Long-term health effects of COVID-19 among patients in Croatian primary care settings
Branislava Popović, Ana Lesac Brizić, Aleksandar Ljubotina, Tina Zavidić, Vedrana Tudor Špalj, Roberta Marković Štimac, Martina Fišić Jurković, Nina Bašić Marković, Ines Diminić Lisica, Jasna Vučak, Nives Radošević Quadranti

TL;DR
This study examines long-term health effects of COVID-19 in Croatia, finding that severe infection and certain pre-existing conditions increase the risk of post-COVID symptoms.
Contribution
The study identifies risk factors and health outcomes associated with post-COVID conditions in primary care settings.
Findings
Severe COVID-19 and older age are strongly associated with long-term pulmonary and neurological effects.
Vaccination is linked to milder disease and lower risk of post-COVID conditions.
Pre-existing conditions like diabetes and obesity predict brain fog and mental health disorders after infection.
Abstract
The COVID-19 pandemic has left lasting effects that extend beyond the acute phase of infection, with increasing evidence of long-term health consequences. This study aimed to assess the prevalence of post-COVID symptoms and conditions and to identify associated risk factors, including pre-existing chronic diseases, COVID-19 vaccination status, and severity of acute infection. This retrospective cross-sectional study was conducted in 10 family medicine practices in Croatia. The data collected from medical records included demographics, COVID-19 vaccination status, SARS-CoV-2 infection history and severity, and documented health conditions before and after infection. Descriptive statistics were used to summarize the data. Group differences were analyzed using the independent samples t-test or χ2 test. Variables significant in univariate analyses (p < 0.05) were included into multivariate…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
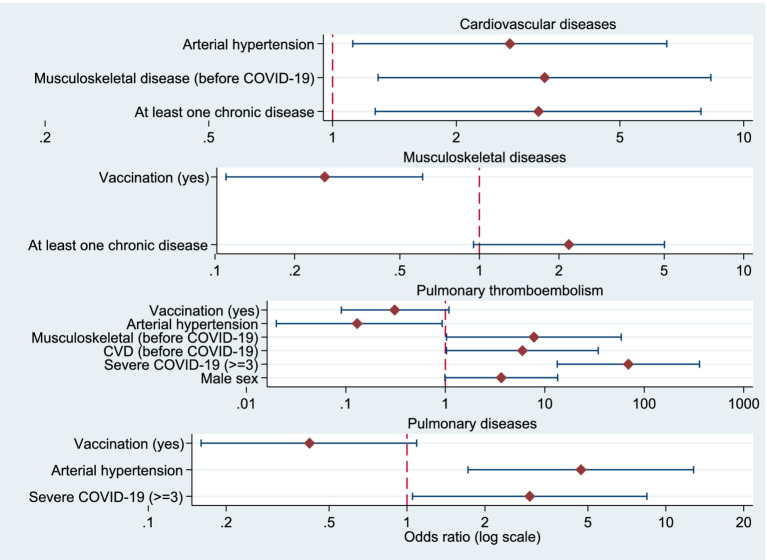 Figure 1
Figure 1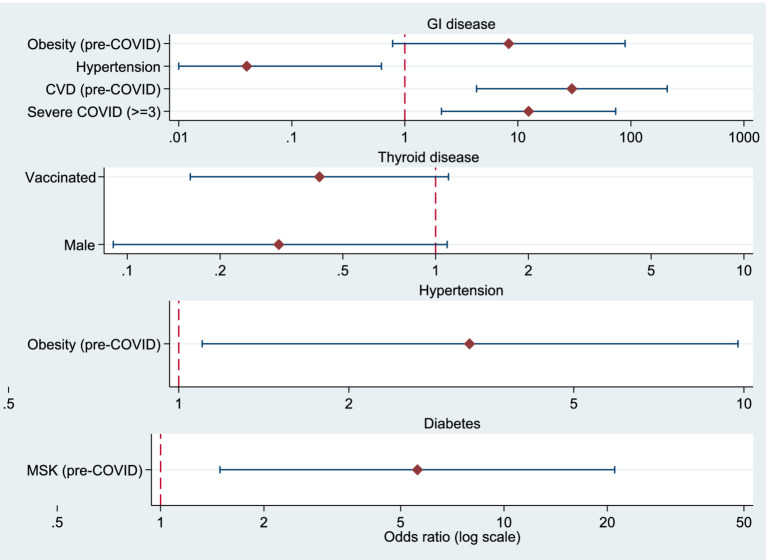 Figure 2
Figure 2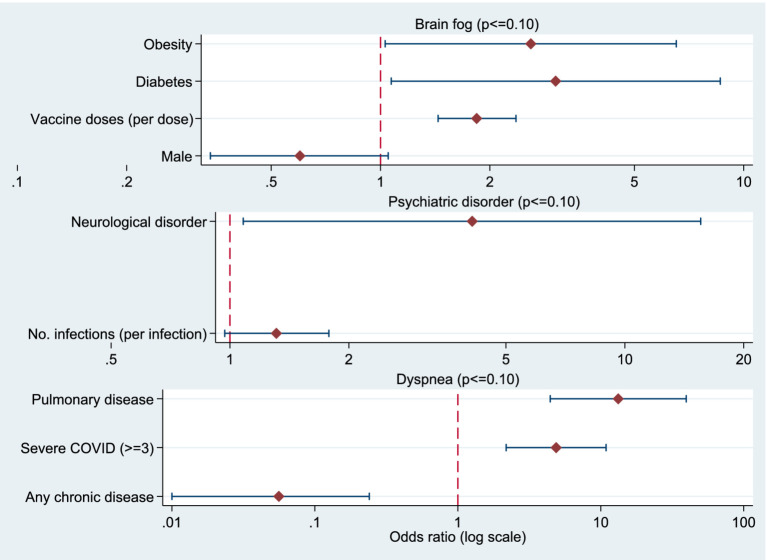 Figure 3
Figure 3| Urban/rural setting | Number of patients | Average patients’ age | GP sex | GP years of age | GP years of experience |
|---|---|---|---|---|---|
| Rural | 2,197 | 45.3 | Female | 39 | 15 |
| Rural | 2,010 | 49.7 | Female | 52 | 23 |
| Rural | 1,354 | 55.1 | Female | 44 | 18 |
| Rural | 1,728 | 62.2 | Female | 65 | 41 |
| Rural | 2,120 | 50 | Female | 57 | 31 |
| Urban | 2,194 | 49.3 | Female | 59 | 32 |
| Urban | 1,557 | 65.7 | Male | 68 | 43 |
| Urban | 1,723 | 55 | Female | 48 | 13 |
| Urban | 1,701 | 60.1 | Female | 66 | 41 |
| Urban | 1,996 | 44.2 | Female | 34 | 10 |
| Variable | Category | n | % (M ± SD) |
|---|---|---|---|
| Sex | Female | 825 | 58.0 |
| Male | 598 | 42.0 | |
| Age (years) | 52.6 ± 17.2 (range: 9–100) | ||
| Age groups | ≤35 | 209 | 14.7 |
| 36–50 | 488 | 34.3 | |
| 51–65 | 357 | 25.1 | |
| ≥66 | 369 | 25.9 | |
| COVID-19 vaccination | 0 doses | 459 | 32.3 |
| 1 dose | 106 | 7.4 | |
| 2 doses | 544 | 38.2 | |
| 3 doses | 289 | 20.3 | |
| ≥4 doses | 25 | 1.8 | |
| History of COVID-19 | Yes | 1,172 | 82.4 |
| No | 251 | 17.6 | |
| Number of infections ( | 0 (never infected) | 251 | 17.6 |
| 1 | 688 | 48.3 | |
| 2 | 297 | 20.9 | |
| 3 | 48 | 3.4 | |
| 4 | 139 | 9.8 | |
| COVID-19 severity ( | 1 - Asymptomatic | 116 | 8.2 |
| 2 - Mild | 932 | 65.5 | |
| 3 – Moderate | 76 | 5.3 | |
| 4 - Severe | 24 | 1.7 | |
| 5 -Critical | 7 | 0.5 | |
| 6 -Death | 17 | 1.2 | |
| COVID-19 severity ≥3 | 124 | 10.6 | |
|
|
|
| ||
|---|---|---|---|---|
|
|
|
|
| |
| Arterial hypertension | 355 | 24.9 | 32 | 2.2 |
| Cardiovascular diseases (except arterial hypertension) | 182 | 12.8 | 37 | 2.9 |
