aligned with local preferences, MRI quality scores will be biased negatively. Therefore, the present analysis focuses on the results of the PET readings.
First, images were evaluated using a 5-point Likert scale for overall image quality (1 = very good to 5 = very bad), image noise (1 = none to 5 = very strong), contrast (1 = very good to 5 = very bad), and resolution (1 = very good to 5 = very bad) with a score of 3 indicating acceptable quality. Subsequently, PET image quality was compared to that of the clinical PET/CT or PET/MRI (1 = very good to 5 = very bad) with a score of 3 indicating equal quality, and the diagnostic comparability of the two scans was assessed. Readers were not blinded to the scanner system and no inter-reader agreement analysis was performed.
2.2. Image Analysis
Selected metrics were obtained from [^18^F]FDG PET images to compare the image noise and PET quantification of BIOGRAPH One with that of the clinical PET/CT or PET/MRI scan. For the brain, the standardized uptake value (SUV) in the frontal cortex, occipital cortex, and basal ganglia normalized to the cerebellum (SUVr) was determined using the syngo.via DB Comparison tool (Scenium, version VE70A, Siemens Healthineers, Forchheim, Germany). In non-brain scans, the peak SUV (highest average 1 mL sphere) was determined in 10 patients with [^18^F]FDG avid tumors. In each patient, the lesion or component of the lesion with the highest SUV was included for analysis. Image noise was assessed using the coefficient of variation (COV) in a 5–10 mL volume of interest (VOI) in the liver of WB/TB [^18^F]FDG scans and in a 2 mL VOI in the white matter of brain [^18^F]FDG scans.
2.3. Statistics
Values are reported as the median [inter-quartile range, IQR]. Liver COV and lesion SUVpeak values are compared by Wilcoxon signed rank test. For brain metrics, the number of observations was considered too low for formal statistical testing.
3. Results
Patient recruitment and scans were completed successfully for all categories except for [^18^F]FET, where only 4 of 5 planned patients were recruited within the study period. The median time from the start of the clinical scan to the start of the BIOGRAPH One PET/MRI study scan was 33 min [IQR: 26;36 min]. Median delay, duration, and average quality scores of individual scan protocols are provided in Table 3.
3.1. Image Reading
Based on 59 averaged paired readings (118 in total), the median score was 1.5 [IQR: 1.5;2] for image quality with 93% rated as good or very good. The median scores were 2 [IQR: 2;2] for image noise, 1.5 [IQR: 1.5;2] for contrast, and 1.5 [IQR: 15;2] for resolution. When comparing image quality to the clinical scan, the median (range) score was 3 [IQR: 2.5;3] with 99% rated as equal or better. The average quality ratings of MRI for individual imaging protocols are provided in Supplementary Table S2. In 117 of 118 (99%) of readings, diagnostic comparability was obtained. One single scan rated as non-comparable was related to apparent tracer uptake in bone in a brain FDG scan due to error in the segmentation-based MRAC.
Examples of the different tracers and applications are shown in Figure 1, Figure 2, Figure 3, Figure 4 and Figure 5. MRI identified additional findings in two patients. In one case, an occluded internal carotid artery—undetectable on low-dose CT—was revealed on MRI. In another case, MRI detected additional cerebral metastases compared to contrast-enhanced CT and PET in a patient with malignant melanoma (Figure 3). Conversely, a 7 mm non-FDG-avid pulmonary nodule was reported on CT in one patient, but was not visible on MRI. No other clinically relevant discrepancies were noted.
3.2. Image Metrics
The body and brain PET metrics are summarized in Table 4. Compared to PET/CT and first-generation PET/MRI, the combined median [^18^F]FDG ROI SUVr values from BIOGRAPH One PET/MRI tended to be higher in the frontal cortex (+13.7%), in the occipital cortex (+4.6%), and in the basal ganglia (+8.1%), resulting in noticeable regional differences in the scaling of 3/5 statistical surface projection maps.
The SUVpeak values from WB/TB and regional scans were higher, with a median difference of 6.2% in images from BIOGRAPH One PET/MRI compared to PET/CT (Figure 6), although the difference did not reach statistical significance (p = 0.08).
The image noise (Figure 7 and Table 4) assessed as COV in the liver of WB and TB scans showed a median COV of 17.2% from BIOGRAPH One PET/MRI (n = 15) compared to 15.5% from standard FOV PET/CT (n = 7, p = 0.128 for difference) and 8.1% from the LAFOV PET/CT (5 min) (n = 8, p = 0.012 for difference). For the brain FDG [^18^F]FDG scans, the median COV in WM was 9.6% (n = 5) compared to 11.7% from a 15 min first-generation PET/MRI scan (n = 4), and also lower (8.5% vs. 10.7%) compared to a 10 min clinical scan on standard FOV PET/CT (n = 1).
4. Discussion
In this report, we present our initial clinical experiences with imaging across a range of tracers and pathologies using the world’s first clinical installation of the next-generation BIOGRAPH One PET/MRI system.
