Infectious disease diagnosis by artificial intelligence (AI): Differences in patient backgrounds and symptoms between antigen test positives and novel AI-powered pharyngeal endoscopy test positives
Masahiko Mori, Shinji Yoshinaga, Tadayoshi Moriyama, Takafumi Maekawa

TL;DR
This study compares patients who tested positive for infectious diseases using a traditional antigen test versus a new AI-powered endoscopy system, finding differences in symptoms and testing timing.
Contribution
The study introduces a novel AI-powered endoscopy system for infectious disease diagnosis and highlights its distinct clinical implications compared to conventional antigen testing.
Findings
AI-positive cases tested earlier after symptom onset compared to antigen-positive cases.
AI-positive cases were more frequently pediatric and showed higher rates of cough and fever.
The AI system misdiagnosed 23% of COVID-19 cases as influenza due to overlapping symptoms and pharyngeal features.
Abstract
This study aimed to identify differences in patient background and symptoms between individuals who tested positive using conventional rapid antigen (Ag) tests and those who tested positive using a novel artificial intelligence (AI)–powered pharyngeal endoscopy system. A total of 813 patients underwent both influenza/COVID-19 Ag testing and AI-powered endoscopic testing. We analyzed differences in patient characteristics and symptoms between the two test-positive groups. AI testing showed an overall percent agreement of 62% (95% confidence interval [CI] 58–66%) (442/713), a positive percent agreement of 47% (95% CI 40–53%) (125/269), and a negative percent agreement of 71% (95% CI 67–76%) (317/444) compared with Ag testing. Compared with Ag-positive cases, AI-positive cases exhibited a shorter interval from symptom onset to testing; median 18 hours (Interquartile range [IQR] 10–27) for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
