Youngest known case of a pancreatic perivascular epithelioid cell tumor
Laura Gilligan, Wesley C. Judy, Bryan Clary, Timothy Fairbanks, Denise Malicki, Tom K. Lin

TL;DR
This paper reports the youngest known case of a rare pancreatic tumor called PEComa in an 8-year-old girl.
Contribution
The novelty is the identification of the youngest reported case of a pancreatic PEComa.
Findings
The tumor was diagnosed using imaging and tissue sampling techniques.
The tumor was benign and successfully removed with no recurrence observed.
The case expands the known age range for pancreatic PEComa diagnosis.
Abstract
Perivascular epithelioid cell tumors (PEComas) are a rare type of mesenchymal tumor that can arise in any part of the body. As of 2024, 37 cases of pancreatic PEComas had been reported in the literature with patients ranging in age from 17 to 74 years old. This is the youngest reported case of a pancreatic PEComa in an 8‐year‐old female presenting with abdominal pain and test findings of biliary obstruction. Magnetic resonance cholangiopancreatography identified the location, size, and obstructive effects of the mass. These findings prompted the performance of an endoscopic retrograde cholangiopancreatography and endoscopic ultrasound with fine‐needle aspiration to obtain a tissue sample that revealed the diagnosis of PEComa based on the morphological features and immunohistochemistry. Our patient's tumor was benign, successfully resected, and to date, the child has not had tumor…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
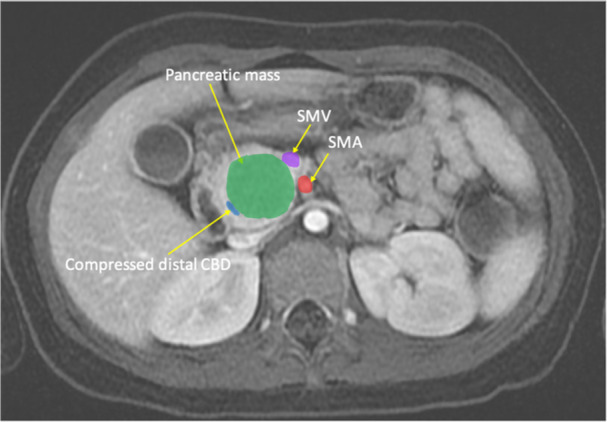 Figure 1
Figure 1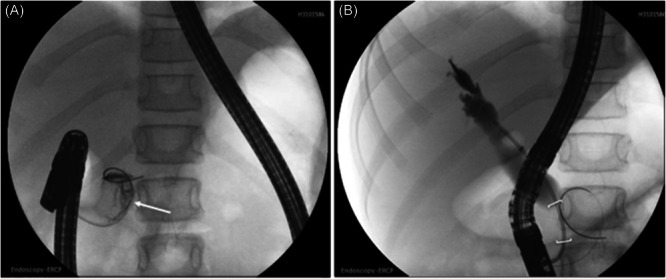 Figure 2
Figure 2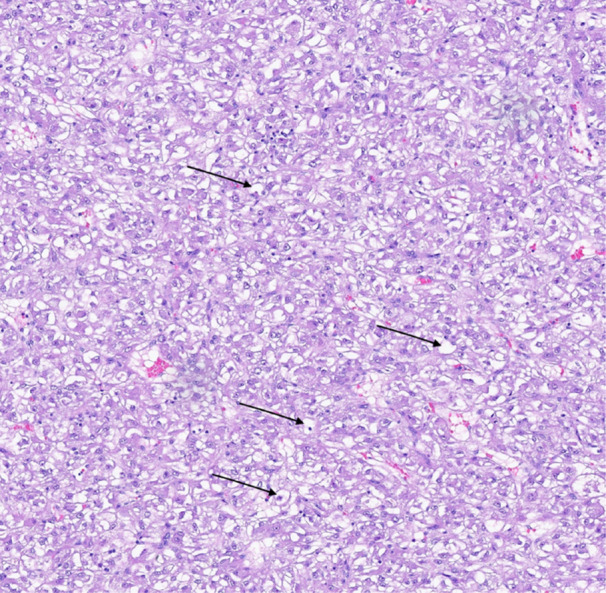 Figure 3
Figure 3| Year | Author | Age | Sex | Location of mass in pancreas | Surgical procedure | Outcome |
|---|---|---|---|---|---|---|
| 1996 | Zamboni | 60 | Female | Body | DP | NED |
| 2004 | Heywood | 74 | Female | Head | PPPD | NED |
| 2005 | Ramuz | 31 | Female | Body | SPDP | NED |
| 2008 | Perigny | 46 | Female | Body | Enucleation | NED |
| 2009 | Hirabayashi | 47 | Female | Head | PPPD | NED |
| 2009 | Baez | 60 | Female | Body | DP | NED |
| 2011 | Zemet | 49 | Male | Head | PPPD | NED |
| 2011 | Nagata | 52 | Male | Head | PD | AWD |
| 2011 | Xie | 58 | Female | Head | PD | NED |
| 2012 | Finzi | 62 | Female | Head | Total excision | NED |
| 2012 | Singh | 38 | Female | Tail | Total excision | NED |
| 2013 | Al‐Haddad | 38 | Female | Uncinate process | PD | n/a |
| 2013 | Okuwaki | 43 | Female | Body/tail | DP | NED |
| 2013 | Moura | 51 | Female | Head | PD | AWD |
| 2013 | Tummala | n/a | n/a | Head | n/a | n/a |
| 2014 | Kim | 31 | Female | Tail | DP | NED |
| 2015 | Petrides | 17 | Female | Head | PPPD | NED |
| 2016 | Wei | 58 | Female | Body | MP | NED |
| 2016 | Mizuuchi | 61 | Female | Head/body | PD | NED |
| 2016 | Collins | 54 | Female | Head/body | MP | NED |
