Patient satisfaction with advanced practice physiotherapy internationally: A systematic mixed studies review
Chris Davis, Tim Noblet, Jodie Breach, Jai Mistry, Kaitlyn Maddigan, Katie Kowalski, Alison Rushton

TL;DR
This review evaluates patient satisfaction with advanced practice physiotherapy globally, finding that both human and system factors contribute to positive patient experiences.
Contribution
The study provides the first comprehensive synthesis of patient satisfaction with advanced practice physiotherapy across international settings.
Findings
High-confidence evidence shows human attributes like communication and competence drive patient satisfaction.
System attributes such as fast access and convenient location also contribute to satisfaction.
Quantitative evidence certainty is very low, highlighting the need for better-quality research.
Abstract
Advanced practice physiotherapy (APP) is internationally recognised as a higher level of practice involving expert clinical and analytical skills to manage complex patient needs. Patient satisfaction measures how pleased someone is with their care, comprises human and system attributes, and is an indicator of patient experience (quality). Patient satisfaction with APP appears high, but no comprehensive evidence synthesis across settings exists. Objectives were to evaluate patient satisfaction with APP internationally, and evaluate human and system attributes of patient satisfaction with APP. Systematic mixed studies review using a parallel-results convergent synthesis design. Key databases and grey literature were searched for studies measuring patient satisfaction with APP across clinical fields from inception to September 9th, 2025. Screening, data-extraction, and quality appraisal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
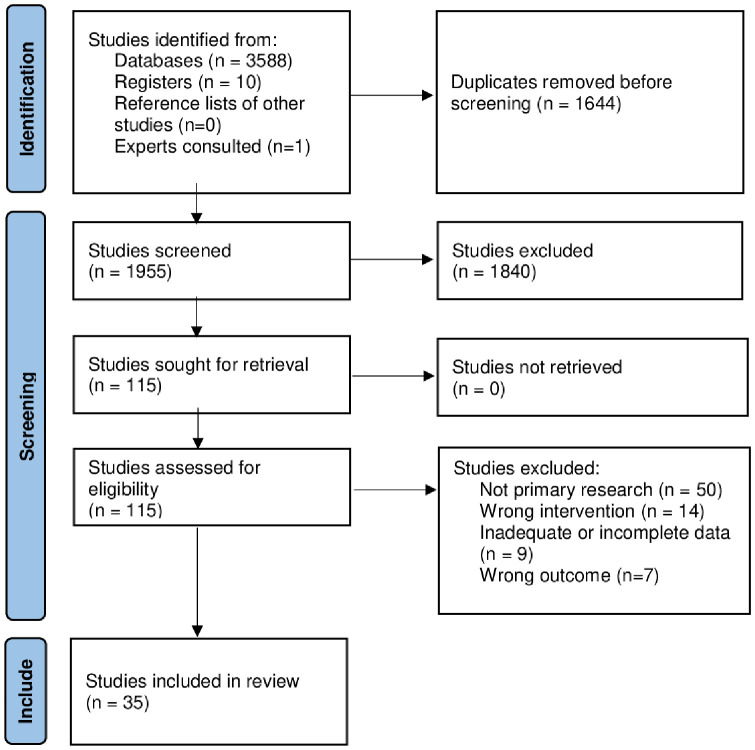 Fig 1
Fig 1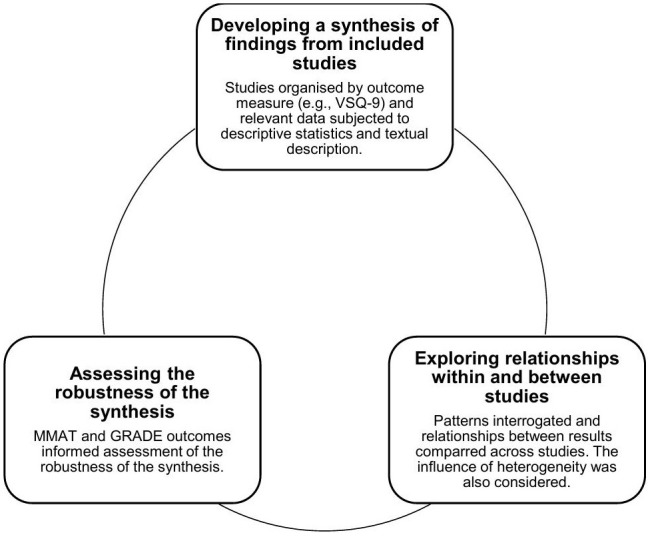 Fig 2
Fig 2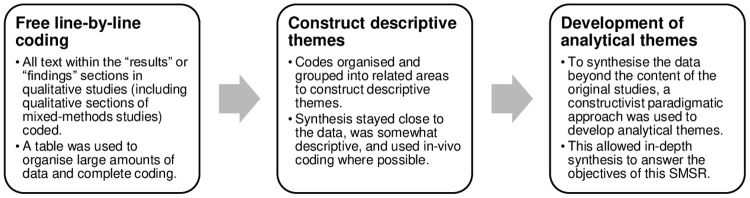 Fig 3
Fig 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNursing Roles and Practices · Occupational Therapy Practice and Research · Interprofessional Education and Collaboration
Introduction
Rationale
Advanced practice (AP) is a high level of clinical, leadership, education, and research practice, requiring autonomy and complex decision-making and existing across many professions [1]. Advanced Practice Physiotherapy (APP) evolved from US military settings in the 1970s, into at least 15 fields of practice across 14 countries globally [2,3]. In MSK settings, AP physiotherapists show diagnostic accuracy, triage appropriateness, positively impact patient outcomes, and improve access to care [4]. Furthermore, diagnostic and triage concordance between AP physiotherapists and orthopaedic or spinal surgeons is high, with comparable or greater clinical outcomes observed with APP-led models of care when compared to usual care [5,6]. Various educational pathways to APP exist including residency, fellowship, accredited or non-accredited training courses, and master’s level education, with the latter most widely accepted and likely the most comprehensive across all 4-pillars of AP [1,7]. World Physiotherapy, working officially with the World Health Organisation to represent and further the physiotherapy profession, describes APP as a higher level of practice, requiring distinctly increased clinical and analytical skills, applied to achieve improved patient outcomes and experience, in patients with complex needs [8,9]. Furthermore, World Physiotherapy recognises AP physiotherapists perform conventional physiotherapeutic tasks as well as tasks traditionally completed by other healthcare professionals (e.g., prescribing medications) [4,9]. Building on World Physiotherapy’s description of APP, Tawiah et al. (2025) propose an international definition of APP as “a broad term that refers to expert physiotherapists who employ a higher level of competencies and expertise with additional responsibilities and autonomy to manage complex and challenging health needs of individuals, families, and populations within or beyond their scope of practice. APPs demonstrate competencies as expert clinician, communicator, collaborator, leader, health advocate, scholar, and professional” (p12) [10].