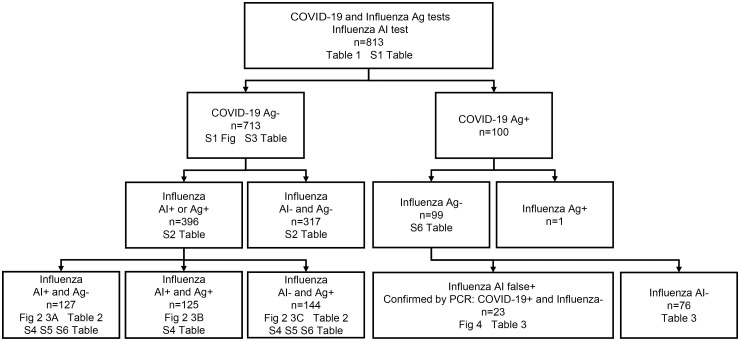 Fig 1
Fig 1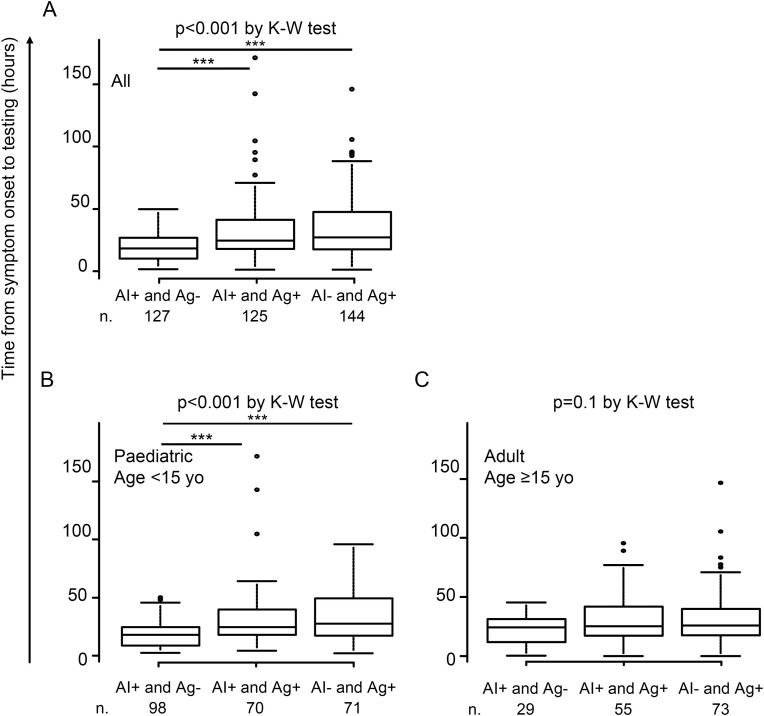 Fig 2
Fig 2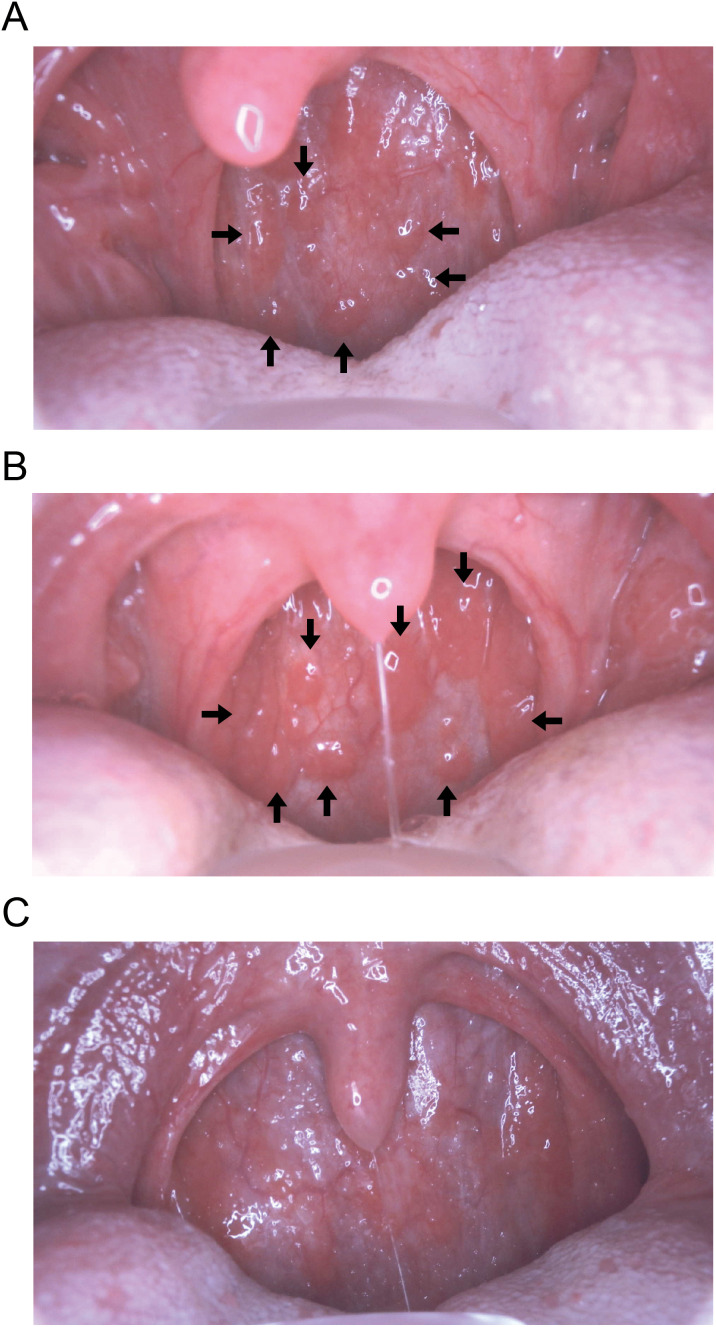 Fig 3
Fig 3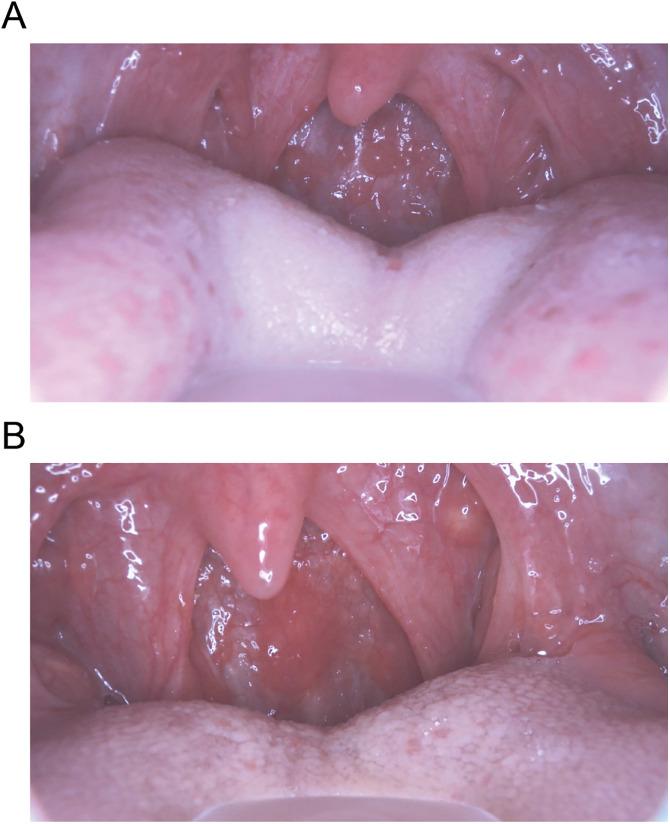 Fig 4
Fig 4- —Health Science Center, general foundation, Sagamihara, Kanagawa, Japan
- —Sasebo city medical association, Sasebo, Nagasaki, Japan
- —Nagasaki prefecture medical association, Nagasaki, Japan
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Bleeding Diagnosis and Treatment · Colorectal Cancer Screening and Detection · COVID-19 diagnosis using AI
Introduction
During the COVID-19 pandemic from 2020 to early 2023, the number of seasonal influenza virus infections worldwide dramatically decreased but surged again after the pandemic subsided (WHO FluNet. https://www.who.int/tools/flunet). Similarly, in Japan, an influenza epidemic re-emerged after national COVID-19 prevention policies were lifted in May 2023 [1]. Influenza and COVID-19 share similar respiratory and systemic symptoms, making it difficult for clinicians to distinguish between the two pathogens based on clinical presentation alone, particularly since the emergence of the Omicron variant, which has been associated with smaller differences in disease severity between the two infections [2].
Throughout the COVID-19 pandemic, rapid antigen (Ag) testing using nasopharyngeal swab samples for viral infections, including COVID-19 and influenza, became widely recognized as a point-of-care diagnostic method in hospitals and drive-through testing centres [3]. However, concerns persisted regarding the discomfort caused by swab collection and the risk of viral exposure to healthcare workers, particularly when obtaining samples from paediatric patients [4].
