Defining prerequisites for optimising outcomes of shoulder arthrodesis in post-traumatic brachial plexus palsy
G. Mithun Pai, Anil K Bhat, Ashwath M. Acharya, Kishore Vellingiri

TL;DR
This study identifies key factors for successful shoulder arthrodesis in patients with post-traumatic brachial plexus palsy.
Contribution
The study defines prerequisites for optimal outcomes after shoulder arthrodesis in brachial plexus palsy.
Findings
All patients achieved radiological union with significant pain relief within 8.5 months.
Patients with intact or reanimated periscapular muscles had better functional outcomes.
Shoulder arthrodesis provides reliable pain relief and functional stability in brachial plexus palsy.
Abstract
Persistent pain, joint subluxation, instability, and limited shoulder mobility present significant reconstructive challenges in post-traumatic brachial plexus injury. This study aims to determine the essential prerequisites for attaining optimal functional results after shoulder arthrodesis in patients with post-traumatic brachial plexus palsy. Between 2017 and 2023, ten patients underwent shoulder arthrodesis, five with upper plexus palsy (mean age 35 years) and five with global palsy (mean age 31 years). The preoperative assessment included an evaluation of the integrity of the periscapular muscles. Arthrodesis was performed using a 3.5-mm locking reconstruction plate, positioning the shoulder in 30° forward flexion, 30° abduction, and 30° internal rotation. Patients were followed for a mean of 30 months, and outcomes were assessed in terms of radiological union, range of motion in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
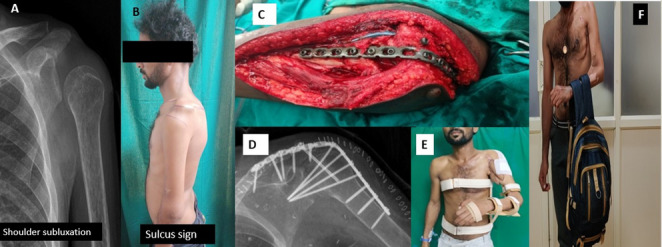 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3- —Manipal Academy of Higher Education, Manipal
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNerve Injury and Rehabilitation · Pain Management and Treatment · Cerebral Palsy and Movement Disorders
Introduction
Restoring shoulder function remains a paramount objective in managing post-traumatic brachial plexus injury. Various surgical procedures, such as nerve reconstruction, tendon transfers, and shoulder arthrodesis, have been documented to improve stability and functionality of the shoulder. Among these, shoulder arthrodesis serves as a crucial, time-tested procedure in situations of persistent and profound paralysis, where alternative reconstruction offers limited advantages. It optimizes the resting position of the paralyzed shoulder, thereby improving spatial awareness and supporting compensatory movements. [1, 2] Glenohumeral arthrodesis results in pain alleviation and enhances scapulothoracic coordination [1]. A stable shoulder joint is crucial for optimal distal limb function; however, the effectiveness of arthrodesis in stabilizing a flail shoulder continues to be a subject of debate [3].
Nerve reconstruction procedures are reported to yield less predictable results for shoulder reanimation compared to the elbow, due to the joint’s intricate biomechanics. [4] The transfer of the trapezius alone could result in an awkward proximal displacement of the humeral head [5]. This resulted in mechanical impingement with a reduced trapezius lever arm, leading to suboptimal shoulder abduction and flexion [5, 6]. Although considerable gains in flexion and abduction were observed, the transfer often did not seem to resolve the external rotation insufficiency [6]. Enhancing shoulder external rotation should be considered with equal importance, as it enables patients to position their hand in front of their body, which often necessitates additional tendon transfers [3].
Despite advancements in tendon transfer procedures, residual impairments frequently persist, underscoring the importance of shoulder arthrodesis in achieving functional outcomes related to stability, pain relief, and facilitating clinically significant functions, such as the brachiothoracic grasp, particularly in cases of global palsy [7]. Although most literature on shoulder arthrodesis in brachial plexus palsy primarily emphasizes postoperative functional outcomes [8, 9], only a limited number of studies have explored the critical preoperative factors required to attain optimal results [10]. The primary objective of this study was to identify preoperative clinical factors that contribute to favourable functional outcomes after shoulder arthrodesis, with a particular focus on parascapular muscle function and optimal arthrodesis positioning. We hypothesized that the preservation of parascapular muscle function is associated with improved postoperative functional outcomes and that patients with upper plexus palsy demonstrate improved functional results following shoulder arthrodesis compared to those with global plexus palsy.