| Pulmonary disease | 60 | 4.2 | 18 | 1.3 |
| Gastrointestinal | 76 | 5.4 | 7 | 0.5 |
| Thyroid diseases | 74 | 6.2 | 17 | 1.2 |
| Musculoskeletal diseases | 71 | 5.0 | 24 | 1.9 |
| Kidney disease | 17 | 1.2 | 2 | 0.2 |
| Malignant disease | 76 | 5.3 | 15 | 1.1 |
| Diabetes mellitus | 58 | 4.1 | 13 | 0.9 |
| Neurological disorders | 32 | 2.2 | 67 | 4.7 |
| Obesity | 58 | 4.1 | 38 | 2.7 |
| Mental health | 81 | 5.7 | 37 | 2.6 |
|
|
|
|
|---|---|---|
|
| 70 | 4.9 |
| Shortness of breath | 40 | 28 |
| Neurological disorders | 67 | 4.7 |
| Mental health disorders | 37 | 2.6 |
| Obesity | 38 | 2.7 |
| Diabetes | 13 | 0.9 |
| Pulmonary thromboembolism | 14 | 1.0 |
| Number of vaccine doses | No chronic disease | ≥1 chronic disease (n) | Total | ||
|---|---|---|---|---|---|
|
| % |
| % | ||
| 0 doses | 272 | 69.7 | 118 | 30.3 | 390 |
| 1 dose | 65 | 77.4 | 19 | 22.6 | 84 |
| 2 doses | 335 | 75.1 | 111 | 24.9 | 446 |
| ≥3 doses | 145 | 57.5 | 107 | 42.5 | 252 |
| Total | 817 | 69.7 | 355 | 30.3 | 1,172 |
| Predictor |
| 95% CI |
|
|---|---|---|---|
| (Constant) | 1.965 | [1.857, 2.073] | <0.001 |
| Pulmonary disease (yes) | 0.219 | [0.020, 0.417] | 0.031 |
| Age 36–50 years | 0.127 | [0.001, 0.253] | 0.049 |
| Age 51–65 years | 0.310 | [0.174, 0.445] | <0.001 |
| Age ≥66 years | 0.504 | [0.368, 0.642] | <0.001 |
| Vaccinated (yes) | −0.207 | [−0.297, −0.118] | <0.001 |
| Model fit: | |||
| Variable | Cardiovascular diseases OR (95% CI) |
| Musculoskeletal diseases OR (95% CI) |
| Pulmonary thromboembolism OR (95% CI) |
| Pulmonary diseases OR (95% CI) |
|
|---|---|---|---|---|---|---|---|---|
| Sex (male) | 0.55 (0.23–1.28) | 0.164 | 1.20 (0.52–2.79) | 0.665 | 3.65 (0.99–13.47) | 0.052* | 0.48 (0.17–1.39) | 0.178 |
| Age | — | — | — | — | — | — | — | — |
| ≥1 chronic disease | 3.17 (1.27–7.87) | 0.013** | 2.18 (0.95–5.01) | 0.067* | — | — | — | — |
| Severe COVID-19 | — | — | — | — | 69.25 (13.33–359.65) | <0.001*** | 2.98 (1.05–8.45) | 0.040** |
| Cardiovascular | — | — | — | — | 5.96 (1.03–34.39) | 0.046** | — | — |
| Musculoskeletal diseases (before COVID-19) | 3.28 (1.29–8.32) | 0.012** | — | — | 7.78 (1.03–58.67) | 0.047** | — | — |
| Pulmonary diseases (before COVID-19) | — | — | — | — | 3.51 (0.76–16.06) | 0.106 | — | — |
| Arterial hypertension | 2.70 (1.12–6.50) | 0.027** | — | — | 0.13 (0.02–0.93) | 0.042** | 4.70 (1.72–12.80) | 0.002*** |
| Obesity | — | — | — | — | — | — | — | — |
| COVID-19 vaccination | — | — | 0.26 (0.11–0.61) | 0.002*** | 0.31 (0.09–1.09) | 0.067* | 0.42 (0.16–1.09) | 0.074* |
| Model fit | LR χ2(4) = 38.39; | LR χ2(3) = 13.36; | LR χ2(6) = 54.37; | LR χ2(4) = 19.24; | ||||
| Variable | Gastrointestinal diseases OR(95% CI) |
| Thyroid diseases OR (95% CI) |
| Arterial hypertension (after COVID-19) OR (95% CI) |
| Diabetes (after COVID-19) OR (95% CI) |
|
|---|---|---|---|---|---|---|---|---|
| Sex (male) | — | — | 0.31 (0.09–1.09) | 0.068* | — | — | — | — |
| Age | — | — | — | — | 1.01 (0.99–1.03) | 0.315 | — | — |
| ≥1 chronic disease | — | — | — | — | — | — | — | — |
| Severe COVID-19 | 12.45 (2.11–73.41) | 0.005*** | 2.98 (1.05–8.45) | 0.040** | — | — | — | — |
| Cardiovascular diseases (before COVID-19) | 30.04 (4.31–209.38) | 0.001*** | — | — | 0.40 (0.09–1.85) | 0.243 | — | — |
| Musculoskeletal diseases (before COVID-19) | — | — | — | — | — | — | 5.60 (1.49–21.02) | 0.011** |
| Pulmonary diseases (before COVID-19) | — | — | 3.51 (0.76–16.06) | 0.106 | — | — | — | — |
| Arterial hypertension | 0.04 (0.00–0.62) | 0.022** | — | — | — | — | — | — |
| Obesity | 8.31 (0.78–88.92) | 0.080* | — | — | 3.27 (1.10–9.76) | 0.034** | 1.94 (0.24–15.56) | 0.534 |
