Unusual endoscopic remission in an anti‐tumor necrosis factor refractory case of severe ulcerative colitis during upadacitinib therapy
Carine A. Halaby, Charlotte F. Kim, Richard Kellermayer

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
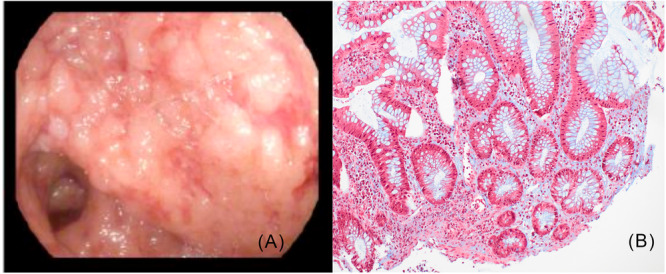 Figure 1
Figure 1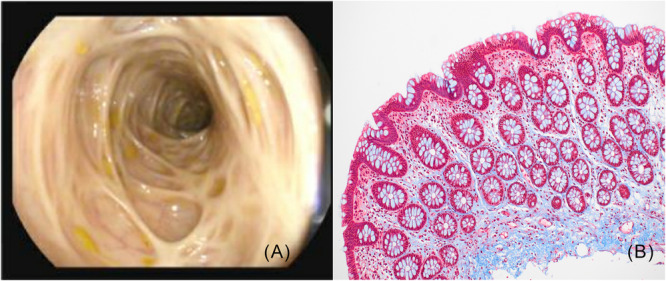 Figure 2
Figure 2- —Gutsy Kids Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory Bowel Disease · Microscopic Colitis · Rheumatoid Arthritis Research and Therapies
A 14‐year‐old female with ulcerative pancolitis (UC pancolitis), diagnosed by endoscopy at an outside hospital, was started on infliximab (IFX) 300 mg (5 mg/kg). After initial improvement, she relapsed severely (Pediatric Ulcerative Colitis Activity Index [PUCAI]1 = 70) 1 week postfirst dose. She was admitted for accelerated IFX (5 mg/kg at 1 week, then 10 mg/kg at 4 weeks) plus IV steroids but remained moderately to severely active after the third IFX (level 9.5 µg/mL; no antibodies). Colonoscopy 8 days after the third IFX (5 weeks from initiation), while on steroids, showed severe pancolitis (Mayo2 2–3) with extensive pseudopolyposis (Figure 1A); magnetic resonance (MR) enterography confirmed diffuse pancolitis. Upadacitinib (UPA 30 mg daily) was started as third‐line therapy,3 yielding rapid improvement. Vedolizumab (VEDO 300 mg every 8 weeks) was added 1 week later as a bridge target, with UPA continued. Steroids were tapered from 40 mg over 25 days from UPA initiation. After 2.5 months of dual therapy, reducing UPA to 15 mg caused relapse; 30 mg daily was resumed. She has since maintained >2 years of remission on dual (UPA/VEDO) therapy (patient preference), with normalized fecal calprotectin (43 µg/g). Surveillance colonoscopy at 1.5 years postdiagnosis (1 year in remission) showed fibrotic ridges, normal mucosa, and no active inflammation (Figure 2A); histology showed subepithelial collagen deposition (Figure 2B).
UPA is an emerging off‐label option for acute severe, anti‐tumor necrosis factor (TNF)‐refractory pediatric UC, with growing evidence of efficacy.4 Historically, such cases commonly progressed to colectomy.5 We propose that fulminant, treatment‐ refractory UC may represent a distinct inflammatory bowel disease (IBD) subtype,6 presenting clinically as UC pancolitis but exhibiting more extensive transmural involvement and submucosal fibrotic characteristics, as observed by Gordon et al.7 Notably, the presence of fibrosis and transmural changes‐ features classically associated with Crohn's disease (CD)‐raises a diagnostic dilemma. However, recent studies8 show that these features can occur in UC, especially in pediatric and long‐standing cases, and do not necessarily justify reclassification as CD in the absence of other distinguishing features such as granulomas, skip lesions, or small bowel involvement. This highlights potential limitations of current IBD classification and possible need for further refinement. Our case supports this predicament and underscores the importance of closely monitoring patients with severe, anti‐TNF refractory UC who respond to UPA “rescue” or “third‐line” therapy.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
ETHICS STATEMENT
An informed verbal consent was obtained from patient and parent before submission of the deidentified image case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Turner D , Hyams J , Markowitz J , et al. Appraisal of the pediatric ulcerative colitis activity index (PUCAI). Inflamm Bowel Dis. 2009;15(8):1218‐1223. 10.1002/ibd.20867 19161178 · doi ↗ · pubmed ↗
- 2Kerur B , Litman HJ , Stern JB , et al. Correlation of endoscopic disease severity with pediatric ulcerative colitis activity index score in children and young adults with ulcerative colitis. World J Gastroenterol. 2017;23(18):3322‐3329. 10.3748/wjg.v 23.i 18.3322 28566893 PMC 5434439 · doi ↗ · pubmed ↗
- 3Assa A , Aloi M , Van Biervliet S , et al. Management of paediatric ulcerative colitis, part 2: acute severe colitis‐An updated evidence‐based consensus guideline from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition and the European Crohn's and Colitis Organization. J Pediatr Gastroenterol Nutr. 2025;81(3):816‐851. 10.1002/jpn 3.70096 40528309 · doi ↗ · pubmed ↗
- 4Panés J , Dubinsky MC , Ishiguro Y , et al. Achievement of long‐term treatment goals in upadacitinib‐treated patients with moderately to severely active ulcerative colitis: a post hoc analysis of phase 3 trial data. J Crohns Colitis. 2025;19(7):jjaf 095. 10.1093/ecco-jcc/jjaf 095 40488552 PMC 12260494 · doi ↗ · pubmed ↗
- 5Ihekweazu FD , Fofanova T , Palacios R , et al. Progression to colectomy in the era of biologics: a single center experience with pediatric ulcerative colitis. J Pediatr Surg. 2020;55(9):1815‐1823. 10.1016/j.jpedsurg.2020.01.054 32087936 PMC 7396289 · doi ↗ · pubmed ↗
- 6Szigeti R , Krishna M , Kellermayer R . Letter: fulminant‐onset complicated inflammatory bowel disease (IBD)‐a unique subtype? Aliment Pharmacol Ther. 2023;57(10):1192‐1193. 10.1111/apt.17418 37094325 · doi ↗ · pubmed ↗
- 7Gordon IO , Abushamma S , Kurowski JA , et al. Paediatric ulcerative colitis is a fibrotic disease and is linked with chronicity of inflammation. J Crohn's Colitis. 2022;16(5):804‐821. 10.1093/ecco-jcc/jjab 216 34849664 PMC 9228908 · doi ↗ · pubmed ↗
- 8Ni P , Harpaz N , Altahrawi A , Liu Q . Diagnostic and prognostic significance of Crohn's disease‐like pathology in surgically diverted recta of patients with ulcerative colitis. Histopathology. 2025;7(1):81‐89. 10.1111/his.15429 39961608 · doi ↗ · pubmed ↗