Cytokines in patients with Posner-Schlossman syndrome
Yu Liu, Shengjie Li, Xiangmei Kong, Qilian Sheng, Zhujian Wang, Wenjun Cao

TL;DR
This study found elevated inflammatory cytokines in the eye fluid of Posner-Schlossman syndrome patients, suggesting immune involvement and potential biomarkers for diagnosis.
Contribution
The study identifies specific cytokine profiles in PSS and their correlation with clinical parameters, offering new insights into disease mechanisms and diagnostics.
Findings
IL-1β, IL-6, IL-10, and IFN-γ levels were significantly higher in PSS compared to controls and POAG.
IL-6 levels correlated with intraocular pressure and corneal endothelial cell loss in PSS patients.
Cytokine profiles showed diagnostic potential for differentiating PSS from POAG.
Abstract
To investigate the inflammatory cytokine profiles in the aqueous humor (AH) of patients with Posner-Schlossman syndrome (PSS) and evaluate their correlations with key ophthalmic parameters. Aqueous humor samples were collected from 31 eyes with PSS, 26 eyes with primary open-angle glaucoma (POAG), and 20 eyes with age-related cataract (ARC, control group) at the Eye and ENT Hospital of Fudan University. A multiplex bead-based flow cytometric immunoassay was performed to quantify the concentrations of interleukins (IL-1β, IL-2, IL-4, IL-5, IL-6, IL-8, IL-10, IL-12, IL-17), tumor necrosis factor-alpha (TNF-α), and interferons (IFN-α, IFN-γ). Simultaneously, the presence of cytomegalovirus (CMV) DNA in PSS samples was assessed by PCR. Clinical data including corneal endothelial cell density, visual acuity, intraocular pressure (IOP), and visual field were also recorded. The AH levels of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
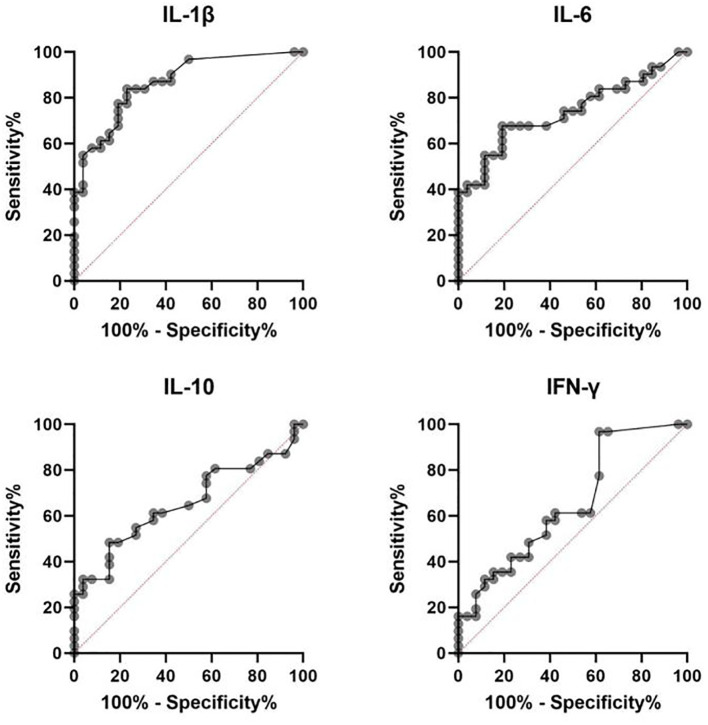 Figure 1
Figure 1| Factors | Groups | ||
|---|---|---|---|
| Control | PSS | POAG | |
| No. of eyes | 20 | 31 | 26 |
| Age (years) | 54.4 ± 9.7 | 50.1 ± 12.5 | 55.5 ± 12.8 |
| – | 0.2058 | 0.7310 | |
| 0.2058 | – | 0.1122 | |
| Male:female | 12:8 | 19:12 | 19:7 |
| – | 0.9273 | 0.3535 | |
| 0.9273 | – | 0.3512 | |
| IOP (mmHg) | 13.8 ± 1.8 | 32.9 ± 9.9 | 28.2 ± 7.3 |
| – | <0.0001 | <0.0001 | |
| <0.0001 | – | 0.0534 | |
| Cytokines | Control n= 20 | PSS n =31 | POAG n =26 | |||
|---|---|---|---|---|---|---|
|
|
|
| ||||
| IL- 1β | 1.75 (0.53,2.46) | 8.96 (4.89,13.69) | 0.77 (0.53,3.14) | <0.0001* | 0.6622 | <0.0001* |