| COVID-19 vaccination | — | — | 0.42 (0.16–1.10) | 0.079* | — | — | 0.41 (0.14–1.23) | 0.112 |
| Model fit | LR | LR χ2(3) = 8.75; | LR χ2(3) = 5.33; | LR χ2(3) = 7.45; | ||||
| Variable | Brain fog OR (95% CI) |
| Psychiatric disorders OR (95% CI) |
| Dyspnea OR (95% CI) |
|
|---|---|---|---|---|---|---|
| Sex (male) | 0.600 (0.34–1.05) | 0.073* | 1.578 (0.77–3.23) | 0.211 | 0.718 (0.35–1.48) | 0.370 |
| Number of COVID-19 vaccinations | 1.839 (1.44–2.36) | <0.001*** | — | — | — | — |
| Number of COVID-19 infections | — | — | 1.311 (0.97–1.78) | 0.082* | 0.958 (0.66–1.39) | 0.819 |
| ≥1 chronic disease | 1.096 (0.77–1.56) | 0.610 | — | — | 0.056 (0.01–0.24) | <0.001*** |
| Cardiovascular diseases | 1.305 (0.55–3.10) | 0.546 | — | — | — | — |
| Thyroid diseases | 0.500 (0.12–2.15) | 0.352 | — | — | — | — |
| Diabetes | 3.034 (1.07–8.62) | 0.037** | 1.798 (0.49–6.62) | 0.378 | — | — |
| Neurological disorders | 0.701 (0.09–5.55) | 0.736 | 4.106 (1.08–15.56) | 0.038* | — | — |
| Obesity | 2.593 (1.03–6.52) | 0.043** | — | — | 2.463 (0.69–8.86) | 0.167 |
| Severe COVID-19 (≥3) | — | — | — | — | 4.876 (2.18–10.89) | <0.001*** |
| Pulmonary diseases | — | — | — | — | 13.248 (4.43–39.60) | <0.001*** |
| Model fit | LR χ2(8) = 39.60; | LR χ2(4) = 9.82; | LR χ2(6) = 45.30; | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLong-Term Effects of COVID-19 · COVID-19 Clinical Research Studies · COVID-19 and Mental Health
Introduction
1
The COVID-19 pandemic, caused by the SARS-CoV-2 virus, has posed a significant challenge to healthcare systems worldwide. A growing body of evidence indicates that the impact of SARS-CoV-2 infection does not necessarily end with viral clearance. Numerous studies have demonstrated that SARS-CoV-2 infection can lead to long-term health consequences that persist well beyond the acute phase of disease (1).
The World Health Organisation (WHO) developed a clinical case definition for post-COVID-19 condition—commonly known as “long COVID”—using a Delphi consensus process involving global experts. Post-COVID-19 condition occurs in individuals with a history of probable or confirmed SARS-CoV-2 infection, usually 3 months from the onset of COVID-19, with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis (2). The NASEM Committee recently updated the definition of long COVID, emphasizing three key changes to improve understanding and recognition. The definition explains that the phrase “long COVID” is widely recognized and easy for both the public and healthcare professionals to understand. Long COVID is now considered part of a broader category of illnesses that can occur after infections (3). However, Croatia does not have a national long COVID clinical guideline for healthcare professionals with a standardized diagnostic protocol. Depending on the affected organ system and the severity of symptoms, GPs refer patients to a neurologist, cardiologist, etc. The Croatian healthcare system has developed a set of national recommendations and educational materials addressing post-COVID-19 condition, primarily coordinated by the Croatian Institute of Public Health (4). These documents aim to support both healthcare professionals and patients in the recognition, assessment, and management of persistent symptoms after SARS-CoV-2 infection.
Outpatient clinics for the care of patients with post-COVID symptoms have been established in several Croatian hospitals, including a pediatric outpatient clinic, as well as a post-COVID day hospital for physical and rehabilitation medicine. However, the absence of fully standardized national clinical pathways highlights the ongoing need for further systematization, research, and evaluation of post-COVID-19 care models.
