Reverse Total Shoulder Arthroplasty for Failed Osteosynthesis in Proximal Humerus Fractures: Outcomes and Challenges
Luís B Pinto, João Alves, Eduardo Ferreira, Herculano Nascimento, António Miranda, Tiago P Torres

TL;DR
Reverse total shoulder arthroplasty (RTSA) is effective for treating failed surgeries in complex proximal humerus fractures, offering pain relief and improved function.
Contribution
This study provides evidence on the outcomes of RTSA as a salvage procedure for failed osteosynthesis in proximal humerus fractures.
Findings
RTSA improved Constant Scores from 35 preoperatively to 88 postoperatively.
Persistent pain and dysfunction were the main indications for RTSA after failed osteosynthesis.
Calcar comminution and poor bone quality were identified as risk factors for initial fixation failure.
Abstract
Background Proximal humerus fractures (PHF) are among the most common humeral fractures, particularly affecting elderly individuals, often following low-energy trauma. While conservative treatment is often preferred in geriatric patients, surgical management remains indicated for displaced fractures. Reverse total shoulder arthroplasty (RTSA) has increasingly been used as a primary treatment option for complex PHF, especially Neer three and four-part patterns. However, in the setting of failed osteosynthesis, there is a lack of evidence regarding the role and outcomes of RTSA. Methods A retrospective study of nine patients who underwent RTSA for failed osteosynthesis of PHF between 2018 and 2023 was conducted. Demographic and clinical data were collected from electronic medical records. The patients were clinically reassessed, and preoperative imaging was reviewed to identify failure…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
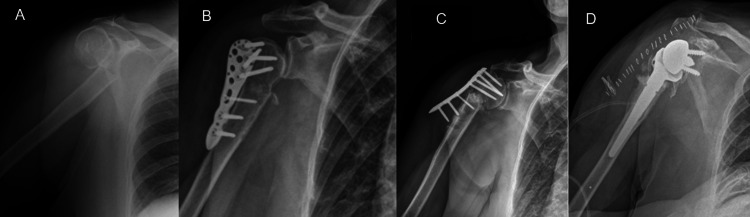 Figure 1
Figure 1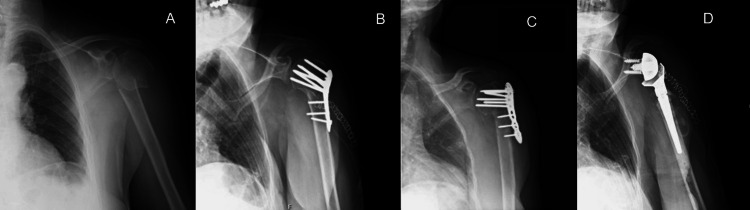 Figure 2
Figure 2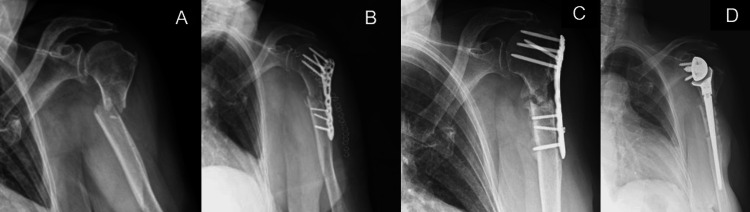 Figure 3
Figure 3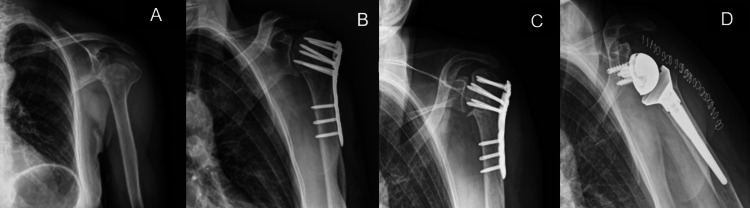 Figure 4
Figure 4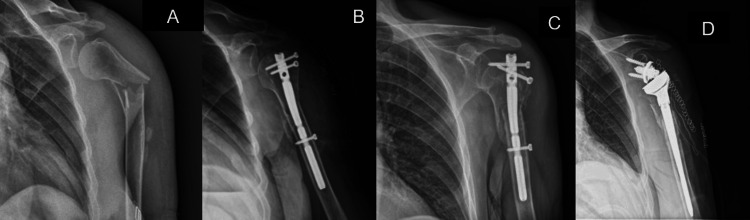 Figure 5
Figure 5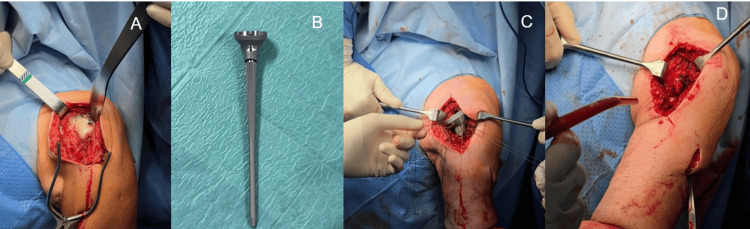 Figure 6
Figure 6 Figure 7
Figure 7| Total patients (n) | 9 |
| Male patients | 1 |
| Female patients | 8 |
| Mean age at RTSA (range in years) | 67 (54-75) |
| Left side | 3 |
| Right side | 6 |
| Mean follow-up (months) | 22 ± 4 |
| Case | Patient | Fracture (Neer classification) | Surgery |
| 1 | Female, 75y | 2-part | ORIF w/ plate and screws |
| 2 | Female, 73y | 2-part | ORIF w/ plate and screws |
| 3 | Female, 54y | 2-part | ORIF w/ plate and screws |