| IL-5 | 1. 14 (1.07,1.93) | 2.04 (1.57,2.72) | 1.65 (1.14,2.47) | 0.0005* | 0.1580 | 0.0818 |
| IL-6 | 2. 77 (1.60,3.75) | 28.10 (4.30,419.47) | 4.34 (2.99,6.23) | <0.0001* | 0.0114* | 0.0020* |
| IL-8 | 16.35 (8.79,23.45) | 117.87 (87.07,245.23) | 114.43 (87.75,144.60) | <0.0001* | <0.0001* | 0.2620 |
| IL- 10 | 1.12 (1.07,1.35) | 1.63 (1.39,2.25) | 1.45 (1.29,1.63) | 0.0001* | 0.0021* | 0.0338* |
| IL- 17 | 2.88 (1.82,3.90) | 3.16 (2.50,4.44) | 2.51 (2.28,3.54) | 0.1049 | 0.8592 | 0.0515 |
| IFN-γ | 2.42 (2.08,2.68) | 3.91 (2.42,7.93) | 2.55 (1.14,4.23) | 0.0159* | 0.5994 | 0.0445* |
| TNF-α | 1.82 (1.42,2.36) | 2.91 (2.44,21.38) | 6.70 (2.18,29.06) | <0.0001* | <0.0001* | 0.9553 |
| Cytokines | AUC | 95% CI | Youden’s index | Cutoff | Sensitivity | Specificity | |
|---|---|---|---|---|---|---|---|
| IL- 1β | 0.867 | 0.750 - 0.942 | <0.001 | 0.608 | 3.14 | 83.87 | 76.92 |
| IL-6 | 0.739 | 0.606 - 0.846 | 0.0003 | 0.485 | 7.46 | 67.74 | 80.77 |
| IL- 10 | 0.654 | 0.516 - 0.775 | 0.0359 | 0.330 | 1.64 | 48.39 | 84.62 |
| IFN-γ | 0.655 | 0.517 - 0.776 | 0.0036 | 0.496 | 1.34 | 96.77 | 38.46 |
| Aqueous humor cytokines of PSS | Gender (males | Age (<50 | Cataract (with | CMV-DNA (+ |
|---|---|---|---|---|
| IL- 1β | 0.187 | 0.920 | 0.088 | 0.736 |
| IL-5 | 0.670 | 0.857 | 0.632 | 0.921 |
| IL-6 | 0.078 | 0.378 | 0.447 | 0.843 |
| IL-8 | 0.935 | 0.337 | 0.708 | 0.620 |
| IL- 10 | 0.584 | 0.214 | 0.417 | 0.487 |
| IL- 17 | 0.273 | 0.631 | 0.662 | 0.170 |
| TNF- α | 0.919 | 0.496 | 0.130 | 0.858 |
| IFN-γ | 0.463 | 0.334 | 0.490 | 0.247 |
| Ocular parameters result Mean ± SD/Median (Interquartile Range) | IL- 1β | IL-5 | IL-6 | IL-8 | IL- 10 | IL- 17 | TNF-α | IFN-γ | |
|---|---|---|---|---|---|---|---|---|---|
| Visual Acuity(LogMAR) | 0.071 | 0.361 | 0.074 | 0.047 | -0.080 | 0.254 | -0.039 | 0.263 | |
| 0.704 | 0.083 | 0.692 | 0.804 | 0. 669 | 0.168 | 0.836 | 0.160 | ||
| IOP(mmHg) | -0.139 | 0.198 |
| 0.294 | 0.193 | -0.251 | 0.134 | -0.003 | |
| 0.455 | 0.287 |
| 0.109 | 0.298 | 0.173 | 0.473 | 0.989 | ||
| Cup-to-Disc Ratio | -0.213 | -0. 112 | -0.082 | -0.148 | -0.180 | 0.085 | 0.238 | -0.196 | |
| 0.354 | 0.629 | 0.723 | 0.521 | 0.436 | 0.715 | 0.298 | 0.396 | ||
| Axial length (mm) | -0.147 | -0.128 | 0.014 | 0.117 | 0.024 | -0.035 | 0.055 | 0.050 | |
| 0.464 | 0.525 | 0.945 | 0.560 | 0.905 | 0.862 | 0.785 | 0.803 | ||
| MD(dB) | -0.052 | 0.012 | 0.310 | 0. 141 | -0.101 | -0.027 | -0.029 | 0.100 | |