The clinical course and outcomes of SARS-CoV-2 infection vary widely among individuals, ranging from asymptomatic to severe disease requiring hospitalization and intensive care. Earlier research has identified multiple risk factors for severe forms of SARS-CoV-2 infection, particularly chronic diseases (5). Previous studies have examined the associations between SARS-CoV-2 infection and incidence of newly developed chronic conditions, such as diabetes mellitus, cardiovascular, neurological and psychiatric diseases (6–9).
The introduction of vaccination against SARS-CoV-2 infection played a key role in controlling the pandemic, but vaccination acceptance was heterogeneous. COVID-19 vaccination behavior depended on several individual and health characteristics, including the presence of comorbidities. Apart from the severity of symptoms, the consequences of the SARS-CoV-2 infection can also vary (10). Despite extensive research on vaccine efficacy and determinants of severe disease, less is known about how chronic diseases before and after SARS-CoV-2 infection affect two key outcomes: the number of vaccine doses received and the severity of SARS-CoV-2 infection.
Epidemiological data indicate that both brain fog and mental health disorders affect approximately one in five individuals within 3 months to 2 years post-infection, underscoring a significant public health concern (11). Frequent symptoms include fatigue, shortness of breath, and cognitive dysfunction (often referred to as brain fog), which generally have an impact on everyday functioning. Symptoms may be new-onset following initial recovery from an acute COVID-19 episode or persist from the initial illness (12, 13).
Mental health conditions included diagnosed mental illness as well as symptoms such as anxiety or low mood, associated with distress or impairment in functioning or future incidence of full disorder without reaching the full criteria for a mental disorder at that time (11).
This study aimed to assess the prevalence and risk factors for the development of post-COVID symptoms and diseases in the general population, taking into account pre-existing chronic diseases and the severity of the clinical picture of SARS-CoV-2 infection. Particular attention was given to the occurrence of brain fog and shortness of breath and their associations with disease severity, vaccination status and comorbidities.
Methods
2
Data collection
2.1
This retrospective cross-sectional study was conducted in Croatia. The study included 10 family medicine practices selected through systematic convenience sampling. The study was not designed to achieve national representativeness. A systematic sample was used, with every tenth patient from the list (in alphabetical order) included in the analysis. The data collected from medical records included patients’ gender, age, COVID-19 vaccination status, history and severity of SARS-CoV-2 infection/s, and documented diseases and symptoms/disorders occurring before and after the SARS-CoV-2 infection.
Since the COVID-19 pandemic was officially declared in Croatia in March 2020, data on infection rates and disease severity were systematically tracked until the pandemic formally concluded in May 2023.
Chronic comorbidities were grouped by organ systems. Arterial hypertension, diabetes and obesity were observed separately. Post-COVID outcomes included self-reported new-onset symptoms such as neurological disorders (headache, persisting smell/taste abnormalities, slowness of movement, peripheral neuropathy, sleep disturbances, tinnitus), brain fog, shortness of breath, and mental health conditions. A cutoff point of 12 weeks was used to extract and analyze the relevant data after acute SARS-CoV-2 infection.
The severity of the SARS-CoV-2 infection was determined based on the clinical assessment from the medical documentation. Disease severity was assessed according to clinical criteria outlined in the Croatian Ministry of Health’s Guidelines for the Treatment of Patients with COVID-19, Version 2, dated November 19, 2020 (14). Based on the symptoms of the disease, the patients were divided into 6 groups: asymptomatic, mild (various symptoms, fever, general malaise, headache, myalgia, runny nose, sore throat and/or cough), moderate (severe symptoms of the disease and/or pneumonia, without the need for oxygen replacement therapy – SpO2 > 93% on room air), severe (respiratory frequency >30 breaths/min, respiratory failure or the need for oxygen replacement therapy – SpO2 ≤ 93% on room air), critical (criteria for ARDS, sepsis, septic shock, with/without acute dysfunction of other organ systems-shock, renal failure, coagulopathy, impaired consciousness) and patients with a fatal outcome.
Data analysis
2.2
The normality of the distribution of numerical variables was tested using the Kolmogorov–Smirnov test, which did not show a significant deviation from normality (p > 0.05). Therefore, parametric statistical methods were used, and values were presented as means ± standard deviations (SD) for continuous variables and as absolute and frequencies (n, %) for categorical variables.
In univariate analyses, the independent samples t-test and χ^2^ test of independence were applied, depending on the type of variable. Variables that showed statistical significance (p < 0.05) were included in the multivariate logistic regression analysis. Multiple linear regression analysis was used to identify predictors of SARS-CoV-2 infection severity, while binary logistic regression was applied to examine factors associated with post-COVID conditions.
COVID-19 vaccination was operationalized differently across regression models depending on the outcome of interest. For analyses of post-COVID clinical conditions, vaccination status was included as a binary variable (vaccinated vs. unvaccinated), reflecting clinically relevant exposure. For analyses of neurocognitive and subjective post-COVID symptoms, such as brain fog, the number of COVID-19 vaccine doses was included as a continuous variable to explore potential dose–response associations.
Age and sex were included as covariates in all binary logistic regression models. Variables that were not statistically significant (p > 0.05) and whose exclusion did not change the remaining coefficients by more than 10% were removed, and parsimonious models including clinically relevant predictors were presented.
Analyses were performed in the IBM SPSS Statistics version 24.0 and Stata version 15.0. The results of the logistic regression are presented as odds ratios (OR) with the corresponding 95% confidence intervals (CI), and p values < 0.05 were considered statistically significant.
Results
3
The study was conducted in 10 family medicine practices, including five located in urban areas and five in rural areas. Table 1 presents the characteristics of the physicians who participated in the survey.