Methodology
Based on the extent of the injury, patients were categorized into two groups: upper plexus palsy involving the C5–C6 or C5–C7 roots, and global palsy involving the C5–T1 roots. A total of 10 male patients with a mean age of 33.6 years (range, 23–65 years) underwent shoulder arthrodesis for post-traumatic brachial plexus palsy between January 2017 and December 2023 at our tertiary care referral centre. Among them, five had upper plexus palsy, and five had global palsy. Before arthrodesis, all patients had undergone various reconstructive procedures, including nerve transfers (e.g., intercostal to biceps, spinal accessory to suprascapular, Oberlin transfer), muscle transfers (e.g., gracilis for elbow flexion, latissimus dorsi to infraspinatus), or interfascicular nerve grafting. The primary indication for shoulder arthrodesis was a double-level suprascapular nerve injury in conjunction with axillary nerve involvement, in patients where no further nerve transfer or primary reconstruction was feasible, typically beyond 12 months post-injury, and who presented with a painful inferior glenohumeral subluxation (Fig. 1A, B). Institutional ethical clearance was obtained, and informed consent was obtained from all participants prior to the functional assessment.
Fig. 1A patient with global brachial plexus palsy and an unstable shoulder. A Preoperative radiograph showing inferior subluxation of the humeral head. B Clinical photograph demonstrating a positive sulcus sign. C Intraoperative exposure of the shoulder with implant placement. D Postoperative radiograph showing screw configuration following arthrodesis. E Splint immobilization in the desired functional position. F One-year follow-up demonstrating regained shoulder stability
Surgical technique
The patient was placed in the beach-chair position under general anesthesia, and a standard deltopectoral approach was used to expose the glenohumeral joint (Fig. 1C). The articular cartilage of the glenoid, humeral head, and undersurface of the acromion was completely denuded to create raw, bleeding surfaces for bone-to-bone fusion—preoperative planning aimed for stable fixation with compression across both the glenohumeral and acromiohumeral joints. A 3.5 mm locking reconstruction plate was contoured and fixed laterally from the humeral shaft to the acromion and scapular spine, with at least four screws across the arthrodesis site. Additional fixation was provided by a 6.5 mm fully threaded cancellous screw passed transarticularly into the glenohumeral joint and, where feasible, a long-cannulated screw from the lateral acromion into the proximal humerus to assist acromiohumeral fusion (Fig. 1C, D). Corticocancellous bone graft harvested from the greater tuberosity, acromion, and/or coracoid was packed into the fusion bed to augment union. The shoulder was positioned in the functional 30° abduction, 30° flexion, and 30° internal rotation to optimize activities such as hand-to-mouth and midline reach before final tightening of the construct. Postoperatively, the limb was immobilized in a custom-moulded 30°–30°−30° splint for six weeks, followed by an arm sling and a structured rehabilitation program focusing on scapulothoracic mobility and periscapular muscle strengthening (Fig. 1E).
Outcome assessment
Postoperative active shoulder abduction, forward flexion (protraction), and external rotation(retraction) were assessed clinically. Abduction angle and forward flexion (protraction) were measured in the frontal plane using the long axis of the humerus and the cervicothoracic spine forming the two limbs of the goniometer. External rotation was measured in the transverse plane with the elbow flexed to 90°, referencing the long axis of the forearm to a transverse limb of the goniometer that was parallel to the upper trunk [1]. We also included brachiothoracic grasp, which is assessed by observing the patient’s ability to stabilize objects between the upper arm and thoracic wall using scapulothoracic and elbow motion [10]. In addition, we assessed the ability to bring the hand to the mouth and rest on the belly, pain assessment using the Visual Analog Scale (VAS)[11], and patient-reported outcome measures using the DASH (Disabilities of the Arm, Shoulder, and Hand) score[12]. The motor status of the parascapular muscles were assessed clinically in each patient using standardized manual muscle testing to determine its impact on the outcome [13]. All measurement were assessed by two fellowship-trained upper limb surgeons with more than five years of experience.