| 0.799 | 0.951 | 0.116 | 0.482 | 0.616 | 0.893 | 0.886 | 0.620 | ||
| MS(dB) | 0. 121 | 0.131 | -0.076 | -0.060 | 0.047 | -0.115 | -0.149 | -0.207 | |
| 0.557 | 0.525 | 0.712 | 0.770 | 0.819 | 0.576 | 0.469 | 0.311 | ||
| CECD(cell/mm2) | -0.156 | -0.057 | -0.379 | -0.353 | -0.145 | -0.239 | 0.034 | -0.161 | |
| 0.499 | 0.805 | 0.074 | 0.116 | 0.531 | 0.297 | 0.882 | 0.485 | ||
| RECL(cell/mm2) | -0.043 | -0.302 |
| 0.004 | -0.280 | 0.194 | -0.303 | 0.113 | |
| 0.853 | 0.184 |
| 0. 987 | 0.220 | 0.400 | 0.182 | 0.625 | ||
| Aqueous humor cytokines | IL- 1β | IL-5 | IL-6 | IL-8 | IL- 10 | IL- 17 | TNF-α | IFN-γ | |
|---|---|---|---|---|---|---|---|---|---|
| IL- 1β | – | -0.122 | 0.125 | -0.039 | 0.023 |
|
| -0.092 | |
| – | 0.514 | 0.504 | 0.835 | 0. 904 |
|
| 0.621 | ||
| IL-5 | -0.122 | – | 0.083 | 0.009 | 0.340 | -0.229 | 0.190 |
| |
| 0.514 | – | 0.657 | 0.961 | 0.061 | 0.215 | 0.305 |
| ||
| IL-6 | 0.125 | 0.083 | – | 0.688 |
| -0.029 | -0.041 | 0.273 | |
| 0.504 | 0.657 | – |
|
| 0.876 | 0.825 | 0.138 | ||
| IL-8 | -0.039 | 0.009 |
| – |
| -0.171 | 0.097 |
| |
| 0.835 | 0.961 |
| – |
| 0.359 | 0.603 |
| ||
| IL-10 | 0.023 | 0.340 |
|
| – | 0.034 | 0.166 | 0.121 | |
| 0. 904 | 0.061 |
|
| – | 0.855 | 0.373 | 0.517 | ||
| IL-17 |
| -0.229 | -0.029 | -0.171 | 0.034 | – | -0.208 | 0.027 | |
|
| 0.215 | 0.876 | 0.359 | 0.855 | – | 0.262 | 0.887 | ||
| TNF-α |
| 0.190 | -0.041 | 0.097 | 0.166 | -0.208 | – | 0.015 | |
|
| 0.305 | 0.825 | 0.603 | 0.373 | 0.262 | – | 0.934 | ||
| IFN-γ | -0.092 |
| 0.273 |
| 0.121 | 0.027 | 0.015 | – | |
| 0.621 |
| 0.138 |
| 0.517 | 0.887 | 0.934 | – | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Diseases and Behçet’s Syndrome · Retinal and Optic Conditions · Ophthalmology and Eye Disorders
Introduction
1
Posner-Schlossman syndrome (PSS), first described by Posner and Schlossman in 1948 (1), is a distinct subtype of secondary glaucoma characterized by recurrent episodes of unilateral elevated intraocular pressure (IOP) accompanied by mild anterior uveitis. The fellow eye typically exhibits normal IOP and no signs of inflammation. Clinically, PSS presents with episodic blurred vision, ocular discomfort or pain, and keratic precipitates (KPs) on slit-lamp examination. The syndrome predominantly affects males between 20 and 50 years of age (2). Though bilateral involvement—either simultaneous or alternating—has also been reported in some cases (3, 4).