Study population characteristics
3.1
The study included 1,423 subjects, of whom 58.0% were female. The mean age of the participants was 52.6 ± 17.2 years (range 9–100). The largest number of subjects belonged to the 36–50-year age group (34.3%), while the smallest number was younger than 35 years (14.7%). Of the total number of subjects, 82.4% had a confirmed SARS-CoV-2 infection. Almost two-thirds of those infected described the course of the disease as mild (65.5%), while a moderate-to-severe form of the disease (≥3 according to the severity scale) was recorded in 10.6% of cases. An asymptomatic course was observed in 8.2% of subjects, and a critical form of the disease was recorded in 0.5% of cases. Regarding vaccination against COVID-19, 32.3% of respondents did not receive any dose of the vaccine, and 38.2% of respondents had two doses. Twenty percent of respondents received three doses, while 1.8% received four or more doses (Table 2).
Pre-existing comorbidities and newly diagnosed conditions after SARS-CoV-2 infection
3.2
Before the SARS-CoV-2 infection, 71.9% of respondents had no chronic condition, while 28.1% had at least one chronic disease. The most frequently reported comorbidities were arterial hypertension (24.9%), cardiovascular diseases (12.8%), and thyroid disorders (6.2%). After recovering from the infection, the most frequently reported post-COVID symptoms were brain fog (4.9%) and shortness of breath (2.8%). Of the newly diagnosed diseases after infection, the most common were neurological (4.7%) and cardiovascular (2.9%) diseases, followed by obesity (2.7%) and mental health disorders (2.6%) (Tables 3, 4).
Vaccination status and comorbidity patterns
3.3
Chronic diseases were more common in multiply vaccinated subjects, especially in those with three or more doses (over 40%) (Table 5). The χ^2^ test of independence showed a significant association between the number of vaccinations and the presence of chronic diseases [χ^2^(6, N = 1,172) = 31.01, p < 0.001, Cramer’s V = 0.163], and as the number of vaccinations increases, the proportion of subjects with at least one chronic disease also increases. Specifically, while 30.3% of unvaccinated subjects had a chronic disease, among those with three or more doses, this proportion increases to more than 40%.
The highest vaccination rates were observed among patients with malignant diseases (79.7%) and diabetes (79.3%), followed by chronic kidney disease patients (76.5%) and chronic respiratory diseases (73.3%).
Factors associated with COVID-19 severity
3.4
The results showed that pulmonary disease was a significant positive predictor of disease severity (β = 0.22, 95% CI [0.02, 0.42], p = 0.031). Compared with the reference group under 35 years of age, people aged 51–65 years (β = 0.31, 95% CI [0.17, 0.44], p < 0.001) and 66 years and older (β = 0.50, 95% CI [0.37, 0.64], p < 0.001) had significantly more severe COVID-19, while the group 36–50 years showed a trend toward more severe disease (β = 0.13, p = 0.049).
Vaccination was a significant negative predictor of disease severity (β = −0.21, 95% CI [−0.30, −0.12], p < 0.001), indicating that vaccinated individuals had a milder form of COVID-19 (Table 6).
Factors associated with post-COVID cardiovascular, musculoskeletal, pulmonary thromboembolism, and pulmonary diseases
3.5
Binary logistic regression analysis was performed to examine factors associated with the occurrence of cardiovascular disease, musculoskeletal disease, pulmonary thromboembolism, and pulmonary disease after SARS-CoV-2 infection.
Cardiovascular disease
3.5.1
Individuals with at least one chronic disease were more likely to develop cardiovascular complications (OR = 3.17; 95% CI 1.27–7.87; p = 0.013). Musculoskeletal disease before SARS-CoV-2 infection was also associated with an increased risk (OR = 3.28; 95% CI 1.29–8.32; p = 0.012), as was arterial hypertension (OR = 2.70; 95% CI 1.12–6.50; p = 0.027).
Musculoskeletal disorders
3.5.2
The presence of at least one chronic disease was associated with a higher likelihood of developing musculoskeletal disorders after SARS-CoV-2 infection (OR = 2.18; 95% CI 0.95–5.01; p = 0.067). COVID-19 vaccination showed a significant protective effect, as vaccinated individuals were less likely to develop musculoskeletal disorders in the post-COVID period (OR = 0.26; 95% CI 0.11–0.61; p = 0.002).
Pulmonary thromboembolism
3.5.3
Moderate-to-severe COVID-19 was strongly associated with an increased risk of pulmonary thromboembolism compared with milder forms of the disease (OR = 69.25; 95% CI 13.33–359.65; p < 0.001). Previous cardiovascular disease before COVID-19 (OR = 5.96; 95% CI 1.03–34.39; p = 0.046) and musculoskeletal disease before COVID-19 (OR = 7.78; 95% CI 1.03–58.67; p = 0.047) were significant predictors. In contrast, arterial hypertension before COVID-19 was associated with a lower risk of pulmonary thromboembolism (OR = 0.13; 95% CI 0.02–0.93; p = 0.042). COVID-19 vaccination showed a non-significant trend toward a protective effect (OR = 0.31; 95% CI 0.09–1.09; p = 0.067).
Pulmonary disease
3.5.4
Severe COVID-19 was associated with an increased likelihood of developing pulmonary disease after infection (OR = 2.98; 95% CI 1.05–8.45; p = 0.040). Arterial hypertension before COVID-19 was also a significant predictor (OR = 4.70; 95% CI 1.72–12.80; p = 0.002). Although statistical significance was not reached, COVID-19 vaccination showed a trend toward a reduced risk of pulmonary disease (OR = 0.42; 95% CI 0.16–1.09; p = 0.074) (Table 7).
Factors associated with post-COVID gastrointestinal, endocrine, and cardiovascular conditions
3.6
Binary logistic regression analysis was performed to examine factors associated with the occurrence of gastrointestinal diseases, thyroid diseases, arterial hypertension and diabetes after SARS-CoV-2 infection.
Gastrointestinal diseases
3.6.1
The analysis showed that severe COVID-19 (p = 0.005) and previous cardiovascular disease (p = 0.001) significantly increased the risk of developing gastrointestinal diseases after infection. Severe COVID-19 was associated with a higher likelihood of developing gastrointestinal diseases after infection (OR = 12.45; 95% CI 2.11–73.41; p = 0.005).
