Over‐the‐wire insertion of a naso‐duodenal feeding tube in a critically ill infant
Hashim Abdul‐Khaliq, Jochen Pfeifer

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
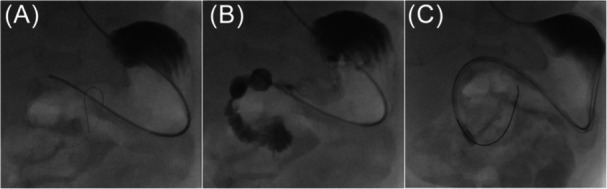 Figure 1
Figure 1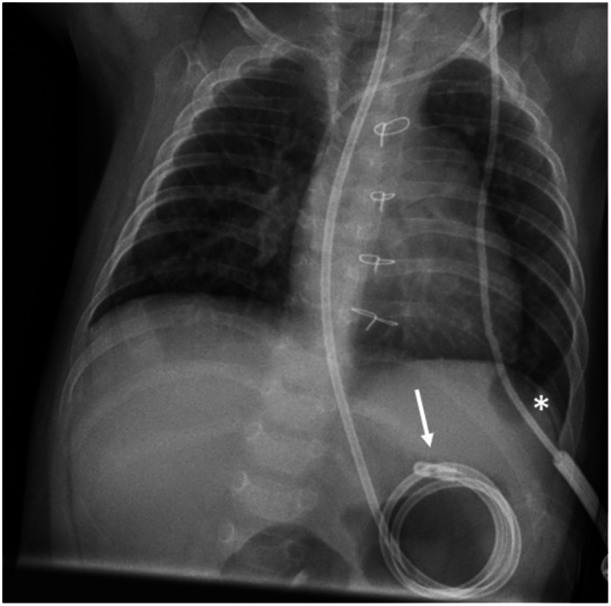 Figure 2
Figure 2- —None
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClinical Nutrition and Gastroenterology · Esophageal and GI Pathology · Intestinal Malrotation and Obstruction Disorders
In a 7‐month‐old boy (body weight 7 kg) with congenital heart disease, short bowel syndrome, and gastric motility disorder, conventional insertion of a duodenal feeding tube was unsuccessful (Figure 1). Alternatively, a catheter‐based method under fluoroscopy was performed. An angiography catheter (4F multipurpose special; Cordis Corp., Miami Lakes, FL, USA) was inserted nasogastrically into the stomach, then a guide wire (0.014'' Whisper™ ES; Abbott Medical, Santa Clara, CA, USA) was advanced into the duodenum over which the catheter could be pushed (Figure 2A). The course of the duodenum then was visualized by manual contrast injection (Figure 2B). Next, a more stable guide wire (0.018'' Nitrex™; ev3 Inc., Plymouth, MN, USA) was carefully inserted into the distal duodenum. To enable an insertion over‐the‐wire, the closed tip of an enteral feeding tube (8 F Freka™ Tube; Fresenius Kabi AG, Bad Homburg, Germany) was cut off. To deburr it, the tip was ground down and washed. Using ultrasound gel to improve gliding ability, the tube could be easily advanced into the duodenum via the wire without any complications (Figure 2C).
Neonates and infants with severe diseases often experience nutrition difficulties. The use of naso‐gastric or, in case of gastric emptying disorders, post‐pyloric tubes may be necessary.1 Blind bedside placement of duodenal tubes can be challenging.2 Endoscopic or percutaneous approaches are alternative, but invasive techniques. Derived from conventional cardiovascular catheterization using angiography catheters under brief fluoroscopy, the over‐the‐wire technique is a simple method for the safe and correct placement of duodenal tubes.3, 4
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
ETHICS STATEMENT
Written informed consent was obtained from the patient's father for publication of the images, and any potentially identifying information has been removed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kuwata S , Iwamoto Y , Ishido H , Taketadu M , Tamura M , Senzaki H . Duodenal tube feeding: an alternative approach for effectively promoting weight gain in children with gastroesophageal reflux and congenital heart disease. Gastroenterol Res Pract. 2013;2013:181604. 10.1155/2013/181604 23653635 PMC 3638695 · doi ↗ · pubmed ↗
- 2Taylor SJ , Sayer K , White P . Nasointestinal tube placement: techniques that increase success. J Intensive Care Soc. 2023;24(1):62‐70. 10.1177/17511437221095336 PMC 997580436874290 · doi ↗ · pubmed ↗
- 3Hwang JY , Shin JH , Lee YJ , et al. Fluoroscopically guided nasojejunal enteral tube placement in infants and young children. AJR Am J Roentgenol. 2009;193(2):545‐548. 10.2214/AJR.08.1341 19620455 · doi ↗ · pubmed ↗
- 4Fang JC , Hilden K , Holubkov R , Di Sario JA . Transnasal endoscopy vs. fluoroscopy for the placement of nasoenteric feeding tubes in critically ill patients. Gastrointest Endosc. 2005;62(5):661‐666. 10.1016/j.gie.2005.04.027 16246675 · doi ↗ · pubmed ↗