PSS shares certain clinical features with primary open-angle glaucoma (POAG), particularly in the early stages, which can make differential diagnosis challenging. Atypical presentations or coexisting PSS and POAG further complicate diagnosis. The absence of disease-specific ocular lesions and validated biomarkers often leads to delayed diagnosis, hindering timely and targeted treatment. As the chronic, relapsing nature of PSS becomes increasingly recognized, its associated socioeconomic burden has prompted growing interest in identifying disease-specific biomarkers to support accurate diagnosis and personalized management strategies.
Despite decades of study, the pathogenesis of PSS remains incompletely elucidated. Prior research has suggested that persistent inflammatory responses within the anterior chamber may impair aqueous humor outflow, resulting in elevated IOP and secondary glaucomatous damage. Cytomegalovirus (CMV) infection has been frequently implicated as a contributing factor in this process (5–8). Simultaneously, multiple cytokines have been reported to participate in immune modulation and inflammatory signaling in glaucomatous diseases (9, 10). However, due to the complexity and redundancy of cytokine networks, their precise roles in PSS remain unclear. Therefore, a comprehensive profiling of inflammatory cytokines and their associations with clinical parameters is critical to understanding PSS pathogenesis and identifying potential diagnostic biomarkers.
In this study, we employed multiplex microsphere flow cytometric immunoassay to measure the levels of a panel of inflammatory cytokines in the aqueous humor of PSS patients and compared these profiles to those of POAG and cataract (control) patients. We further explored correlations between cytokine concentrations and ophthalmic indicators—including visual acuity, IOP, and corneal endothelial cell density—to evaluate their diagnostic potential and relevance to disease severity. These findings may lay the groundwork for the development of laboratory-based diagnostic tools and provide mechanistic insights into the immunopathogenesis of PSS.
Materials and methods
2
Study subjects
2.1
A total of 77 eyes from 77 patients were included in this study, comprising 31 eyes diagnosed with Posner-Schlossman syndrome (PSS), 26 with primary open-angle glaucoma (POAG), and 20 with age-related cataract (ARC, serving as controls). All participants were recruited from the Eye and ENT Hospital, Fudan University, between August 2022 and November 2024. Patients in the control group exhibited no signs of ocular pathology upon comprehensive ophthalmic examination and had intraocular pressure (IOP) values below 21 mmHg.
All participants enrolled in this study were carefully screened and confirmed to have no underlying systemic diseases (e.g., diabetes, autoimmune disorders, cardiovascular diseases, etc.). Furthermore, all samples were collected prior to the initiation of any study-related or relevant medications, ensuring that the sample status reflected the natural history of the condition under investigation without pharmacological confounding. In patients with PSS, aqueous humor sampling was performed during an active episode characterized by elevated intraocular pressure and mild anterior chamber inflammation, but before the initiation of treatment, to ensure that cytokine profiles reflected the intrinsic inflammatory status of the disease.
The diagnosis of PSS was based on the following criteria: (1) recurrent unilateral episodes of elevated IOP (>21 mmHg) with spontaneous return to normal between episodes; (2) mild anterior chamber inflammation, characterized by fine keratic precipitates on slit-lamp examination; (3) open iridocorneal angle confirmed by gonioscopy; and (4) a healthy fellow eye with normal IOP, visual field, and optic disc morphology (11). POAG diagnosis was established according to standard criteria, including an open iridocorneal angle, documented history of elevated IOP prior to anti-glaucoma treatment, and exclusion of secondary glaucoma.
The study protocol adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Ethics Committee of the Eye and ENT Hospital, Fudan University. Written informed consent was obtained from all participants.
Reagents and instruments
2.2
A 12-plex human cytokine detection kit (Catalog No. 191217) was purchased from Hangzhou R&D Biological Technology Co., Ltd. Inflammatory cytokines in aqueous humor—including IL-1β, IL-2, IL-4, IL-5, IL-6, IL-8, IL-10, IL-12, IL-17, TNF-α, IFN-α, and IFN-γ—were measured using a bead-based multiplex flow cytometry immunoassay. The procedure employed a microsphere-based sandwich immunofluorescence technique, integrated with enzyme-linked immunosorbent assay (ELISA) principles.