Patient satisfaction is a complex phenomenon reflecting how individuals feel about their care, described as a sense of contentedness or fulfilment, that results from meeting needs and expectations [11–14]. Ng and Luk (2019) suggest patient satisfaction comprises two attributes [15]. Human attributes relate to provider attitude and technical competence, with system attributes relating to accessibility and efficacy. Similar attributes are seen in non-clinical settings, with reference to relational (emotional benefits from social interaction) and functional (service efficiency) dimensions of service quality [16]. Patient satisfaction is measured using questionnaires, patient-reported outcome measures, or experience measures, and importantly is an indicator of patient experience [14,17,18]. Patient experience, defined as “the sum of all interactions, shaped by an organisation’s culture, that influence patient perceptions, across the continuum of care” [19], is a valuable measure of healthcare quality [12,14].
Research investigating patient satisfaction with APP lacks comprehensive analysis and is often a briefly reported secondary objective in systematic reviews investigating models of care. In this research, high patient satisfaction is found across outpatient musculoskeletal (MSK), spinal pain, emergency department, and orthopaedic diagnostic settings [6,20–25]. APP is often rated as equivalent to, or more satisfactory than physician-led care, with the opportunity to spend more time with AP physiotherapists (than with physicians) cited a possible reason [6,22]. However, methodological quality of primary studies within these reviews varies, and heterogeneity exists across patient satisfaction measures. Furthermore, the included primary studies are mostly conducted in MSK fields, use quantitative methodologies, and seldom offer explanations of why a patient was satisfied (or not) with APP. Considering patient satisfaction provides valuable insight into patient experience (a component of healthcare quality), and no comprehensive systematic review synthesising patient satisfaction across settings exists, further investigation is needed.
Objectives
- To evaluate patient satisfaction with APP internationally.2) To evaluate human and system attributes of patient satisfaction with APP.
Materials and Methods
Reported using Preferred Reporting Items for Systematic review and Meta-Analyses (PRISMA) [26] and the published protocol (PROSPERO: CRD42023443612) [27].
Design
Systematic mixed studies review (SMSR) with parallel-results convergent design [28]. Objective-1 was addressed quantitatively, and objective-2 was addressed quantitatively and qualitatively. SMSR was selected as mixed evidence allows comprehensive understanding of complex phenomena (patient satisfaction) and because objectives were not measuring effectiveness [29].
Eligibility criteria
Eligibility criteria (Table 1) were informed by the PICOS framework [32]. Studies were grouped for synthesis according to quantitative and qualitative design.
Table 1: Eligibility criteria [27].
Information sources
MEDLINE (Ovid), Embase, CINAHL, Cochrane, Web of Science, and PEDro databases, grey literature (ProQuest), and trial registers (clinicaltrials.gov and WHO International Clinical Trials Registry Platform) were searched from inception to September 9^th^, 2025. Manual reference list searches and consultations with expert researchers also attempted to identify further studies.