| 2016 | Hartley | 31 | Female | Tail | DP | n/a |
| 2016 | Jiang | 50 | Female | Head | PD | NED |
| 2017 | Zhang | 43 | Female | Head | PD | NED |
| 2017 | Zizzo | 68 | Male | Head | None | AWD |
| 2018 | Sangiorgio | 47 | Female | Body | n/a | n/a |
| 2018 | Sangiorgio | 70 | Female | Body | n/a | n/a |
| 2018 | Hong | 35 | Female | Head | PD | n/a |
| 2019 | Uno | 49 | Female | Tail | DP | NED |
| 2019 | Gondran | 17 | Male | Head | None (Sirolimus) | AWD |
| 2020 | Ulrich | 49 | Female | Body | DP | n/a |
| 2020 | Sinha | 59 | Female | Tail | DP | n/a |
| 2020 | Colon | 50 | Female | Body | DP | NED |
| 2021 | Geng | 40 | Female | Body | PPPD | NED |
| 2022 | Harrison | 39 | Male | Tail | DP | NED |
| 2022 | Sixto | 68 | Male | Head | PPPD | NED |
| 2024 | Tsukita | 74 | Male | Tail | DP | NED |
| 2024 | Yuza | 23 | Female | Head | PD | NED |
| 2024 (Our case) | Gilligan | 8 | Female | Head | PD | NED |
- —None
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberous Sclerosis Complex Research · Renal cell carcinoma treatment · Histiocytic Disorders and Treatments
INTRODUCTION
1
The family of perivascular epithelioid cell tumors (PEComas) includes angiomyolipomas, clear cell “sugar” tumors, and PEComas‐not otherwise specified (PEComa‐NOS). These rare mesenchymal tumors can arise in any part of the body. They are composed of epithelioid cells with clear to eosinophilic granular cytoplasm and most commonly stain positive for melanocytic and myogenic markers. While most PEComas are benign, malignant potential exists. As of 2024, 37 cases of pancreatic PEComa had been reported in the literature with patients ranging in age from 17 to 74 years old1, 2, 3 (Table 1).
We present the youngest known case of pancreatic PEComa in an 8‐year‐old female with obstructive jaundice secondary to a solid pancreatic head mass.
CASE REPORT
2
An 8‐year‐old female from Guam presented with 6 months of progressively worsening abdominal pain, jaundice, weight loss, and acholic stools. Laboratory studies found a total and direct hyperbilirubinemia of 13 and 10 mg/dL, respectively, alanine aminotransferase (ALT) 421 U/L, and aspartate aminotransferase (AST) 228 U/L. An ultrasound was reportedly completed, though results from Guam were not available. Computed tomography (CT), followed by magnetic resonance cholangiopancreatography showed a noninvasive pancreatic head mass, prompting transfer to the United States.
Repeat cross‐sectional imaging (Figure 1) showed a 3 cm solid mass of the pancreatic head partially compressing the distal common bile duct (CBD) and mildly displacing the inferior vena cava, portal vein, duodenum, and distal stomach. There was no evidence of metastasis, nor of abnormal pancreatic duct anatomy such as pancreatic divisum. Partial oncologic workup was pursued and notable for a normal lactate dehydrogenase (187 U/L), normal alpha‐fetoprotein (<2.0 ng/mL), and normal carcinoembryonic antigen (<2.0 ng/mL).