Statistical analysis
The mean and range for each variable were reported to summarize central tendencies and dispersion. To evaluate the differences in outcomes between patients with upper and pan-brachial plexus palsy, a combination of descriptive and inferential statistical methods was applied. Continuous variables, such as shoulder abduction, protraction, retraction, time to union, DASH scores (Disabilities of the Arm, Shoulder, and Hand), and VAS scores (Visual Analogue Scale for pain), were compared between the two groups using independent t-tests.
Results
Patients (1–5) with upper brachial plexus palsy were predominantly young adults (age range, 23–65 years), with the right dominant upper limb affected in three cases (Table 1).
Table 1. The demographics of patients with brachial plexus injuries who underwent shoulder arthrodesisPatientAgeGenderSideInjury to the 1st surgery (month)Ist surgery to arthrodesis (month)Primary surgeryReason for shoulder fusionFinal follow-up (month) Upper brachial plexus palsy 128MaleRight34OberlinDouble-level lesion (Suprascapular + Axillary nerve involvement)16223MaleLeft27Musculocutaneous nerve neurolysisDouble-level lesion (Suprascapular + Thinned axillary nerve)12365MaleRight5 (elsewhere)24Intercostal nerve to Musculocutaneous (Elsewhere)Time since injury > 1 year (not amenable to repair)12426MaleRight126Latissimus dorsi to BicepsTime since injury > 1 year (not amenable to repair)30540MaleLeft726Latissimus dorsi to Biceps + SteindlerTime since injury > 1 year (not amenable to repair)28 Global brachial plexus palsy 632MaleRight67Intercostal→Musculocutaneous, Intercostal→Pectoral, Free Gracilis (SAN)Non-availability of nerve donors72736MaleRight66Intercostal→Musculocutaneous, Intercostal→Pectoral, Free Gracilis (SAN)Non-availability of nerve donors14828MaleRight74Functioning Free Gracilis Transfer (SAN)Time since injury > 1 year (not amenable to nerve repair)36931MaleRight78Contralateral C7→Lower trunk, Free Gracilis Transfer (SAN)Non-availability of nerve donors361027MaleRight26Intercostal→Musculocutaneous, Intercostal→Pectoral, Free Gracilis (SAN)Non-availability of nerve donors36
The median interval from injury to first surgical intervention was approximately 5 months (range, 2–72 months), while the mean duration between the first Surgery and shoulder fusion was notably longer, averaging 11.8 months (range, 6–24 months). This delay likely reflects the period allowed for recovery following nerve reconstructions or muscle transfers. Initial reconstructive procedures varied and included Oberlin transfer, musculocutaneous nerve neurolysis, intercostal-to-musculocutaneous nerve transfer, and muscle transfers such as latissimus dorsi to biceps and Steindler’s flexorplasty. Shoulder arthrodesis was ultimately indicated for two primary reasons: in two patients, double-level lesions involving both the suprascapular and axillary nerves precluded shoulder stabilization, and in the remaining three patients, delayed presentation rendered further nerve reconstruction or transfer unfeasible. The follow-up duration ranged from 12 to 30 months (mean, 19.6 months), providing mid-term outcome data after fusion.
Patients (6–10) with pan-brachial plexus injuries underwent shoulder fusion primarily due to the limited reconstructive options available (Table 1). All were young males (age range, 27–36 years; mean, 30.8 years), with the right side affected in every case. The average time from injury to initial Surgery was 5.6 months (range, 2–7 months), while the mean interval between the first surgery and shoulder arthrodesis was 6.2 months (range, 4–8 months), reflecting a staged reconstruction approach. The primary interventions involved various combinations of nerve transfers, most commonly intercostal-to-musculocutaneous or intercostal-to-pectoral nerve transfers, and functioning free gracilis muscle transfers reinnervated by the spinal accessory nerve. One patient also underwent a contralateral C7 to lower trunk transfer. The principal indication for shoulder fusion in four of the five patients was the absence of viable donor nerves, making them unsuitable for further reconstructive procedures. The final follow-up period ranged from 14 to 72 months (mean, 38.8 months), allowing assessment of long-term functional outcomes.
All patients with upper brachial plexus injuries who underwent shoulder arthrodesis retained a reasonable degree of scapulothoracic motion with a mean abduction of 52°, protraction of 68°, and a mean retraction of 46° (Table 2). All patients demonstrated recovery of functional upper limb independence with the ability to perform brachiothoracic grasp and hand-to-mouth activities. The mean time to union following shoulder fusion was 7.4 months, while the longest time to union was 11 months (Fig. 2).