Search strategy
Search strategies were developed in line with the published protocol, using patient satisfaction, physiotherapy, and advanced practice constructs. An independent specialist librarian refined the MEDLINE (Ovid) search strategy, which was further adapted to meet other database search terms (S1 File).
Study records
Data management.
Covidence, a web-based systematic review software, was used to import citations, remove duplicates, and determine eligibility during screening.
Selection process.
Eligibility criteria instruction was provided before screening to ensure consistency. Two reviewers screened titles and abstracts against eligibility criteria independently. Full texts were obtained and imported into Covidence for articles meeting eligibility criteria or deemed indeterminable. Full texts were screened against eligibility criteria by two reviewers independently. Inter-rater screening agreement was calculated using Cohens-kappa (k). The full selection process is illustrated in the PRISMA flow diagram (Fig 1).
PRISMA flow diagram.
Data collection process.
Data were collected by two reviewers independently into a Microsoft Excel form with pre-set data items. Training provided prior to data collection helped maintain quality and consistency. Data from 5 studies were first collected by both reviewers and subsequently compared to ensure consistency. Following full data collection, data were collated with discrepancies resolved through discussion. Authors of one study [33] were contacted twice to address incomplete data, but due to lack of response the study was excluded.
Data items
Data items were sought in line with the published protocol, including study characteristics, population, intervention, and outcome data.
Quality assessment
The mixed methods appraisal tool (MMAT) assessed methodological quality of included studies. The MMAT is a valid, reliable, and efficient tool [34,35] developed to appraise methodological quality of five empirical study categories (qualitative, randomised-controlled trial, non-randomised, quantitative descriptive, and mixed methods) eligible for inclusion [36]. Two reviewers familiarised themselves with the MMAT before independently completing quality assessment. A pilot of 5 studies were appraised and discussed to ensure reviewer consistency. The first two MMAT questions ensured the paper was an empirical study [36], then criteria were rated “Yes”, “No”, or “Can’t Tell” depending on information reported in the paper. An amendment to the published protocol involved using thresholds and a summary scale to present MMAT outcomes. These identified high, moderate, and low-quality studies using a percentage of “Yes” responses (0–40% = Low, 60–80% = Moderate, 100% = High). Thresholds were informed by similar research using the MMAT and were included to support narrative synthesis [37,38]. As this SMSR aimed to generate rich understanding of patient satisfaction, studies were not excluded based on methodological quality, as this could have limited insight [39]. Quality assessment was instead used to provide transparency and aid interpretation during thematic synthesis [39,40].
Synthesis methods
Parallel-results convergent synthesis design, involving separate quantitative and qualitative data syntheses, before integration in the discussion [28]. Meta-analysis or statistical exploration of heterogeneity (e.g., subgroup analysis) was not appropriate.
Quantitative synthesis
To evaluate patient satisfaction with APP internationally (objective 1) and evaluate human and system attributes of patient satisfaction with APP (objective 2), narrative synthesis was conducted [41]. This was chosen due to expected heterogeneity within primary studies and lack of randomised controlled trials (RCT). The methodological foundation of narrative synthesis includes 3 key elements completed iteratively and non-sequentially (Fig 2) [41].
Elements of narrative synthesis [42].VSQ-9: Visit Specific Satisfaction Questionnaire, MMAT: Mixed Methods Appraisal Tool, GRADE: Grading of Recommendations, Assessment, Development and Evaluation, APP: Advanced Practice Physiotherapy.
Qualitative synthesis
To evaluate human and system attributes of patient satisfaction with APP (objective 2), thematic synthesis was conducted [42]. This was chosen to integrate findings of multiple qualitative or mixed-methods studies and involved three steps (Fig 3) [42].
Steps of thematic synthesis [42].
Two reviewers completed thematic synthesis independently before coming together to discuss analytical themes. This crystallisation stage helped the development of analytical themes that offer rich accounts of patient satisfaction [43]. To increase trustworthiness, reflexivity helped position subjective and intersubjective influences when shaping of analytical themes (S2 File) [44]. Analytical themes were supported by textual descriptions and illustrative quotations in an accompanying table. As analytical themes derived from text within studies’ results sections, differentiation between author and participant quotes were made.
Certainty assessment
Grading of Recommendations, Assessment, Development and Evaluation (GRADE) assessed certainty of evidence for quantitative syntheses (S3 File) [45]. Most syntheses started as “low” and adaptations to assessments within GRADE domains were made to account for the mostly non-randomized study (NRS) designs. Questions addressing various biases within the MMAT and the overall rating (high to low) informed assessment of the Risk of Bias domain [46]. Indirectness was assessed against how thoroughly studies reported PICOS elements, for example, information provided regarding the AP physiotherapists experience, qualifications, or specific role (intervention) [46]. Without statistical heterogeneity measures, Inconsistency was assessed using descriptive statistics across outcomes within a given measure (e.g., mean averages across VSQ-9 scores). Imprecision was informed by CIs or SE when reported [46]. Total NRS and unpublished papers informed publication bias assessment [46]. Without effectiveness data, rating-up was not appropriate for magnitude of effect or dose-response gradient. All plausible confounding was assessed using study population characteristics considered to introduce confounding (e.g., younger age) [15,47].