Compared directly with its predecessor, the BIOGRAPH One offers markedly improved performance. In addition to longer axial FOV, preliminary PET characterization (data presented at ISMRM annual meeting, 2025, Honolulu, HI, USA, article in preparation) shows a >50% percent increase in sensitivity (14.1 cps/kBq vs. 22.7 cps/kBq), approximately 1 mm improvement in image resolution (4.3 mm vs. 3.4 mm), and a TOF time resolution below 190 ps. In contrast, the Biograph mMR PET/MRI does not have TOF capability. The MRI component is based on the MAGNETOM Vida platform with compatible software and a gradient amplitude increase from 45 mT/m to 60 mT/m.
4.1. PET Image Quality
The scanner demonstrates enhanced PET imaging performance compared to the first-generation Biograph mMR system, offering image quality similar to that of leading digital PET/CT systems. Only a few added or missed findings were observed. As a reminder, our study was not designed to assess potential diagnostic gains or superiority.
The COV measurements were similar or lower than our reference systems with the exception of the LAFOV PET/CT (5 min scan). However, COV values are a limited measure of scanner performance, due to decreased tissue activity from physical and biological decay in delayed images and differences in scan duration and reconstruction parameters.
The improved sensitivity may permit shorter scans or reduced administered activity compared to Biograph mMR PET/MRI. Although not equivalent to standard longer MRI protocols, shorter protocols may be attractive in patients who are not able to complete a standard clinical protocol. Combining accelerated MRI with MRI-guided PET reconstruction [16] could permit ultra-fast low-dose imaging, e.g., a 5 min brain protocol at less than half standard activity. Alternatively, acquiring PET data during the full duration of a standard MRI protocol could allow for a significant dose reduction. Low-dose imaging is of particular importance in children, pregnant women, patients with cancer-prone syndromes, and healthy volunteers.
4.2. PET Quantification
The systematically higher SUVr values in brain [^18^F]FDG are consistent with the well-known bias in segmentation-based MRAC which may adversely impact the image reading. This is a particular issue using statistical surface projections comparing patient data to normal controls from PET/CT, or when using a reference region for calculation of uptake metrics. At our institution, we have relied on an in-house developed deep learning Dixon-based synthetic CT for PET/MRI MRAC showing superior PET quantification accuracy [17,18].
The SUVpeak values in FDG-avid lesions in body imaging were higher, although not statistically significant, and likely related to later imaging times. Some regional bias may be derived from the segmentation-based MRAC (Figure 8).
By visual analysis, tracer distribution differed insignificantly for [^18^F]FET (Figure 2) and [^68^Ga]Ga-DOTATOC was constant with mean SUV differing by <5%.
4.3. Brain Applications
At our institution PET/MRI is the preferred one-stop-shop imaging modality for memory clinic patients with >800 exams performed yearly. The BIOGRAPH One PET/MRI will allow for shorter protocols or advanced imaging sequences within a clinically acceptable scan duration. Other key applications are the use of amino acid PET imaging of gliomas [19] and [^68^Ga]Ga-DOTATOC, although attention to effects of the MRAC method is of key importance [18].
The longer axial FOV of 35 cm permits better coverage of large arteries and will provide an image-derived input function less affected by partial volume effects [20] for quantitative kinetic modeling in research and the clinic, e.g. for cerebrovascular flow reserve measurements with [^15^O]H_2_O PET [21].
4.4. Non-Brain [18F]FDG Oncology Applications
For non-brain imaging, [^18^F]FDG PET/CT represents a robust and versatile modality with wide applications in oncology, infection/inflammation, and cardiac imaging. Hybrid PET/MRI may be employed as either focused regional imaging when both PET and diagnostic MRI are indicated, as a low-radiation alternative to WB PET/CT, or as a combination of focused regional imaging for tumor staging (T) and locoregional lymph nodes (N) and WB screening for distant metastatic disease (M).
The longer axial FOV allows faster multi-bed imaging. For example, a WB (vertex to mid femur) PET/MRI scan can be accomplished within 20 min or less with all-purpose MRI sequences such as Dixon T1, T2, and DWI (diffusion-weighted imaging). Such a minimal protocol may be comparable to PET with low-dose CT and applicable for screening or WB staging of diseases such as lymphoma [11]. A recurring concern for the use of PET/MRI for WB imaging is the lower sensitivity for detection of non-FDG-avid small lung nodules <1 cm with a detection rate reported as low as 12%, although with no impact on patient management in a per patient analysis [22]. The detection rate may be improved by adding Ultrashort Echo (UTE) or Zero Echo Time (ZTE) sequences and using respiratory gating, but at the expense of longer scanning. In the present study a single non-avid pulmonary nodule was not identified on MRI. A low-dose CT of the thorax three months later displayed a stationary benign-looking flat-shaped 7 mm calcification in the left lung.
Significant clinical value can be obtained using similar basic protocols that minimize radiation exposure or realize the full diagnostic potential of MRI when combined with focused regional MRI, e.g., in pelvic diseases or head–neck cancer as in the present study. Rather than simply combining standard MRI protocols with PET, MRI sequences should be designed to provide complementary diagnostic information, e.g., by improving anatomical information or by disqualifying benign [^18^F]FDG-avid lesions, while avoiding redundancy. The limitations of segmentation-based MRAC for the identification of bone (Figure 6) remain a concern for PET for the assessment of lesions adjacent to bone.