Table 2. The functional outcomes of patients with upper brachial plexus injuries in comparison to those with pan-brachial plexus palsy who underwent shoulder fusionParametersUpper brachial plexus palsyGlobal brachial plexus palsyIndependent t-testAbduction52° (45°–60°)44°(40°–45°)p < 0.0001Protraction68° (60°–80°)38° (30°–40°)p < 0.0001Retraction46° (45°–50°)41° (40°–45°)p = 0.0003Brachiothoracic graspYesYesHand to mouth/bellyYesYesVAS Score6.0 ± 5.516.0 ± 11.4− p = 0.04DASH Score24.4 ± 4.535.8 ± 5.3P = 0.02Time to union7.4 months (6–11 months)7.2 months (6–9 months)
Fig. 2. Patient with upper brachial plexus palsy showing A radiological outcome at 14 months demonstrating solid bony union and maintained alignment, and B functional outcome illustrating stable shoulder with satisfactory range of motion in the desired position
We observed that patients with pan-brachial plexus palsy who underwent shoulder arthrodesis were able to demonstrate brachiothoracic grasp and hand-to-mouth activities, in addition to attaining considerable scapulothoracic motion despite profound neurological involvement. The scapulothoracic motion was demonstrated in terms of 44° degrees of shoulder abduction, 38° degrees of protraction, and 41° degrees of retraction, which contributed significantly to compensatory movement following fusion. Notably, these values were comparable to those observed in patients with upper brachial plexus injuries, implying that even in cases of pan-plexus involvement, a functional range of motion can be achieved when the periscapular muscles remain viable or are successfully reinnervated. The time to bone union after arthrodesis ranged from 6 to 9 months, consistent with expected healing timelines for shoulder fusion. These outcomes demonstrate meaningful functional gains following shoulder arthrodesis, reinforcing its role as an effective salvage procedure for complex brachial plexus injuries (Fig. 1F).
Statistical analysis comparing patients with upper brachial plexus palsy and pan brachial plexus palsy revealed significant differences across all outcome variables. Patients in the upper group exhibited significantly better abduction (p < 0.0001), protraction (p = 0.0003), and retraction (p = 0.0003) movements compared to the pan group (independent t-test). The time to union was comparable between the two groups. The DASH (Disabilities of the Arm, Shoulder, and Hand) score was significantly better in patients with upper plexus palsy (mean 24.4 ± 4.5) compared to those with global palsy (mean 36.8 ± 5.3), p = 0.004. Pain levels (VAS) improved in both groups, with no significant difference, indicating arthrodesis provided consistent pain relief regardless of palsy type (Table 2).
Patients with preserved or reinnervated pectoralis major, trapezius, serratus anterior, and rhomboid muscles, demonstrating a minimum of grade 3 muscle power, showed improved functional outcomes, as evidenced by lower DASH scores and minimal pain levels. In contrast, those with absent muscle power, particularly of the serratus anterior and pectoralis major, as noticed in Table 3.
Table 3. Parascapular muscle involvement across patients, along with their DASH scores (functional impairment) and VAS scores (pain)PatientPectoralisTrapeziusSerratus anteriorRhomboidsDASH (100–0)VAS (0–100) Upper brachial plexus palsy 1NoYesYesYes2602YesYesYesYes2403YesYesYesYes31104YesYesYesYes20105YesYesYesYes2110 Global brachial plexus palsy 6YesYesYesYes3607YesYesNoYes33308YesYesNoNo46209NoYesNoNo312010NoYesNoYes3310
Discussion
The primary conclusion of this study is that favourable functional outcomes following shoulder arthrodesis in cases of post-traumatic brachial plexus injury are predominantly associated with particular preoperative factors rather than with the surgical technique adopted alone. In particular, the preservation or successful reinnervation of critical parascapular muscles and achieving an optimal fusion position were strongly associated with improved postoperative function. These parameters appear essential in facilitating effective scapulothoracic compensation following the loss of glenohumeral mobility.