GRADE Confidence in Evidence from Reviews of Qualitative Research (GRADE-CERQual) assessed confidence in evidence for qualitative syntheses (S4 File) [48]. Methodological limitations were assessed using the MMAT [49], coherence was assessed considering fit between collected primary study data and review findings [50], adequacy was assessed through data richness and bridging criteria “thoroughness of data collection and interpretation” [51,52], and relevance was assessed by how clearly primary studies reported alignment with eligibility criteria [53]. GRADE-CERQual assessments were presented using a summary of qualitative findings table [54]. Both GRADE and GRADE-CERQual assessments were completed independently by two reviewers, with conflicts resolved through discussion, not requiring a third reviewer.
Results
Study selection
Searches yielded 3599 studies. After duplicate removal, 1955 studies underwent title and abstract screening, and 115 studies underwent full-text screening, resulting in 35 studies included (Fig 1) [55–89]. A list of excluded studies from full-text screening is provided (S5 File). Very high reviewer agreement occurred at title and abstract (k = 0. 9) and full-text (k = 0.96) screening. Disagreements were resolved through discussion and did not require third author arbitration.
Study characteristics
Studies were published between 1999–2025, encompassing RCT (n = 5), quantitative non-randomized (n = 11), quantitative descriptive (n = 3), qualitative (n = 9), and mixed methods (n = 7) designs. Studies originated from Canada (n = 14), Australia (n = 9), United Kingdom (n = 7), Sweden (n = 2), Denmark (n = 1), Republic of Ireland (n = 1), and France (n = 1). All but one study was published [83], and no companion studies were identified. Studies were in MSK/orthopaedic fields, spanning hospital outpatient department (n = 19), emergency department (n = 8), primary care (n = 6), and physiotherapy department (n = 2) settings. Study characteristics are detailed in Table 2.
Table 2: Results of individual studies.
Quality assessment
Studies were rated as high (n = 8), moderate (n = 15), and low (n = 11) quality (S6 File). Qualitative studies demonstrated highest, and quantitative descriptive studies lowest methodological quality. Quality criteria met the least were assessor blinding to intervention (RCT) and confounders accounted for in design and analysis (quantitative non-randomized).
Results of individual studies
Key results of individual studies are presented in Table 2 and expanded results of individual studies are available in S7 File.
Results of syntheses
Narrative synthesis: Overall patient satisfaction.
Across twenty-three studies capturing quantitative data, overall patient satisfaction with APP was consistently high, regardless of instrument, study quality, or analytic approach [55,56,58–60,64–66,68–71,73–77,80,81,83,86–88].
Ten moderate (n = 8) and low (n = 2) quality studies using a modified visit specific satisfaction instrument (VSQ-9, 0 “poor” to 100 “excellent”) showed excellent mean (84.5–94) and/or median (90.6–100) satisfaction [55,60,70,74–77,81,87,88], although the certainty of this finding was rated as very low using GRADE.Three moderate (n = 2) and low (n = 1) quality studies using the patient satisfaction questionnaire (PSQ, 5-point Likert scale, strongly agree – strongly disagree) showed 45–85% “strongly agree” with “overall I was satisfied with the treatment received” [58,64,71], although the certainty of this finding was rated as very low using GRADE.Three studies of high, moderate, and low quality using the MedRisk patient satisfaction instrument (1 “Strongly Disagree” – 5 “Strongly Agree”), showed high mean overall satisfaction (3.9–4.8) [68,87,88], although the certainty of this finding was rated as very low using GRADE.Three moderate (n = 1) and low (n = 2) quality studies using bespoke 5-point Likert scale questionnaires of varied wording, showed high collated positive responses (i.e., both agree and strongly agree) for overall satisfaction (90%−98%) [65,83,86], although the certainty of this finding was rated as very low using GRADE.
Six individual high (n = 1), moderate (n = 2), and low (n = 3) quality studies all showed high overall satisfaction using different outcome measures or analyses (Table 2) [56,59,66,69,73,80].
Narrative synthesis: Human attributes of patient satisfaction (HAPS).
Across seventeen studies capturing quantitative data, HAPS with APP were consistently high, regardless of instrument, study quality, or analytic approach [55,58,60–62,64–66,68–71,75,76,80,83,88].