Thyroid diseases
3.6.2
Men were less likely than women to develop thyroid disease after COVID-19 (OR = 0.31, 95% CI [0.09–1.09], p = 0.068). Vaccination also showed a protective trend (OR = 0.42, 95% CI [0.16–1.10], p = 0.079). Although no predictor reached statistical significance, the observed trends suggest a higher propensity for post-COVID thyroid dysfunction in women and a potential protective effect of vaccination.
Cardiovascular diseases and arterial hypertension
3.6.3
Individuals with cardiovascular disease before COVID-19 had a markedly increased risk (OR = 30.04; 95% CI 4.31–209.38; p = 0.001). Among the predictors analyzed, obesity was a significant risk factor (OR = 3.27, 95% CI [1.10–9.76], p = 0.034).
Obesity and diabetes
3.6.4
Obesity before COVID-19 showed a trend toward increased gastrointestinal risk (OR = 8.31; p = 0.080), whereas arterial hypertension before COVID-19 was protective (OR = 0.04; p = 0.022). Pulmonary diseases were associated with a higher, but not statistically significant, risk (OR = 3.51, 95% CI [0.76–16.06], p = 0.106). Individuals who had musculoskeletal diseases before infection were significantly more likely to develop diabetes after COVID (OR = 5.60, 95% CI [1.49–21.02], p = 0.011) (Table 8).
Factors associated with brain fog, psychiatric disorders, and dyspnea after COVID-19
3.7
Brain fog
3.7.1
In the logistic regression model for the occurrence of brain fog, the number of doses of the COVID-19 vaccine received, the presence of diabetes and obesity were significant predictors. Respondents who received a higher number of vaccine doses were 1.84 times more likely (OR = 1.839; 95% CI: 1.44–2.36; p < 0.001) to develop brain fog compared to those who received fewer doses. People with diabetes were three times more likely to develop brain fog (OR = 3.03; 95% CI: 1.07–8.62; p = 0.037), while obesity was also a significant predictor (OR = 2.59; 95% CI: 1.03–6.52; p = 0.043) - obese respondents were about 2.6 times more likely to develop brain fog. Men showed about 40% lower probability of brain fog compared to women, but with a low level of significance (Table 9).
Mental health disorders
3.7.2
In the model for the occurrence of mental health disorders after SARS-CoV-2 infection, the presence of neurological disorders was shown to be a significant predictor; respondents were approximately four times more likely to develop a mental health disorder compared to those without neurological comorbidities (OR = 4.11; 95% CI: 1.08–15.56; p = 0.038). The number of SARS-CoV-2 infections showed a borderline significant association (p = 0.082), with each additional infection increasing the likelihood of mental health disorder by approximately 31% (OR = 1.31; 95% CI: 0.97–1.78) (Table 9).
Shortness of breath
3.7.3
The most important predictors for the occurrence of shortness of breath after recovering from SARS-CoV-2 infection were the severity of the acute infection, the presence of chronic pulmonary disease and the status of comorbidities. Subjects who had a moderate or severe form of the disease (severity ≥ 3) were almost five times more likely to have shortness of breath (OR = 4.86; 95% CI: 2.20–10.72; p < 0.001). Pulmonary disease was the strongest predictor, whereby subjects with this diagnosis had as much as 13 times greater odds of developing shortness of breath (OR = 13.78; 95% CI: 4.62–41.09; p < 0.001).
On the other hand, the presence of at least one chronic disease (other than pulmonary) was shown to be a protective factor, as such subjects were approximately 95% less likely to develop shortness of breath compared to subjects without comorbidities (OR = 0.053; 95% CI: 0.012–0.226; p < 0.001). Obesity was not a significant predictor (p = 0.187), although obese subjects were approximately 2.4 times more likely to develop dyspnea (Table 9).
Odds ratios from the logistic regression analyses are additionally presented as forest plots in the Supplementary material (Figures 1–3).
Forest plots showing odds ratios (OR) and 95% confidence intervals for factors associated with post-COVID cardiovascular diseases, musculoskeletal diseases, pulmonary thromboembolism, and pulmonary diseases. The vertical dashed line indicates OR = 1. All x-axes are presented on a logarithmic scale.
Forest plots showing odds ratios (OR) and 95% confidence intervals for factors associated with post-COVID gastrointestinal diseases, thyroid diseases, arterial hypertension, and diabetes. The vertical dashed line indicates OR = 1. All x-axes are presented on a logarithmic scale.
Forest plots showing odds ratios (OR) and 95% confidence intervals for factors associated with brain fog, psychiatric disorders, and dyspnea after COVID-19. The vertical dashed line indicates OR = 1. All x-axes are presented on a logarithmic scale.
Discussion
4
This study provides valuable insights into the prevalence and risk factors for the development of post-COVID symptoms and diseases in the general population. The findings suggest that while the overall prevalence of post-COVID symptoms is relatively low, they continue to represent a significant public health concern, particularly in terms of their long-term consequences.
The study found that nearly 25% of patients had arterial hypertension before SARS-CoV-2 infection, and almost 13% had other cardiovascular diseases. A total of 4.2% of participants suffered from pulmonary disease before SARS-CoV-2 infection. The analysis showed that chronic pulmonary disease was strongly associated with the severity of SARS-CoV-2 infection. Other studies have demonstrated that conditions such as diabetes, hypertension, coronary heart disease and chronic lung disease significantly increase the risk of severe forms of COVID-19 (5). As these comorbidities can impair immune responses and elevate the risk of complications, their presence further complicates recovery from SARS-CoV-2 infection and contributes to the long-term burden of the disease (15).
The study confirmed that COVID-19 vaccination was a protective factor against severe forms of COVID-19 infection and the development of certain long-term conditions, including musculoskeletal diseases, pulmonary thromboembolism, and pulmonary and thyroid diseases.
In addition to severe COVID-19, our results indicate that male gender, as well as previous cardiovascular and musculoskeletal disease, increase the risk of developing a pulmonary thromboembolic incident. Meta-analyses highlight diabetes and malignant disease as risk factors (16).