As an alternative diagnostic method for influenza virus infection, an artificial intelligence (AI)-powered pharyngeal endoscopy system was introduced in Japan in December 2022 [5]. This system analyzes pharyngeal images captured by an endoscopic scope, enabling AI to detect follicular nodules on the posterior pharyngeal wall—findings commonly observed in patients with influenza virus infection [6]. By integrating clinical information such as patient backgrounds and symptoms, the AI system provides an automated diagnosis of influenza virus infection [5]. However, differences in diagnostic outcomes between this AI-powered pharyngeal endoscopy system and conventional rapid Ag testing—and the potential role of AI-based diagnosis in point-of-care testing in outpatient settings—remain unclear.
The primary objective of this study was to identify differences in patient backgrounds and symptoms between individuals who tested positive for influenza by conventional rapid Ag testing and those who tested positive using the AI system. A secondary objective was to explore challenges in developing AI-based diagnostic models for infectious diseases by examining cases misclassified by the AI system, with a particular focus on COVID-19 cases incorrectly diagnosed as influenza.
Results
Characteristics of subjects
The characteristics of sex, age, and influenza testing positivity among 813 subjects are presented in Table 1 and S1 Table (original dataset). In total, 52% (420/813) of patients were diagnosed with influenza virus infection as positive by either AI or Ag. Among these, 276 were positive by AI, and 270 by Ag. Of the 270 Ag-positive cases, 50% (134/270) were infected with influenza A strain and 50% (136/270) with influenza B strain. In addition, 12% (100/813) of patients were diagnosed with COVID-19 infection.
Table 1: Characteristics of study subjects.