Five moderate (n = 4) and low (n = 1) quality studies using a modified VSQ-9 instrument (“poor” to 100 “excellent”) and measuring five HAPS, showed excellent (mean, median) satisfaction for explanation during consultation (87–93, 100), technical skills (91–95, 100), personal manner (94–96, 100), answers to questions (92–93, 100), and advice and information about exercise or activity (88–93, 100) [55,60,70,75,76]. The certainty of this finding was rated as very low using GRADE.Two moderate quality studies using the Quality from the Patients Perspective questionnaire (QPP, 4-point scale, do not agree at all – completely agree), showed complete agreement to “I received the best possible examination and treatment” and “[the caregiver] seemed to understand how I experienced my situation” [62,66]. The certainty of this finding was rated as very low using GRADE.Three moderate (n = 2) and low (n = 1) quality studies using the PSQ (5-point Likert scale, strongly agree – strongly disagree) and measuring four HAPS, showed 39–83% “strongly agreed” with “I felt I received good advice and information about my condition”, 42–86% “strongly agreed” with “I was given enough time to ask questions and discuss my condition”, 43–87% “strongly agreed” with “I felt confident the member of staff could deal with my condition”, and 42–77% “strongly agreed” with “I felt confident the member of staff would have got a second opinion if necessary” [58,64,71]. The certainty of this finding was rated as very low using GRADE.Two studies of moderate and low quality used bespoke 5-point Likert scale questionnaires of varied wording to measure five HAPS, reported as collated positive responses (i.e., both agree and strongly agree) [65,83]. Positive responses were high for thoroughness of examination (97%, 95%), listening and understanding (91%, 80%), interest in the patient as a person (80%, 85%), advice received (90%), and amount of information provided about medicines (86%). The certainty of this finding was rated as very low using GRADE.
Five individual studies of high (n = 1), moderate (n = 1), and low (n = 3) quality all reported high scores relating to HAPS using different outcome measures or analyses (Table 2) [61,68,69,80,88].
Narrative synthesis: System attributes of patient satisfaction (SAPS).
Across twelve studies capturing quantitative data, SAPS with APP were mostly high, regardless of instrument, study quality or analytic approach [55,60,61,65,68–70,75,76,80,83,88].
Five moderate (n = 4) and low (n = 1) quality studies using a modified VSQ-9 instrument (0 “poor” to 100 “excellent”) and measuring five SAPS, showed good to excellent (mean, median) satisfaction for waiting time for appointment (55, 50), clinic location (N/A, 50), clinic telephone contact (70–81, 75), wait time in clinic (70–81, 75), and time spent in appointment (88–93, 75–100) [55,60,70,75,76]. The certainty of this finding was rated as very low using GRADE.Two studies of moderate and low quality used bespoke 5-point Likert scale questionnaires with varied wording to measure five SAPS^,^ reported as collated positive responses (i.e., both agree and strongly agree) [65,83]. Positive responses were moderate for “it was easy to make an appointment with the physiotherapist”(57%), “there was an acceptable time lapse to obtain an appointment” (48%), “it was possible to obtain an appointment on a convenient day or hour” (65%), and “the waiting time was acceptable” (73%). Furthermore, “time spent with the physiotherapist was too short” presented as 74% “disagree and strongly disagree” in one study, and 35% “agree and strongly agree” in the other. The certainty of this finding was rated as very low using GRADE.
Five individual studies of high (n = 1), moderate (n = 1), and low (n = 3) quality all reported high scores relating to HAPS using different outcome measures or analyses (Table 2) [61,68,69,80,88].
Thematic synthesis
Fourteen studies of high (n = 6), moderate (n = 4), and low (n = 4) quality captured qualitative data pertaining to patient satisfaction with APP [55,57,63,67,68,72,78–80,82–85,89]. Twelve studies captured HAPS [55,57,63,67,68,72,78,82–85,89], and all studies captured SAPS. Supporting quotes presented in Table 3.
Table 3: Supporting quotes for qualitative themes.
Thematic synthesis: Human attributes of patient satisfaction (HAPS)
Four analytical themes emerged pertaining to HAPS: proficient communication and interpersonal skills, credible and competent experts, patient empowerment and self-management, and thorough assessments.
Proficient communication and interpersonal skills [55,63,67,68,72,78,82–85,89]: Patients appreciate how AP physiotherapists proficiently use active listening, and clear, simple, effective communication during consultations. Patients are satisfied with education provided by AP physiotherapists and being kept informed of key progress updates relevant to their care. Patients value AP physiotherapists’ interpersonal and relational skills, their approachability, empathy, and ability to create an environment that fosters therapeutic alliance. High confidence evidence for proficient communication and interpersonal skills (GRADE-CERQual).
Credible and competent experts [55,63,67,68,72,78,82–85,89]: Patients recognise AP physiotherapists as credible, knowledgeable experts. This results in confidence and trust in their professional ability and competence, with APP being seen as equivalent, or preferable to doctor-led care in some settings. High confidence evidence for credible and competent experts (GRADE-CERQual).
Patient empowerment and self-management [55,63,68,72,82–85]: Patients appreciate AP physiotherapists’ use of shared decision making and being empowered to steer their own recovery. Reassurance and encouragement provided by AP physiotherapists gives patients confidence to self-manage their condition, providing a sense of control. Conversely, some patients felt overwhelmed when too involved in decision-making regarding their care, perhaps preferring a more autocratic style. High confidence evidence for patient empowerment and self-management (GRADE-CERQual).