A comparative analysis of upper and global plexus palsy revealed that patients with upper plexus injuries typically exhibited improved range of motion and higher functional scores, likely due to the relatively preserved scapulothoracic mechanics. Notably, patients with global palsy exhibited considerable functional improvements, particularly in brachiothoracic grasp, alongside scapular protraction and retraction (Fig. 3), when the essential stabilizing muscles, such as the serratus anterior and pectoralis major, demonstrated a minimum of grade three muscle strength.
Fig. 3. Patient with upper brachial plexus palsy showing A radiological outcome at 16 months demonstrating solid bony union and maintained alignment, and B functional outcome illustrating stable shoulder with satisfactory range of motion in the desired position
While the previous literature on shoulder arthrodesis has mainly concentrated on documenting postoperative function, limited studies have explored the factors that influence optimal outcomes. Garg et al. [14] and van der Lingen et al. [15] reported improved results in individuals with intact functionality of the spinal accessory nerve and scapulothoracic muscles, respectively. Nevertheless, these studies did not classify outcomes based on the pattern of plexus involvement with the exact extent of specificity as in the present series. Our findings suggest that classification based on neurological involvement provides enhanced prognostic insight in the context of arthrodesis.
The pectoralis major, trapezius, levator scapulae, serratus anterior, and rhomboids collaboratively facilitate scapulothoracic movement to compensate for diminished glenohumeral mobility. The trapezius and levator scapulae allowed arm elevation through scapular rotation, whereas the serratus anterior allowed forward reaching through protraction and upward rotation, despite the lack of deltoid function. The preservation or reinnervation of the pectoralis major was significantly associated with the recovery of brachiothoracic grip and forward reach, hence improving midline hand function. Patients with intact or reanimated parascapular musculature demonstrating a minimum of grade three muscle strength achieved better functional outcomes in our study, highlighting the need for comprehensive preoperative assessment and targeted nerve reconstruction (Table 3).
Functional results are also strongly influenced by fusion position. To enhance functional reach and minimize periscapular pain, Sousa et al. [16] recommended the fusion position of 35° of abduction, 30° of forward flexion, and less than 45° of internal rotation. Arthrodesis was performed in our series at approximately 30° of internal rotation, 30° of flexion, and 30° of abduction. This configuration has been associated with the most effective upper limb placement for everyday tasks while avoiding winging or severe scapular discomfort. Our findings are consistent with biomechanical evidence demonstrating balanced scapulothoracic loading. Furthermore, the simultaneous acromiohumeral and glenohumeral fusion was shown to boost fusion rates by Rehmann et al. [17], a concept that is integrated into our surgical technique.
A meta-analysis by Zhang et al. [18] comparing upper trapezius transfer and shoulder arthrodesis revealed similar outcomes for both treatments in terms of range of motion and complication rates. However, the analysis devoted little consideration to shoulder stability measures, brachiothoracic grasp, and scapular dynamics, all of which are crucial following arthrodesis.Our study aims to fill this gap by emphasizing the significance of scapular control and compensatory mechanisms, which have a direct impact on independence and long-term satisfaction beyond conventional outcome measures such as DASH or VAS scores.
Complications associated with shoulder arthrodesis include non-union, postoperative fracture, hardware irritation, and infection. Historically, non-union rates have reached as high as 20% [18], but improvements in fixation methods have significantly decreased this risk [17, 19]. In our series, the lack of significant complications can be attributed to stable fixation and optimal fusion positioning.
The study adhered to the STROBE guidelines [20] and aligns with the United Nations Sustainable Development Goals 3 and 4 [21]. However, the retrospective design and limited sample size restrict the generalizability of the findings, as well as other limitations. Given the retrospective design of the investigation, blinding was not practical. Objective measurement of parascapular muscle strength through electromyography or advanced imaging was not conducted; instead, assessments were based on clinical evaluation, which is subject to the examiner’s judgment and interpretation.. Further prospective investigations utilizing objective biomechanical assessment are recommended.
To conclude, shoulder arthrodesis continues to be a dependable salvage procedure for post-traumatic brachial plexus palsy when reconstructive options are limited. Favorable outcomes are closely associated with the preservation or reinnervation of essential parascapular muscles, notably the trapezius, serratus anterior, and pectoralis major, as well as correct fusion positioning. Even in cases of global plexus palsy, satisfactory functional recovery can be attained when scapulothoracic stability and compensatory movements are restored (Fig. 3).