4.5. MRI
The clinical performance of the integrated MRI system is expected to be comparable to that of the current 3T MAGNETOM Vida. Although only fast protocols—shorter than our standard protocols—were utilized in this study, MRI still provided additional diagnostic value by revealing an occluded internal carotid artery in one patient and detecting additional brain metastases in another. The system was equipped with a 20-channel head/neck coil, and further improvements in image quality are anticipated with the planned implementation of a 32-channel coil.
The enhanced MRI capabilities may be particularly valuable in applications such as in epilepsy surgery planning, where high-quality MRI and PET are essential for the detection of subtle abnormalities such as heterotopias and cortical dysplasias.
4.6. Limitations
This study has several limitations and does not constitute a formal validation of the system’s clinical performance. Rather, it serves as an early indication of its potential and highlights issues to be addressed following CE approval for clinical use. Sequential imaging may have introduced bias in perceived image quality due to improved signal-to-background contrast in delayed acquisitions, despite lower count density resulting from isotope decay. Additionally, selection bias may have occurred as the study population included relatively healthier patients. Finally, comparisons were limited to systems from the same vendor, and no evaluation against PET/CT or PET/MRI platforms from other manufacturers was performed.
5. Conclusions
The BIOGRAPH One PET/MRI system demonstrates strong potential for delivering state-of-the-art PET imaging quality comparable to current PET/CT systems, while expanding the range of possible clinical indications. Its advanced design may enable reductions in either scan time or administered activity relative to its predecessor, improving efficiency and patient safety. MRI-based attenuation correction remains a critical area of focus of attention for accurate PET quantification.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Delso G. Furst S. Jakoby B. Ladebeck R. Ganter C. Nekolla S.G. Schwaiger M. Ziegler S.I. Performance measurements of the Siemens m MR integrated whole-body PET/MR scanner J. Nucl. Med.2011521914192210.2967/jnumed.111.09272622080447 · doi ↗ · pubmed ↗
- 2Drzezga A. Souvatzoglou M. Eiber M. Beer A.J. Furst S. Martinez-Moller A. Nekolla S.G. Ziegler S. Ganter C. Rummeny E.J. First clinical experience with integrated whole-body PET/MR: Comparison to PET/CT in patients with oncologic diagnoses J. Nucl. Med.20125384585510.2967/jnumed.111.09860822534830 · doi ↗ · pubmed ↗
- 3Singnurkar A. Poon R. Metser U. Head-to-Head Comparison of the Diagnostic Performance of FDG PET/CT and FDG PET/MRI in Patients with Cancer: A Systematic Review and Meta-Analysis AJR Am. J. Roentgenol.2024223 e 243151910.2214/AJR.24.3151939016450 · doi ↗ · pubmed ↗
- 4Mirshahvalad S.A. Kohan A. Metser U. Hinzpeter R. Ortega C. Farag A. Veit-Haibach P. Diagnostic performance of whole-body [18F]FDG PET/MR in cancer M staging: A systematic review and meta-analysis Eur. Radiol.20243467368510.1007/s 00330-023-10009-337535156 · doi ↗ · pubmed ↗
- 5Virarkar M. Ganeshan D. Devine C. Bassett R.Jr. Kuchana V. Bhosale P. Diagnostic value of PET/CT versus PET/MRI in gynecological malignancies of the pelvis: A meta-analysis Clin. Imaging 202060536110.1016/j.clinimag.2019.11.01831864201 · doi ↗ · pubmed ↗
- 6Al-Ibraheem A. Abdlkadir A. Herrmann K. Bomanji J. Jadvar H. Shi H. Mansour A. Paez D. Chiti A. Scott A.M. Diagnostic Accuracy of [18F]FDG PET/MRI in Head and Neck Squamous Cell Carcinoma: A Systematic Review and Metaanalysis J. Nucl. Med.2024651533153910.2967/jnumed.124.26804939266291 · doi ↗ · pubmed ↗
- 7Ling S.W. de Jong A.C. Schoots I.G. Nasserinejad K. Busstra M.B. van der Veldt A.A.M. Brabander T. Comparison of 68Ga-labeled Prostate-specific Membrane Antigen Ligand Positron Emission Tomography/Magnetic Resonance Imaging and Positron Emission Tomography/Computed Tomography for Primary Staging of Prostate Cancer: A Systematic Review and Meta-analysis Eur. Urol. Open Sci.202133617110.1016/j.euros.2021.09.00634632423 PMC 8488242 · doi ↗ · pubmed ↗
- 8Shen F. Liu Q. Wang Y. Chen C. Ma H. Comparison of [18F] FDG PET/CT and [18F]FDG PET/MRI in the Detection of Distant Metastases in Breast Cancer: A Meta-Analysis Clin. Breast Cancer 202525 e 113e 123.e 410.1016/j.clbc.2024.09.01539438190 · doi ↗ · pubmed ↗