Thorough assessments [57,63,67,72,83–85,89]: Patients feel AP physiotherapists conduct thorough assessments, valuing the opportunity to spend time and ask questions regarding their care. Time taken to conduct thorough assessments also perhaps contributes to patients experiencing person-centred care. Moderate confidence evidence for thorough assessments (GRADE-CERQual).
Thematic synthesis: System attributes of patient satisfaction
Three analytical themes emerged from synthesis of qualitative data pertaining to SAPS: fast access to specialist care, convenient location and amenities, and integrated care.
Fast access to specialist care [55,57,63,67,68,72,78–80,82–85,89]: Patients perceive APP to speed up access to specialist care. Patients perceive this as reducing time to diagnosis and receiving the right treatment for their condition promptly. Furthermore, patients appreciate shorter than expected wait times, seeing APP as an accessible, effective and efficient service. Moderate confidence evidence for fast access to specialist care (GRADE-CERQual).
Convenient location and amenities [55,63,67,68,80,82,83,89]: The location of APP services is important to patients, with mixed preference between hospital, urban, community, or rural settings. A key factor driving satisfaction with location appears to be travel distance or time, with stronger preference for convenient services closer to patients’ homes. The amenities (or lack of) and physical environment of APP services is also important to patients (e.g., parking facilities, waiting room comfort). Moderate confidence evidence for convenient location and amenities (GRADE-CERQual).
Integrated care [55,63,68,72,78,80,82–84,89]: APP is positively received when effectively integrated into the wider care pathway. This integration, for example through co-located clinics in community or hospital settings, is seen to facilitate communication between AP physiotherapists and doctors. Conversely, patients are dissatisfied when integration does not exist and get frustrated with long wait-times for referrals into other services (e.g., imaging) following APP. Moderate confidence evidence for integrated care (GRADE-CERQual).
Discussion
This SMSR found patient satisfaction with APP internationally is high, based on quantitative data assessed using GRADE, which indicated very-low certainty evidence. Quantitative synthesis showed HAPS were also high (very-low certainty evidence, GRADE), supported by qualitative themes indicating AP physiotherapists use proficient communication and interpersonal skills, are credible and competent experts, drive patient empowerment and self-management, and conduct thorough assessments (moderate to high confidence evidence, GRADE-CERQual). Quantitative synthesis showed SAPS were mostly high (very-low certainty evidence, GRADE), supported by qualitative themes suggesting APP enables fast access to specialist care, with convenient locations and amenities, and through integrated care (moderate confidence evidence, GRADE-CERQual).
Convergence between syntheses
Convergence was observed when quantitative and qualitative syntheses substantiated one another, offering triangulation and strengthening the conviction of findings. HAPS showed strong convergence between syntheses, especially the theme “proficient communication and interpersonal skills” strongly represented quantitatively with high scores in personal manner, explanation during consultations, and listening attributes. This finding is likely crucial to unlocking many other drivers of patient satisfaction with APP. Communication that purposefully involves the patient, demonstrates active listening, is patient-centred, and uses verbal and nonverbal techniques is known to build therapeutic alliance and drive engagement in physiotherapy encounters [91]. The AP physiotherapist’s ability to employ a broad range of these advanced communication skills, modified to account for individual patient needs or preferences, and to communicate complex information in simple terms, undoubtedly contributes to driving patient satisfaction. The theme “credible and competent experts” was reflected in high scores for technical skills and patients’ confidence in AP physiotherapists’ ability, and the theme “thorough assessments” in high scores for thoroughness of examination and patients feeling they had time to ask questions. Both these findings relate to the concept of trust between patients and AP physiotherapists. Trust is fundamental to effective relationships between healthcare providers and patients, facilitating positive interactions, rapport, and can have direct therapeutic effects, all of which are important for driving satisfaction [92]. Convergence in SAPS also occurred, but to a slightly lesser extent. The theme “fast access to specialist care” was reflected in high scores for acceptable time to obtaining an appointment, and waiting time in clinic, and the theme “convenient location and amenities” in high scores for clinic location, and ease of making an appointment at convenient times. These findings centre around the dimensions of healthcare accessibility, availability, and acceptability, all of which are intimately connected to patient satisfaction [93]. When healthcare services provide the right care, to address individualised needs, at the right time, patient expectations are met or surpassed, and satisfaction is likely to occur. The ability of APP to integrate at various stages of the care pathway, especially in primary care, triage, or diagnostic roles, evidently improves timely access and drives satisfaction with services. Two qualitative themes not reflected in the quantitative data were “patient empowerment and self-management” and “integrated care”. This is likely because patient satisfaction measures in the primary studies did not evaluate these concepts, either due to limitations in the measurement tools or perhaps because these phenomena are better explored qualitatively.