Qualitative polymerase chain reaction (PCR) for CMV DNA detection was performed using a TaqMan PCR kit (Shanghai ZJ BioTech Co., Ltd., China) on an ABI 7500 real-time PCR system (Thermo Fisher Scientific, Waltham, MA, USA).
Sample collection
2.3
Aqueous humor samples (100 μL each) were obtained via anterior chamber paracentesis prior to any intraocular surgery or pharmacological treatment. All samples were collected under aseptic conditions and immediately stored at –80 °C until analysis.
Collection of ocular clinical parameters
2.4
Visual Acuity: Visual acuity was measured using an international logMAR visual acuity chart. Visual Field Examination: Visual fields were measured using an Octopus 900 automated perimeter. Corneal Endothelial Cell Density: Corneal endothelial cell density was measured using a corneal endothelial microscope (NSP-9900II).
Statistical analysis
2.5
Data analysis was conducted using IBM SPSS Statistics 21.0. The Shapiro–Wilk test was used to assess normality. For normally distributed variables, results are expressed as mean ± standard deviation (SD), and comparisons between groups were made using independent-sample t-tests. Non-normally distributed variables are presented as median with interquartile range [IQR], and analyzed using the Mann–Whitney U test. Categorical variables were compared using Fisher’s exact test.
Spearman’s rank correlation analysis was performed to evaluate associations between cytokine concentrations and clinical parameters (e.g., IOP, CECD, visual field). Correlation strength was defined as: strong (|r| ≥ 0.8), moderate (|r| = 0.5–0.8), weak (|r| = 0.3–0.5), and negligible (|r| < 0.3). A P-value <0.05 was considered statistically significant. Given the exploratory nature of this study and the biological correlations among cytokines, formal correction for multiple comparisons was not applied. The findings should therefore be interpreted with caution and viewed as hypothesis-generating.
Receiver operating characteristic (ROC) curves were generated using MedCalc 19.6 (MedCalc Software Ltd., Ostend, Belgium) to assess the diagnostic performance of candidate cytokines. For ROC curve analyses, optimal cutoff values were determined using Youden’s index, defined as sensitivity + specificity − 1.
Results
3
Demographic and clinical characteristics
3.1
Table 1 summarizes the demographic and preoperative clinical characteristics of the study population. There were no statistically significant differences in age or gender distribution among the PSS, POAG, and control groups (P > 0.05). Both the PSS and POAG groups exhibited significantly elevated intraocular pressure (IOP) compared with controls (P < 0.0001), while the IOP difference between PSS and POAG groups was not statistically significant (P = 0.0534).
Cytokine profiles in aqueous humor
3.2
Among the 12 measured cytokines, IL-2, IL-4, IL-12, and IFN-α were below the lower limit of detection in the majority of samples across all three groups and were therefore excluded from subsequent quantitative analyses.
As shown in Table 2, the levels of IL-1β, IL-5, IL-6, IL-8, IL-10, IFN-γ, and TNF-α in the aqueous humor of PSS patients were significantly higher than those in the cataract control group (P < 0.05). Furthermore, IL-1β, IL-6, IL-10, and IFN-γ levels were also significantly elevated in PSS compared to POAG eyes (P < 0.05), while IL-5 and TNF-α showed no significant differences between the two.
Diagnostic performance of selected cytokines
3.3
Receiver operating characteristic (ROC) curve analysis was conducted to assess the potential discriminatory ability of IL-1β, IL-6, IL-10, and IFN-γ in differentiating PSS from POAG. The results are presented in Table 3 and Figure 1.
ROC curves of the four cytokines between PSS and POAG patients.
Among the cytokines analyzed, IL-1β demonstrated the highest diagnostic performance, with an area under the curve (AUC) of 0.867 (95% CI: 0.750–0.942), sensitivity of 83.87%, and specificity of 76.92% at a cutoff of 3.14 pg/mL. IL-6 also showed moderate discriminative value (AUC = 0.739), followed by IFN-γ and IL-10.
Cytokine profiles stratified by clinical subgroups
3.4
Stratified analyses based on sex, age, presence of coexisting cataract, and CMV DNA status revealed no significant differences in aqueous humor cytokine levels among PSS subgroups (Table 4, all P > 0.05).
Among the 31 PSS patients, 17 (54.8%) tested positive for CMV DNA in aqueous humor by PCR. However, no statistically significant differences were observed in cytokine concentrations between CMV-positive and CMV-negative individuals (Table 4).