| 4 | Female, 70y | 2-part | CRIF w/ proximal humeral nail |
| 5 | Female, 68y | 2-part | ORIF w/ plate and screws |
| 6 | Female, 53y | 3-part | ORIF w/ plate and screws |
| 7 | Female, 70y | 2-part | ORIF w/ plate and screws |
| 8 | Male, 65y | 3-part | ORIF w/ plate and screws |
| 9 | Female, 71y | Proximal humeral metaphysis | CRIF w/ proximal humeral nail |
| Case | Patient | Fracture (Neer classification) | Cause of failure |
| 1 | Female, 75y | 2-part | Varus collapse |
| 2 | Female, 73y | 2-part | Non-union |
| 3 | Female, 54y | 2-part | Varus collapse |
| 4 | Female, 70y | 2-part | Nail pull-out |
| 5 | Female, 68y | 2-part | Varus collapse |
| 6 | Female, 53y | 3-part | Avascular necrosis |
| 7 | Female, 70y | 2-part | Varus collapse |
| 8 | Male, 65y | 3-part | Avascular necrosis |
| 9 | Female, 71y | Proximal humeral metaphysis | Nail pull-out |
| AROM | Mean value |
| Abduction | 80º |
| Forward elevation | 85º |
| External rotation | Nape |
| Internal rotation | Lateral buttock |
| Pain Visual Analog Scale [ | |
| Preoperative | 7 |
| Postoperative | 3 |
| Constant Score [ | |
| Preoperative | 65 |
| Postoperative | 88 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Shoulder and Clavicle Injuries · Elbow and Forearm Trauma Treatment
Introduction
Proximal humerus fractures (PHFs) are the most common fractures of the humerus. They account for 4% to 10% of all fractures and approximately half of all upper limb fractures. PHF occur more frequently in elderly women and are generally associated with low-energy trauma, making them the third most common osteoporotic fractures [1].
The management of these fractures in the geriatric population is predominantly conservative [2]. However, in younger patients and in cases of complex fracture patterns (e.g., Neer three- and four-part fractures [3]) with significant displacement, surgical treatment is indicated unless medical risk factors deem the patient unfit for surgery. Surgical options comprise open reduction and internal fixation (ORIF) or closed reduction and internal fixation (CRIF), as well as reverse total shoulder arthroplasty (RTSA) [1,4,5]. In recent years, RTSA has been increasingly used as the primary surgical treatment for PHFs in Neer three- and four-part fractures in active elderly patients, providing more predictable outcomes compared to osteosynthesis and hemiarthroplasty [6-8]. This trend is due to the complications often associated with ORIF or CRIF, such as screw cut-out, malunion of the tuberosities, glenoid erosion, and avascular necrosis of the humeral head [6-8].