High convergence across quantitative and qualitative syntheses suggests both HAPS and SAPS influence overall satisfaction with APP. However, HAPS were more apparent in this review. More qualitative themes emerged, more studies captured quantitative data, and more syntheses occurred, resulting in higher overall convergence. The prominence of HAPS suggests AP physiotherapists themselves are integral to driving patient satisfaction.
Context
Our findings align with World Physiotherapy’s definition of APP as a “level of practice, functions, responsibilities, activities and capabilities” [8], as these features closely mirror HAPS. It is AP physiotherapists’ communication proficiency, expertise, or thoroughness that drives satisfaction, reflecting an advanced level of practice rather than skills associated with further scope of practice (e.g., injection therapy). Congruence between this APP definition and what drives satisfaction with APP from the patient’s perspective, strengthens the credibility of this definition.
High patient satisfaction with AP also exists across other professions [94–96]. High patient satisfaction occurs in cancer, emergency, and critical-care advanced nursing practice (ANP), often with equivalent or greater satisfaction from nurse-led, compared to physician-led care [97,98]. Although not a focus area for our review, equivalence and preference to physician-led care emerged from thematic synthesis (credible and competent experts), strengthening the case for alternative care models. Likewise, high patient satisfaction exists in ANP-led memory assessment clinics, driven by the nurse’s sensitivity, empathy, and knowledge [99], as found with APP in our review (proficient communication and interpersonal skills, credible and competent experts). These attributes help form therapeutic alliance from assessment, through to multimodal care, a journey AP physiotherapists are well equipped to own. In advanced practice radiography (APR), patient satisfaction is high in therapeutic settings, driven by comprehensive consultations, patient empowerment, time available, opportunities for questions, being well informed, and treatment efficacy [100,101]. These HAPS with APR are congruent with our findings, showing AP physiotherapists deliver patient-centred and personalised care.
Our review supports the conceptual distinction between HAPS and SAPS as proposed by Ng and Luk (2019) [15]. For example, provider attitude was reflected as a human attribute in our review through the AP physiotherapists’ personal manner, interest in the patient as a person, and interpersonal skills. However, some attributes were less clearly delineated. Efficacy was considered a human attribute if patients felt confident APP could manage their condition (i.e., future-tense), as satisfaction depended on perceptions of AP physiotherapists’ competence and capability. Conversely, if patients felt APP did improve their problem (i.e., past-tense), perhaps by reducing time to diagnosis and receiving treatment, this was a system attribute. Although not an attribute, another concept less delineated was time. If patients felt AP physiotherapists took time to listen and conduct thorough assessments (regardless of appointment duration), it was a human attribute. Whereas if patients were satisfied with the appointment duration, it was a system attribute. The blurred boundaries identified in our review support the notion that HAPS and SAPS are dynamic and contextual in nature and should be interpreted accordingly [15]. Findings from this SMSR also reinforce Donabedian’s model of healthcare quality, illustrating relationships between healthcare structure (SAPS), process (HAPS), and outcome (Patient Satisfaction) [102,103]. In this theoretical framework, Structure relates to the physical and organisational aspects of healthcare, encompassing rational performance, accessibility, culture, and perceived efficacy of services. Process relates to methods and procedures of care delivery, encompassing interactions with healthcare providers, their attitudes or technical competence, and emotions evoked from healthcare services. Outcome relates to the effects of healthcare on patients, which in this instance is patient satisfaction.
Limitations
This SMSR was limited by the modest methodological quality of the included quantitative studies and by the application of GRADE to predominantly non‑randomised designs, which is a recognised challenge [104]. Additionally, GRADE assessments were informed by MMAT outcomes, which penalise lack of blinding, even though blinding in physiotherapy research is often difficult or impossible [105]. GRADE also rates non-randomised designs down, even though observational research may provide highly relevant, real‑world evidence for outcomes such as patient satisfaction. Together, these factors may have contributed to the conservative “very low” certainty ratings across quantitative syntheses, despite the consistency of findings across the primary studies.
All included studies were mostly in diagnostic MSK or orthopaedic settings. AP standards state advanced practitioners should provide interventions like therapy, lifestyle advice, and care [105], and patient satisfaction with these aspects of APP is not reflected in this review. Furthermore, clinical encounters in MSK and orthopaedics are typically outpatient-based and as attributes of patient satisfaction will be relevant to this context, caution is encouraged when considering applicability to inpatient-based APP.
Lastly, although not a methodological limitation, studies originated from all but one World Physiotherapy region (South America) with recognised APP roles [2]. While our findings are largely representative of APP internationally, caution is encouraged when considering generalisability to South America. This under-representation may be due to only Peru having recognised APP roles demonstrated in the literature to date, the emerging nature of physiotherapy across the region, and/or Brazil producing most South American physiotherapy research [106].