Hypertension is known to be associated with post-COVID pulmonary embolism (17), but in our study, arterial hypertension was shown to have a protective effect.
In our study, obesity was shown to be a significant factor associated with both brain fog and hypertension. Previous research has similarly shown that obesity can exacerbate the severity of COVID-19 and increase the risk of severe outcomes, including ICU admission and mortality (18). Our results confirm that obesity may be a critical factor in the development of post-COVID cognitive dysfunction, likely due to its impact on metabolic processes and inflammation.
The analysis showed that patients with diabetes, malignancies, chronic kidney and pulmonary disease had higher vaccination rates. This may indicate increased awareness of risk among these patient groups or more proactive health recommendations from healthcare providers.
More than 10% of patients who recovered from SARS-CoV-2 infection developed a chronic illness that is classified as a psychiatric or neurological disorder. Comparing our findings with previous international studies, it is observed that the prevalence of symptoms such as brain fog (4.9%) and shortness of breath (2.8%) in this general population sample are consistent with UK population-based studies reporting post-COVID symptom rates of approximately 2–6% (19).
In the systematic review van der Feltz-Cornelis et al. concluded that mental health conditions and brain fog both occur in around one in five patients between 3 months and 2 years after SARS-CoV-2 infection and show that the odds of brain fog significantly decreased with increasing vaccination rates (11). An interesting finding of this study is the association between several vaccine doses received and more frequent reporting of brain fog symptoms. Although our result may seem contradictory, it is important to emphasize that a causal relationship has not been proven. This association may reflect a higher level of health awareness and willingness of vaccinated subjects to recognize and report symptoms. Another important interpretation of the observed association is that vaccinated groups disproportionately included older adults and individuals with chronic conditions, populations that are inherently more likely to experience and report cognitive symptoms. Vaccine uptake was highest among older participants and those with comorbidities, suggesting that the association with brain fog may reflect underlying demographic and clinical differences rather than a direct effect of vaccination.
Numerous studies indicate a protective effect of vaccination on the occurrence of post-COVID symptoms. Research in Israel has shown that an mRNA vaccine may be associated with a reduced prevalence of reported post-acute SARS-CoV-2 infection symptoms (20).
A study from Norway has also shown that booster vaccination before SARS-CoV-2 infection was associated with a marked reduction in both neurocognitive and cardiorespiratory symptoms persisting for at least 3 months after Omicron infection (21).
Krishna et al. concluded that long COVID has declined markedly in the United Kingdom following vaccine rollout. Although vaccination does not alter the symptom profile, it is associated with reduced symptom severity. These findings suggest that pre-infection immunity lowers long COVID risk, likely through attenuation of acute disease and its sequelae (22).
It is known that cognitive impairment after COVID-19 may be mediated by metabolic and neuroinflammatory processes, which explains the higher frequency of symptoms in people with diabetes and obesity (23). These findings indicate the need for a holistic approach to assessing the post-COVID state, with the family doctor playing a key role in identifying patients at risk.
Research conducted in hospital settings, as expected, revealed a higher prevalence of dyspnea compared to our outpatient sample (24). A meta-analysis on the prevalence of post-COVID breathlessness revealed that 26% of COVID-19 survivors reported the presence of breathlessness symptoms more than 4 weeks post-infection, and 41% of survivors reported reduced physical capacity due to post-COVID breathlessness, as assessed by the MRC/mMRC dyspnoea scale (25). The lower prevalence observed in our sample may be attributed to the milder clinical presentations of infection and the relatively smaller proportion of patients with chronic pulmonary conditions. The results also confirm that dyspnea is one of the most important post-COVID symptoms, especially in people who had a more severe form of acute illness or previous lung disease. Similar associations between the severity of the acute phase and persistent respiratory distress have been found in a review article by Morgan et al. which emphasized that the strongest predictive risk factors for persistent dyspnea included pulmonary comorbidities, the severity of the SARS-CoV-2 infection, female sex, elevated body mass index, pre-existing anxiety and depression, pre-COVID physical limitations, and socioeconomic differences (26). These data further emphasize the importance of systematic monitoring of respiratory function during the recovery period, especially in primary health care, where most patients seek help after discharge from the hospital or after a mild infection at home.
The presence of chronic disease in our results is a protective factor in the development of dyspnea, which can be explained by the fact that people with chronic diseases are usually under more frequent medical supervision and therefore recognize and control respiratory disorders earlier.
The association of neurological and psychiatric disorders after COVID-19 is supported by a growing body of evidence on the neuropsychiatric effects of infection (27). Various theories explaining long COVID, such as direct neuro-invasion, systemic effects of the virus, and neuroimmune dysregulation, have been suggested. Social isolation and associated factors also serve as the link between the SARS-CoV-2 virus, long COVID and its neuropsychiatric manifestations (28). Such patients are particularly vulnerable and require a proactive approach to monitoring and psychosocial support.
From a clinical perspective, family physicians play a crucial role in the early identification and long-term follow-up of patients with post-COVID symptoms (29). As a multisystem disorder, SARS-CoV-2 infection has negative impacts on the physical and mental health of people, as well as their ability to work, so the Croatian Ministry of Health made a guideline for post-COVID rehabilitation. These rehabilitation programs include breathing exercises, physical therapy, psychological support, occupational therapy, education on self-management,etc. in special hospitals for medical rehabilitation, health resorts and thermal spas. The first official Croatian guide for patients recovering from long COVID, which also serves as a guide for health professionals, explains common post-COVID symptoms and how to manage them. The guide offers several benefits for clinical practice: provides a description of common post-COVID symptoms, supports continuity of care and allows healthcare professionals to educate patients on effective self-care strategies (30). Primary care represents the first line of contact for most patients, enabling an integrated approach that encompasses the biomedical, psychological, and social aspects of health. Regular check-ups, assessment of symptoms and coordination of care with other specialists (neurologist, pulmonologist, psychiatrist) can significantly improve patient outcomes and quality of life.