There is still controversy regarding the minimum age for indicating primary RTSA in PHFs. However, in cases of osteosynthesis failure, the options typically include either revision surgery or conversion to RTSA [7-11]. Currently, there is a lack of robust scientific evidence regarding the role and outcomes of RTSA in the treatment of osteosynthesis failures and proximal humerus non-union [10,12-16].
The aim of this study is to describe nine cases of osteosynthesis failure and non-union after osteosynthesis in PHFs treated with RTSA. The authors sought to analyze the clinical and functional outcomes of RTSA following failed osteosynthesis, as well as the causes and potential risk factors for osteosynthesis failure as a secondary objective.
Materials and methods
This is a retrospective observational study, which included patients who underwent revision surgery with RTSA following the failure of proximal humerus osteosynthesis. The study was conducted at a single tertiary care institution. Cases treated between January 2018 and December 2023 with a minimum follow-up of 12 months were eligible for inclusion.
Failure of osteosynthesis was defined as the presence of complications such as non-union, fixation failure, screw cut-out, implant loosening or humeral head avascular necrosis, requiring revision surgery. A total of nine patients with failed proximal humerus osteosynthesis, who were subsequently treated with RTSA, were included.
Patients’ electronic medical records were retrospectively reviewed to collect demographic data, comorbidities, fracture characteristics, type of initial osteosynthesis, and causes for fixation failure. All patients were also clinically reassessed at the time of data collection to obtain updated clinical and functional outcomes.
The primary objective was to evaluate the clinical and functional outcomes of RTSA as a salvage procedure for proximal humerus osteosynthesis failure. A secondary objective was to identify potential risk factors associated with osteosynthesis failure. Clinical assessment included pain evaluation and shoulder function using standardized outcome measures with the Visual Analog Scale (VAS) and Constant-Murley score [17-19]. In all the procedures, the surgical approach, implant selection, and postoperative rehabilitation protocols were standardized according to the institutional practice.
According to the institutional policy, formal approval from an ethics committee was not required for retrospective observational studies based on anonymized clinical data. Therefore, ethics approval and informed consent were waived for this study.
Results
There was a predominance of female patients (n=8; 89%), with a mean age of 67 years at the time of RTSA (Table 1).
In six cases (67%), the initial fracture was classified as a Neer two-part fracture, five (83%) of which were treated with ORIF using plates and screws, and one case (17%) was treated with a proximal humeral nail (Stryker®, Michigan, USA). Two cases (22%) involved Neer three-part fractures, both treated with ORIF using plates and screws (Stryker®, Michigan, USA). The remaining case (11%) was a proximal humeral metaphyseal fracture treated with a proximal humeral nail (Table 2).
Causes of failure are summarized in Table 3.
In all cases, the indication for RTSA was persistent pain and significant shoulder dysfunction. Figures 1-5 provide a clinical and radiological description of some of the cases.
Case 1A) Two-part PHF B) ORIF with plate and screws C) Varus collapse with screw pull-out D) RTSAPHF: proximal humerus fracture; ORIF: open reduction and internal fixation; RTSA: reverse total shoulder arthroplasty
Case 3A) Two-part PHF B) ORIF with plate and screws C) Varus collapse with screw pull-out D) RTSAPHF: proximal humerus fracture; ORIF: open reduction and internal fixation; RTSA: reverse total shoulder arthroplasty
Case 2A) Two-part PHF B) ORIF with plate and screws C) At 9-month follow-up, Non-union D) RTSAPHF: proximal humerus fracture; ORIF: open reduction and internal fixation; RTSA: reverse total shoulder arthroplasty
Case 6A) Three-part PHF B) ORIF with plate and screws C) Avascular necrosis D) RTSAPHF: proximal humerus fracture; ORIF: open reduction and internal fixation; RTSA: reverse total shoulder arthroplasty
Case 9A) Proximal humeral metaphysis fracture B) CRIF with proximal humeral nail C) Proximal nail pull-out D) RTSACRIF: closed reduction and internal fixation; RTSA: reverse total shoulder arthroplasty
In all cases, a preoperative infection screening was performed through laboratory tests, and a preoperative CT scan was conducted for surgical planning. Additionally, four intraoperative samples were collected for cytobacteriological examination in all patients, with all results being negative for infection. The removal of osteosynthesis material was performed in the same surgical procedure as the RTSA, except for one case in which RTSA was carried out nine months after hardware removal.