Clinical implications
The human or relational aspect of an APP patient encounter matters to patients. Strong communication skills like active listening, clear explanations, and providing advice all appear to be important to patient satisfaction. AP physiotherapists should be supported to develop these interpersonal and relational skills alongside their development of technical skills and expertise. Patient empowerment also appears to be integral to patient satisfaction with APP. Therefore, to drive patient satisfaction with APP, services should adopt principles of personalised care like shared decision-making, supported self-management, and social prescribing. Lastly, integrating APP services within the wider healthcare system is essential to drive satisfaction. Therefore, when implementing or improving APP services, careful consideration to how APP seamlessly integrates with its co-dependent services should be a priority.
Research implications
High methodological quality studies using prospective or randomised designs, and with consideration of confounding variables, are needed to improve evidence certainty. Future research should investigate relationships between HAPS and SAPS and explore if compensatory mechanisms exist, as suggested in service quality settings outside healthcare [16,107]. A comprehensive review of APP patient preferences, values, and expectations is also needed, as already explored across other levels of physiotherapy practice [108–110]. Patient satisfaction is closely connected to these concepts, and understanding what matters to APP patients (across the care pathway) could improve patient centredness. Lastly, deeper exploration into patient experience of APP (as a key component of healthcare quality) and how patient satisfaction is situated within it, is needed. Future research exploring these constructs could provide valuable insights into patient-centred care and inform future APP service quality improvement. Central to all future research in this field is the need for a standardized, valid, and reliable tool that is specifically designed to measure patient satisfaction with APP. This would allow more precise measurement of patient satisfaction and benchmarking of APP services across healthcare sectors and settings.
Conclusion
Overall patient satisfaction with APP internationally is high, driven by both HAPS and SAPS. Despite the very-low certainty of this evidence, there is moderate to high confidence that AP physiotherapists drive high patient satisfaction as proficient communicators and credible experts, who conduct thorough assessments and drive patient empowerment. There is also moderate confidence in high patient satisfaction being achieved through APP services enabling fast access to specialist care, at convenient locations, whilst situated within integrated care systems.
Key Points
Findings.
Overall patient satisfaction with APP internationally is high, driven by human and system attributes.
Implications.
AP physiotherapists are key to patient satisfaction. Ensuring AP physiotherapists are supported to develop interpersonal and communication skills, alongside technical skills, is essential to drive patient satisfaction.
Caution.
Methodological quality of quantitative studies was low, no relevant studies from South America were identified, and findings relate to MSK and Orthopaedic settings only.
Supporting information
S1 FileSearch strategies.(DOCX)
S2 FileReflexivity statements.(DOCX)
S3 FileGRADE Summary of Findings (SoF) table.(DOCX)
S4 FileGRADE CERQual evidence profile.(DOCX)
S5 FileList of excluded studies.(DOCX)
S6 FileQuality assessment.(DOCX)
S7 FileExpanded individual studies table.(DOCX)
S1 ChecklistPRISMA 2020 checklist.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1NHS. Multi-professional framework for advanced clinical practice in England. 2017. http://www.aomrc.org.uk/wp-content/
- 2Tawiah AK, Desmeules F, Finucane L, Lewis J, Wieler M, Stokes E, et al. Advanced practice in physiotherapy: a global survey. Physiotherapy. 2021;113:168–76. doi: 10.1016/j.physio.2021.01.001 34794584 · doi ↗ · pubmed ↗
- 3James JJ, Stuart RB. Expanded role for the physical therapist. Screening musculoskeletal disorders. Phys Ther. 1975;55(2):121–31. doi: 10.1093/ptj/55.2.121 124877 · doi ↗ · pubmed ↗
- 4Vedanayagam M, Buzak M, Reid D, Saywell N. Advanced practice physiotherapists are effective in the management of musculoskeletal disorders: a systematic review of systematic reviews. Physiotherapy. 2021;113:116–30. doi: 10.1016/j.physio.2021.08.005 34607076 · doi ↗ · pubmed ↗
- 5Lafrance S, Vincent R, Demont A, Charron M, Desmeules F. Advanced practice physiotherapists can diagnose and triage patients with musculoskeletal disorders while providing effective care: a systematic review. J Physiother. 2023;69(4):220–31. doi: 10.1016/j.jphys.2023.08.005 37714771 · doi ↗ · pubmed ↗
- 6Lafrance S, Lapalme J-G, Méquignon M, Santaguida C, Fernandes J, Desmeules F. Advanced practice physiotherapy for adults with spinal pain: a systematic review with meta-analysis. Eur Spine J. 2021;30(4):990–1003. doi: 10.1007/s 00586-020-06648-5 33123757 · doi ↗ · pubmed ↗
- 7Maddigan K, Davis C, Saville B, Nishimura K, Van Bussel J, Tawiah AK, et al. The educational pathway to Advanced Practice for the physiotherapist: A systematic mixed studies review. P Lo S One. 2025;20(5):e 0322626. doi: 10.1371/journal.pone.0322626 40354470 PMC 12068731 · doi ↗ · pubmed ↗
- 8World P. World Physiotherapy. https://world.physio/about-us. 2023.