Limitations
5
While this study offers important insights into the prevalence and factors influencing post-COVID conditions, several limitations should be considered.
First, the retrospective design of the study may introduce bias, particularly in the recording of diagnoses and the assessment of disease severity. The severity of SARS-CoV-2 infection was determined based on medical documentation, which may not always reflect the full clinical picture, especially in cases with subtle or evolving symptoms. Additionally, as a cross-sectional study, it does not allow for conclusions about causality, particularly regarding the long-term health outcomes of post-COVID conditions. Another limitation is the lack of precise data on the time elapsed between SARS-CoV-2 infection and assessment of post-COVID symptoms. As participants were assessed at varying stages of post-infection recovery, symptom prevalence could not be analyzed by follow-up duration, which should be considered when interpreting the findings.
Fatigue, despite being one of the most common and well-documented post-COVID symptoms, was not specifically assessed in our study. The symptom questionnaire focused primarily on organ-specific symptoms routinely recorded in primary care, and therefore fatigue was not included as a separate variable. This should be considered a limitation when interpreting the prevalence of post-COVID symptoms in our cohort.
The relatively small number of participating practices and the non-random sampling approach limit the generalizability of the findings. Although practices from different regions and settings were included, the sample cannot be considered nationally representative. Potential selection bias cannot be excluded and should be considered when interpreting the results.
Conclusion
6
This study provides comprehensive insights into the long-term health effects of SARS-CoV-2 infection in Croatian primary care settings, highlighting the multifaceted nature of post-COVID conditions. Pre-existing chronic diseases, older age, and obesity emerged as significant risk factors for more severe acute COVID-19 and the subsequent development of long-term complications, including neurological, psychiatric, cardiovascular, pulmonary, and metabolic sequelae. Notably, COVID-19 vaccination demonstrated consistent protective effects against severe disease and certain post-COVID conditions, underscoring its critical role in mitigating long-term health impacts.
Although the overall prevalence of post-COVID symptoms in the general population was lower than in hospitalized patients, cognitive dysfunction, dyspnea, and other persistent symptoms remain substantial public health concerns. The study also revealed nuanced associations, such as the increased reporting of brain fog among individuals with higher vaccination doses, likely reflecting heightened health awareness and underlying demographic and clinical factors rather than a causal effect. These findings reinforce the complex interplay between pre-existing conditions, vaccination, and post-COVID outcomes, particularly in populations with metabolic and chronic health conditions where inflammatory and neuroimmune pathways may drive symptom persistence.
Family physicians are uniquely positioned to provide comprehensive, patient-centered care that integrates biomedical, psychological, and social aspects. Early identification of at-risk patients, systematic monitoring of symptoms, and timely interventions can mitigate complications, improve functional outcomes, and reduce the long-term burden of post-COVID conditions on both patients and healthcare systems. This study emphasizes the importance of vigilant, targeted preventive strategies and the central role of primary care in managing post-COVID health, especially in patients with chronic comorbidities.
Despite the valuable insights provided, the study’s retrospective design, lack of standardized follow-up data, absence of fatigue assessment, and non-random sample limit the generalizability of the findings. Future prospective, longitudinal studies with representative populations are essential to validate these results, clarify symptom trajectories, and further elucidate the complex relationships between pre-existing conditions, vaccination, and long-term post-COVID sequelae.
In summary, sustained vigilance, targeted immunization strategies, integrated primary care, and patient-centered follow-up are critical for addressing the enduring health consequences of SARS-CoV-2 infection and safeguarding population health.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Li J Zhou Y Ma J Zhang Q Shao J Liang S . The long-term health outcomes, pathophysiological mechanisms and multidisciplinary management of long COVID. Signal Transduct Target Ther. (2023) 8:416. doi: 10.1038/s 41392-023-01640-z, 37907497 PMC 10618229 · doi ↗ · pubmed ↗
- 2World Health Organisation. A clinical case definition of post-COVID-19 condition by a Delphi consensus, 6 October 2021. WHO, 2021. Clinical care. Available online at: https://www.who.int/publications/i/item/WHO-2019-n Co V-Post_COVID-19_condition-Clinical_case_definition-2021.1 (Accessed October 28, 2025).
- 3Ely EW Brown LM Fineberg HV. National Academies of sciences, engineering, and medicine committee on examining the working definition for long Covid. Long Covid defined. N Engl J Med. (2024) 391:1746–53. doi: 10.1056/NEJ Msb 2408466, 39083764 PMC 11687645 · doi ↗ · pubmed ↗
- 4Hrvatski zavod za javno zdravstvo In: HZJZ, editor. Povratak zdravlja i snage nakon COVID-19[Internet]. Zagreb: (2022)
- 5Liu H Chen S Liu M Nie H Lu H. Comorbid chronic diseases are strongly correlated with disease severity among COVID-19 patients: a systematic review and Meta-analysis. Ageing Dis. (2020) 11:668–78. doi: 10.14336/AD.2020.0502, 32489711 PMC 7220287 · doi ↗ · pubmed ↗
- 6Gaudet L Pillay J Saba S Zakaria D Cheta N Gardiner H . Associations between SARS-Co V-2 infection and incidence of new chronic condition diagnoses: a systematic review. Emerg Microbes Infect. (2023) 12:2204166. doi: 10.1080/22221751.2023.2204166, 37071113 PMC 10155634 · doi ↗ · pubmed ↗
- 7Xie Y Xu E Bowe B Al-Aly Z. Long-term cardiovascular outcomes of COVID-19. Nat Med. (2022) 28:583–90. doi: 10.1038/s 41591-022-01689-3, 35132265 PMC 8938267 · doi ↗ · pubmed ↗
- 8Taquet M Sillett R Zhu L Mendel J Camplisson I Dercon Q . Neurological and psychiatric risk trajectories after SARS-Co V-2 infection: an analysis of 2-year retrospective cohort studies including 1 284 437 patients. Lancet Psychiatry. (2022) 9:815–27. doi: 10.1016/S 2215-0366(22)00260-7, 35987197 PMC 9385200 · doi ↗ · pubmed ↗