The surgical technique used was the same for all patients, and all procedures were performed by experienced shoulder surgeons. Patients were positioned in a "beach chair" position under general anesthesia with an interscalene block. The surgical approach used was the deltopectoral approach, and a tenodesis of the long head of the biceps tendon was performed in cases where it was still present.
RTSA was performed using a LIMA® implant (LimaCorporate S.p.A., San Daniele del Friuli, Udine, Italy) in all patients. Whenever possible, tuberosity preservation and reattachment were attempted, provided that the bone stock was deemed satisfactory based on the surgeon’s assessment and following the technique described by Boileau et al. [20-24]. Reinsertion of the tuberosities was achieved in four patients (44%) (Figure 6).
Case 9A) Proximal humeral nail pull-out with rotator cuff lesion B) Long humeral stem (LIMA®) C) and D) Reinsertion of tuberosities with the technique describe by Boileau et al. [20].Implant details: LIMA® (LimaCorporate S.p.A., San Daniele del Friuli, Udine, Italy)
In two cases (22%), a cemented humeral stem was used, with one of them requiring a long stem. The decision to cement the humeral stem was made intraoperatively. The average length of hospital stay was three days, with all patients receiving perioperative antibiotic prophylaxis with cefazolin for 24 hours. Rehabilitation was initiated during hospitalization, with an average total rehabilitation period of one year and six months.
At the one-year follow-up, the mean active range of motion (AROM) was 90° of abduction, 110° of forward flexion, external rotation reaching the nape of the neck on average, and internal rotation reaching the lateral side of the buttock (Table 4 and Figure 7).
Case 9 Patient AROM six months after RTSA; AROM: active range of motion; RTSA: reverse total shoulder arthroplasty
Regarding complications after RTSA, only one case (11%) of traumatic dislocation was reported, which occurred three months postoperatively following a fall. The mean pre-RTSA VAS score was seven, decreasing to three after RTSA. The mean pre-RTSA Constant-Murley Score was 35, improving to 88 postoperatively, with the lowest post-RTSA Constant-Murley Score observed in the case of traumatic dislocation. The average time between the initial surgery and conversion to RTSA was 11.5 months, and the mean follow-up period after RTSA was 27 months.
Discussion
Performing RTSA after the failure of osteosynthesis in a PHF requires careful planning and execution by experienced shoulder surgeons. The presence of bone defects, poor residual bone stock quality, rotator cuff lesions and the condition of the surrounding soft tissues are key concerns in these cases [25-30]. Additionally, ruling out infection as a cause of osteosynthesis failure is mandatory [25,27-28].
RTSA is currently recognized in the literature as an excellent option as a revision procedure for cases of failed osteosynthesis in PHFs [28]. A recent study by Caldaria et al. demonstrated that RTSA, as a salvage procedure in such situations, provides satisfactory and durable outcomes compared to alternative therapeutic options, which have shown limited success [10,31,32].
In a study by Shannon et al., RTSA performed as a salvage procedure after unsuccessful PHF osteosynthesis exhibited a slightly higher complication rate compared to primary RTSA, but the revision and reoperation rate, as well as clinical outcomes and shoulder function, were comparable [33]. In another study, Sebastia-Forcada et al. compared the outcomes of primary RTSA versus secondary arthroplasty after failed proximal humeral locking plate fixation and demonstrated that patients who were revised to RTSA secondarily had slightly lower functional scores and higher complication rates compared with patients treated with primary RTSA but had significant functional improvement and pain relief compared with their preoperative status [16].
In our case series, RTSA resulted in significant improvements in both pain and mobility, with a mean post-RTSA Constant-Murley score of 88. Current literature reports high complication rates for RTSA following failed ORIF in PHF, highlighting dislocation as the most common complication [13]. We observed only one case (11%) of traumatic dislocation in our series, while less frequently, aseptic loosening, infection and periprosthetic fracture are also concerning complications. Boileau et al. suggested that proximal humeral bone loss could lead to an increased rate of aseptic loosening of the humeral component in RTSA [21-23,34]. Although no cases of aseptic loosening were recorded in our series, the follow-up period remained relatively short.