Correlation between cytokines and ophthalmic parameters
3.5
Correlation analysis between cytokine levels and ophthalmic measurements in the PSS group revealed that IL-6 was significantly and positively correlated with IOP (r = 0.395, P = 0.007) and relative endothelial cell loss (RECL; r = 0.453, P = 0.039) (Table 5). No other cytokines showed statistically significant correlations with CECD, visual field indices, or axial length. In multivariable regression analyses adjusted for age, sex, and intraocular pressure, IL-6 remained significantly associated with intraocular pressure and relative endothelial cell loss.
Inter-cytokine correlation analysis
3.6
Spearman’s rank correlation analysis revealed a complex cytokine regulatory network within the aqueous humor of patients with Posner-Schlossman syndrome (PSS) (Table 6). IL-6 exhibited strong positive correlations with both IL-8 (r = 0.688, P < 0.0001) and IL-10 (r = 0.487, P = 0.006), suggesting coordinated upregulation among these inflammatory mediators. Similarly, IL-8 was positively correlated with IL-10 (r = 0.506, P = 0.004) and IFN-γ (r = 0.404, P = 0.024), showing a significant positive correlation, which is consistent with (or may reflect) coordinated expression within a shared inflammatory pathway. IL-1β showed a positive correlation with IL-17 (r = 0.457, P = 0.010), but was negatively correlated with TNF-α (r = –0.491, P = 0.005), IL-1β levels showed a significant positive correlation with IL-17 and a significant negative correlation with TNF-α. This pattern of correlations suggests a complex, non-linear regulatory network among these cytokines in PSS, rather than a simple linear association. Additionally, IL-5 was negatively correlated with IFN-γ (r = –0.440, P = 0.013), reflecting a potential counterbalance between Th2- and Th1-type immune responses. Collectively, these findings highlight the intricate and dynamic cytokine interactions that may underlie the immunopathogenesis of PSS.
Discussion
This study delineates a unique inflammatory cytokine profile in the aqueous humor (AH) of patients with Posner-Schlossman syndrome (PSS), distinct from profiles in primary open-angle glaucoma (POAG) and cataract controls. Our findings underscore a central role for immune dysregulation in PSS pathogenesis.
Elevated levels of IL-1β, IL-6, IL-10, and IFN-γ in PSS AH were significant. Notably, in ROC analysis, these cytokines effectively discriminated PSS from POAG, highlighting their potential as diagnostic biomarkers in clinically ambiguous cases.
Approximately 55% of AH samples were CMV PCR-positive, yet cytokine levels did not differ significantly between PCR-positive and PCR-negative groups, aligning with prior findings (6). A negative PCR result does not exclude latent CMV infection, and the precise role of CMV—as an inflammatory activator or a bystander—in PSS remains to be defined. Therefore, there was no significant difference in cytokines between the CMV-positive group and the CMV-negative group.
The significant elevation of IL-1β, coupled with its positive correlation with IL-17 in PSS AH, is consistent with the involvement of Th17-mediated pathways—an underexplored mechanism in PSS. Given that IL-1β is a critical cytokine for the differentiation and functional regulation of human Th17 cells (12) and points to a pathway for chronic anterior chamber inflammation that extends beyond the classical Th1/Th2 imbalance.
IL-6 was notably elevated and demonstrated positive correlations with both intraocular pressure (IOP) and relative endothelial cell loss (RECL). This dual association supports the interpretation of IL-6 as a potential link between inflammatory activity and tissue damage, a concept corroborated by studies in related ocular conditions (8, 13). The co-elevation of IL-6, IL-8, and IL-10 reflects a coordinated, complex immune response within the anterior chamber.
IL-10 is secreted by TH2 cells (14). The rise in the anti-inflammatory cytokine IL-10 is consistent with a compensatory mechanism to modulate ongoing inflammation, potentially in response to viral triggers such as CMV (15, 16).Similarly, elevated IFN-γ levels, along with a negative correlation with IL-5, are indicative of a dominant Th1 response that could suppress Th2 activity in PSS, aligning with patterns observed in other infectious uveitides (17–19).