The magnetic resonance cholangiopancreatography image shows a 2.7 × 2.6 × 3.2 cm noninvasive pancreatic head mass compressing the distal common bile duct, mildly displacing the duodenum, abutting the superior mesenteric vein and adjacent to the superior mesenteric artery.
An endoscopic retrograde cholangiopancreatography (ERCP) was performed: pancreatogram of the main pancreatic duct with findings of a large amorphous tissue mass within the head of the pancreas; cholangiogram was notable for a distal CBD narrowing with upstream ductal dilatation extending into the central intrahepatic ducts (Figure 2). A biliary sphincterotomy was performed followed by balloon extraction of a moderate amount of sludge material from the main bile duct. The distal CBD narrowing was brushed and duodenal fluid from the biliary tree and pancreatic duct were aspirated for cytology and tissue pathology. A plastic biliary stent was placed into the CBD. The ventral pancreatic duct showed abnormal filling and did not clearly connect to the main pancreatic duct. Therefore, a pancreatic duct stent was not placed, but a short pancreatic sphincterotomy was performed. The following day, endoscopic ultrasound with fine‐needle aspiration (EUS‐FNA) was performed. Following the procedures, the patient developed epigastric abdominal pain with a lipase of 898 U/L, increased from a lipase of 61 U/L at presentation, consistent with post‐procedural pancreatitis. It was not possible to differentiate a post‐ERCP versus post‐FNA pancreatitis since there was no lipase level between the two procedures.
(A) Endoscopic retrograde cholangiopancreatography pancreatogram with contrast opacification of an amorphous intraductal mass (arrow). (B) Cholangiogram with findings of common bile duct stricture (brackets) with upstream main bile duct dilation.
The cytology brushing of the biliary narrowing and the duodenal aspirates were non‐diagnostic. The FNA specimen revealed loose clusters of large epithelioid cells with vacuolated, eosinophilic cytoplasm (Figure 3) in the background of normal pancreatic acini and ducts. The tumor cells stained positive for HMB45, smooth muscle actin (SMA), inhibin, GATA3, MART1, and TFE3, and negative for CK7, CK20, S100, desmin, and synaptophysin. Collective findings were consistent with the diagnosis of pancreatic PEComa.
Hematoxylin and Eosin, x20 original objective. Moderately dense proliferation of large epithelioid cells with vacuolated/clear cytoplasm and variably sized nuclei, indicated with arrows.
The patient underwent pancreaticoduodenectomy with pancreaticojejunostomy, gastrojejunostomy, choledochojejunostomy, and cholecystectomy. The surgical margins were negative and histologically, the tumor was consistent with the FNA specimen, confirmed by immunohistochemistry. There was no evidence of malignant features nor metastases. The patient had an uncomplicated postsurgical course and was discharged on postoperative Day 12. At the 12‐month follow‐up, she was doing well and without evidence of recurrence.
DISCUSSION
3
The term “PEComa” was coined by Bonetti et al. in 1992 to describe lesions with epithelioid‐like cells in a perivascular distribution with co‐expression of melanocytic and myogenic markers.4 PEComas include angiomyolipomas, lymphangioleiomyomas, clear cell “sugar” tumors, and PEComas‐not otherwise specified. The tumors are characterized by mTOR pathway activating mutations including TSC1 or TSC2 bi‐allelic inactivation, TFE3 gene fusion and FLCN truncating mutations.5 PEComas can arise in almost any organ, including the stomach, intestines, liver, pancreas, lung, kidney, and genitourinary organs. Pancreatic PEComas are quite rare with only 37 previously reported cases in the literature.1, 2, 3 Until this case, the youngest reported PEComa patients were 17‐year‐old adolescents6, 7 (Table 1).
The symptoms of pancreatic PEComas can be vague or absent. Some patients have reported melena,6 low‐back pain, or diarrhea.1 However, abdominal pain is the most common complaint, present in over half of reported patients.1 Our patient had abdominal pain for about 5 months before the appearance of more insidious symptoms. These progressive symptoms prompted further evaluation leading to transfer to the United States for more comprehensive medical care. Aside from PEComa, the differential for a pre‐teen patient with a solid pancreatic head mass includes autoimmune pancreatitis, solid pseudopapillary neoplasm, pancreatoblastoma, insulinoma, adenocarcinoma, lymphoma, and other non‐epithelial tumors.8 Given the location of the lesion, it was amenable for EUS‐FNA to obtain the diagnostic specimen for histologic and immunohistochemical evaluation.