Lauren et al. reported a 20% reoperation rate in patients undergoing RTSA for proximal humerus non-union [13]. This high reoperation rate was not observed in our study, possibly due to the small sample size. Notably, in four out of the six cases (67%) of Neer two-part fractures treated with plates and screws (patients one, three, five and seven), osteosynthesis failure resulted from intraoperative malreduction, leading to varus collapse and screw pull-out, highlighting the importance of proper reduction during ORIF. Additionally, in all four of these cases, significant calcar comminution was present, which may have contributed to the osteosynthesis failure. Furthermore, in two cases (22%) (patients four and nine) of the proximal humeral nail pull-out, the authors retrospectively considered that, given the patients’ age (>70 years), they likely had poor, osteoporotic bone stock unsuitable for osteosynthesis and would have been better treated with primary RTSA. In the two cases (22%) with avascular necrosis (patients six and eight), both had preoperative Herthel Criteria (disrupted medial hinge as well as a displaced anatomical neck fracture, with >45º of angulation) with an increased risk of humeral head ischemia. It is also important to mention that the only case of non-union of our series (patient two) occurred in a female patient who was a smoker and had osteoporosis.
Our study has some limitations, including its retrospective nature, small sample size, absence of a comparison group (e.g., revision ORIF or primary RTSA), potential selection bias, heterogeneity in fracture patterns and failure mechanisms, which limits generalizability and precludes robust subgroup analysis and relatively short follow-up period.
Conclusions
Our case series adds to the growing body of evidence supporting RTSA as a complex but effective salvage surgical treatment for failed osteosynthesis of PHFs, achieving good clinical and functional outcomes. Nevertheless, the results are not always predictable, and the complication rate remains considerable. Additionally, observations from our retrospective case series suggest that certain characteristics of the initial fracture pattern, such as calcar comminution and poor bone quality, may be associated with an increased risk of osteosynthesis failure. Given the retrospective nature of our study as well as our small sample size, these findings should be interpreted in the context of the existing literature rather than as definitive risk factors. Nonetheless, they reinforce previously reported principles regarding the importance of meticulous surgical technique, including anatomical restoration of the calcar and adequate metaphyseal support, to reduce the risk of varus collapse in surgical neck fractures treated with locking plates.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiology of proximal humeral fractures: a detailed survey of 711 patients in a metropolitan area J Shoulder Elbow Surg Passaretti D Candela V Sessa P Gumina S 211721242620172873583910.1016/j.jse.2017.05.029 · doi ↗ · pubmed ↗
- 2Prediction of nonunion after nonoperative treatment of a proximal humeral fracture J Bone Joint Surg Am Goudie EB Robinson CM 66868010320213384904910.2106/JBJS.20.01139 · doi ↗ · pubmed ↗
- 3Displaced proximal humeral fractures. I. Classification and evaluation J Bone Joint Surg Am Neer CS 2nd 10771089521970 https://pubmed.ncbi.nlm.nih.gov/5455339/5455339 · pubmed ↗
- 4The translated proximal humerus fracture: a comparison of operative and nonoperative management J Orthop Trauma Cosic F Kirzner N Edwards E Page R Kimmel L Gabbe B 0837202310.1097/BOT.000000000000261237053113 · doi ↗ · pubmed ↗
- 5Primary versus salvage reverse total shoulder arthroplasty for displaced proximal humerus fractures in the elderly: a systematic review and meta-analysis J Shoulder Elb Arthroplast Nelson PA Kwan CC Tjong VK Terry MA Sheth U 194202010.1177/2471549220949731 PMC 828217134497963 · doi ↗ · pubmed ↗
- 6Reverse shoulder arthroplasty for recent proximal humerus fractures: outcomes in 422 cases Orthop Traumatol Surg Res Gallinet D Cazeneuve JF Boyer E 80581110520193127976910.1016/j.otsr.2019.03.019 · doi ↗ · pubmed ↗
- 7Reverse shoulder arthroplasty for acute proximal humeral fractures: postoperative complications at 7 days, 90 days and 1 year Injury Noguera L Trigo L Melero V Santana F Torrens C 3713755020193064262310.1016/j.injury.2019.01.002 · doi ↗ · pubmed ↗
- 8Reverse shoulder arthroplasty for the treatment of three-part and four-part proximal humeral fractures in the elderly J Shoulder Elbow Surg Ross M Hope B Stokes A Peters SE Mc Leod I Duke PF 2152222420152516834710.1016/j.jse.2014.05.022 · doi ↗ · pubmed ↗