While TNF-α was elevated in both PSS and POAG, affirming its general association with glaucomatous processes (20–22), its negative correlation with IL-1β specifically in PSS implies a unique regulatory interaction within the PSS cytokine network that warrants further study.
This study is limited by a modest sample size, a consequence of PSS’s low incidence and recurrent nature, compounded by stringent inclusion and technical criteria. The lack of formal multiple-comparison correction represents a limitation of this exploratory study and warrants validation in larger, independent cohorts. Future multicenter studies employing more sensitive, high-throughput techniques are needed to validate these cytokine profiles and systematically explore their roles as biomarkers in PSS. It should be noted that despite statistically significant differences, considerable overlap in cytokine levels exists between PSS and POAG patients. Therefore, single-cytokine thresholds are unlikely to function as standalone diagnostic tools in clinical practice. Instead, these findings highlight cytokines that may contribute to differential disease profiling and could be incorporated into future multi-parameter or integrative diagnostic models.
Conclusion
Our study found significantly increased levels of inflammatory factors such as IL-1β, IL-6, IL-10, IFN-γ in the aqueous humor of PSS patients, indicating that these molecules undergo significant changes in the aqueous humor of PSS and may be closely related to ocular lesions. The cytokines IL-6 in the aqueous humor exhibited a significant positive correlation with PSS key ophthalmic parameters, suggesting a potential relationship between ocular lesions and immune responses and inflammation in PSS patients. In general, there seems to be a stronger cytokine response in PSS than POAG, and the inflammation was promoted by a strong TH1 response in PSS. Further investigation into the role of cytokines and the balanced regulation of TH1/TH2/TH17 in the pathogenesis of PSS could provide novel perspectives and potential avenues for disease treatment and intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Posner A Schlossman A . Syndrome of unilateral recurrent attacks of glaucoma with cyclitic symptoms Arch Ophthal(1948);39:517–535doi:10.1001/archopht.1948.00900020525007, PMID: 18123283 · doi ↗ · pubmed ↗
- 2Jiang JH Zhang SD Dai ML Yang JY Xie YQ Hu C . Posner-Schlossman syndrome in Wenzhou, China: a retrospective review study Br J Ophthalmol(2017);101:1638–1642 doi:10.1136/bjophthalmol-2016-309863, PMID: 28450379 · doi ↗ · pubmed ↗
- 3Hess LK Lee GA Shah P . Bilateral simultaneous presentation of Posner-Schlossman syndrome Clin Exp Ophthalmol(2017);45:925–927doi:10.1111/ceo.12981, PMID: 28486785 · doi ↗ · pubmed ↗
- 4Jap A Sivakumar M Chee SP . Is Posner-Schlossman syndrome benign? Ophthalmology(2001);108:913–918doi:10.1016/s 0161-6420(01)00551-6, PMID: 11320022 · doi ↗ · pubmed ↗
- 5Bai W Huang X Shen X Ye Y Peng S Zhu T . HSP 70 and TNF Loci Polymorphism Associated with the Posner-Schlossman Syndrome in a Southern Chinese Population J Immunol Res(2022);2022:5242948 doi:10.1155/2022/5242948, PMID: 36530572 PMC 9757935 · doi ↗ · pubmed ↗
- 6Li J Ang M Cheung CM Vania M Chan AS Waduthantri S . Aqueous cytokine changes associated with Posner-Schlossman syndrome with and without human cytomegalovirus P Lo S One(2012);7:e 44453 doi:10.1371/journal.pone.0044453, PMID: 23028541 PMC 3441587 · doi ↗ · pubmed ↗
- 7Igarashi N Honjo M Kaburaki T Aihara M . Effects of ROCK Inhibitors on Apoptosis of Corneal Endothelial Cells in CMV-Positive Posner-Schlossman Syndrome Patients Invest Ophthalmol Vis Sci(2020);61:5doi:10.1167/iovs.61.10.5, PMID: 32749463 PMC 7441372 · doi ↗ · pubmed ↗
- 8Li J Ji Y Yang W Yao Y Wang S Zhang Z . Analysis of risk factors associated with secondary open-angle glaucoma in Posner-Schlossman syndrome: A retrospective case-control study Front Med (Lausanne)(2023);9:1064449 doi:10.3389/fmed.2022.1064449, PMID: 36698797 PMC 9868410 · doi ↗ · pubmed ↗