Histologically, PEComas arrange as sheets of epithelioid cells with clear to eosinophilic cytoplasm. Distinctive perivascular epithelioid cells are present with the expression of markers for both melanocytes and smooth muscle. Primary tumor features associated with malignant behavior (metastases, local invasion) include size >5 cm, high grade atypia, mitoses >1/50 high power fields, presence of necrosis, and lymphovascular invasion.9 Our patient's tumor was 3 cm and met no other criteria, which favored being a benign mass with low likelihood of metastasis. Immunohistochemically, PEComas stain positive for melanocytic (HMB‐45, MiTF, MelanA, and MART1) and myogenic (SMA, desmin) markers. HMB‐45 has been positive in all but one case.1, 2, 3
The optimal treatment of primary pancreatic PEComas involves resection of the mass with negative margins when feasible. Of the 35 cases, including our own, in the existing literature with data on treatment (three cases lack information on treatment), 94 percent underwent surgical resection1, 2, 3 (Table 1). PEComas can reach significant size, yet given the lack of local invasion associated with most primary tumors, resection can still be feasible. This is particularly relevant to PEComas involving the head and uncinate of the pancreas where adjacent visceral vasculature may be displaced but are uncommonly invaded. Systemic medical treatment regimens with modest activity exist including traditional sarcoma agents (anthracycline, gemcitabine) as well as mTOR inhibitors.7 Recurrence following resection of pancreatic PEComa in patients without metastases at presentation appears to be quite infrequent, even for those with adverse features.10
CONCLUSION
4
In summary, pancreatic PEComas are a rare type of mesenchymal tumor. Though typically benign, malignant potential exists and treatment involves resection of the mass. In this report, we describe the presentation, evaluation, and treatment of a pancreatic PEComa in an 8‐year‐old female, the youngest reported patient to be diagnosed with this type of tumor.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest.
ETHICS STATEMENT
We wish to thank the patient and her parents, who provided consent for this case report to be written and discussed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nogueira Sixto M , Carracedo Iglesias R , Estévez Fernández S , Rodríguez Pereira C , Sánchez Santos R . Pancreatic PE Coma, a not so uncommon neoplasm? systematic review and therapeutic update. Gastroenterol Hepatol. 2024;47(1):93‐100. 10.1016/j.gastrohep.2023.05.009 37230381 · doi ↗ · pubmed ↗
- 2Tsukita H , Koyama K , Ishinari T , et al. A case of pancreatic PE Coma with prominent inflammatory cell infiltration: the inflammatory subtype is a distinct histologic group of PE Coma. Diagn Pathol. 2024;19(1):59. 10.1186/s 13000-024-01485-2 38622713 PMC 11017648 · doi ↗ · pubmed ↗
- 3Yuza K , Takenouchi A , Kobayashi K , et al. Pancreatic PE Coma with preoperative tumor fluctuations: a diagnostic challenge in a rare case report. HPB. 2024;26:S 315‐S 316.
- 4Bonetti F , Pea M , Martignoni G , Zamboni G . PEC and sugar. Am J Surg Pathol. 1992;16(3):307‐308. 10.1097/00000478-199203000-00013 1599021 · doi ↗ · pubmed ↗
- 5Agaram NP , Sung YS , Zhang L , et al. Dichotomy of genetic abnormalities in PE Comas with therapeutic implications. Am J Surg Pathol. 2015;39(6):813‐825. 10.1097/PAS.0000000000000389 25651471 PMC 4431898 · doi ↗ · pubmed ↗
- 6Petrides C , Neofytou K , Khan AZ . Pancreatic perivascular epithelioid cell tumour presenting with upper gastrointestinal bleeding. Case Rep Oncol Med. 2015;2015:431215. 10.1155/2015/431215 25632358 PMC 4302363 · doi ↗ · pubmed ↗
- 7Gondran H , Thebaud E , Moreau A , et al. First pancreatic perivascular epithelioid cell tumor (PE Coma) treated by m TOR inhibitor. Pancreatology. 2019;19(4):566‐568.31130397 10.1016/j.pan.2019.05.459 · doi ↗ · pubmed ↗
- 8Patterson KN , Trout AT , Shenoy A , Abu‐El‐Haija M , Nathan JD . Solid pancreatic masses in children: a review of current evidence and clinical challenges. Front Pediatr. 2022;10:966943. 10.3389/fped.2022.966943 36507125 PMC 9732489 · doi ↗ · pubmed ↗