Among the 713 COVID-19-negative cases (shown on the left side of the participant flow diagram in Fig 1), the 396 influenza testing-positive patients were younger (median 13 (interquartile range [IQR] 10–27) years vs.15 (IQR 11–34) years, p = 0.003), had a higher frequency of contact history with infected individuals (48% (189/396) vs. 24% (75/317), odds ratio [OR] 2.9 (95% confidence interval [CI] 2.1-4.1), p < 0.001) and more frequent use of antipyretics (45% (178/396) vs. 37% (118/317), OR 1.4 (95% CI 1.02-1.9), p = 0.04). They had a lower frequency of influenza vaccination (22% (89/396) vs. 31% (98/317), OR 0.6 (95% CI 0.5-0.9), p = 0.01). Symptomatically, they showed higher frequencies of cough (81% (322/396) vs. 40% (157/317), OR 4.4 (95% CI 3.2-6.2), p < 0.001), runny nose (64% (254/396) vs. 42% (134/317), OR 2.4 (95% CI 1.8-3.3), p < 0.001), fever (≥38.0°C) (65% (259/396) vs. 31% (98/317), OR 4.2 (95% CI 3.1-5.8), p < 0.001), joint pain (24% (95/396) vs. 17% (55/317), OR 1.5 (95% CI 1.04-2.2), p = 0.03) and muscle pain (17% (69/396) vs. 12% (39/317), OR 1.7 (95% CI 1.07-2.5), p = 0.03), but a lower frequency of gastrointestinal symptoms (7% (26/396) vs. 11% (35/317), OR 0.6 (95% CI 0.3-0.9), p = 0.04) compared with the 317 influenza testing-negative patients (S2 Table).
Participant flow diagram.The numbers of figures and tables whose analyses were performed are indicated.
Diagnosis concordance between Ag and AI testing
The concordance rate for diagnosing influenza between Ag and AI testing was evaluated. Among the 713 COVID-19 Ag-negative cases, AI testing showed an overall percent agreement of 62% (95% CI 58–66%) (442/713), a positive percent agreement of 47% (95% CI 40–53%) (125/269), and a negative percent agreement of 71% (95% CI 67–76%) (317/444) with Ag testing (S3 Table). The area under the receiver operating characteristic curve (AUROC) for AI testing, using Ag testing as the reference, was 0.59 (95% CI, 0.55–0.63), with a specificity of 0.71 and a sensitivity of 0.47 (S1 Fig). In analyses stratified by age and time from symptom onset, a higher frequency of disagreement between AI and Ag testing was observed among paediatric patients (<15 years) than among young and middle-aged adults (15–64 years): 43% (169/397) vs. 32% (91/284), OR 1.6 (95% CI 1.1-2.2), p = 0.006. Specifically, compared with adult patients, paediatric patients showed a higher frequency of negative disagreement (AI+ and Ag-) results relative to negative agreement (AI- and Ag-) results: 38% (98/256) vs. 17% (28/168), OR 3.1 (95% CI 1.9-5.0), p < 0.001. A similar trend was observed when comparing paediatric patients with elderly adults (≥65 years): 38% (98/256) vs. 0.5% (1/20), OR 12 (95% CI 1.6-89), p = 0.002. Among the 269 Ag-positive cases (although 270 were originally reported in Table 1, one patient with dual infection—COVID-19 Ag+ and influenza B Ag + —was excluded from the analyses; this patient is listed as COVID-19 Ag+ and Influenza Ag + , n = 1 in Fig 1), no significant difference in AI concordance was observed between strain A (49% (66/134)) and strain B (44% (59/135), OR 1.3 (95% CI 0.8-2.0), p = 0.4). These findings indicate that paediatric patients exhibited a higher frequency of discordant results between AI and Ag testing, characterized by a greater proportion of AI+ and Ag- results compared with adult patients.
Influenza vaccination and testing positivity
We next analyzed whether influenza vaccination prior to testing affected differences in test positivity between AI and Ag testing. There was no significant difference in vaccination rates between AI+ and Ag+ cases: 21% (53/252) in AI+ patients vs. 23% (62/269) in Ag+ patients (OR 0.9 (95% CI 0.6-1.4), p = 0.6). Similarly, vaccination rates did not differ between AI+ and Ag- patients and AI- and Ag+ patients: 21% (27/127) vs. 25% (36/144), respectively (OR 0.8 (95% CI 0.5-1.4), p = 0.5) (S4 Table). These findings suggest that a history of influenza vaccination prior to testing did not influence differences in test positivity between the two methods.
Impact of examination timing on influenza test positivity: Differences in time from symptom onset to testing among influenza testing-positive cases
We analyzed differences in the time from symptom onset to testing among influenza-testing positive cases. Among the 396 COVID-19 Ag-negative and influenza-testing positive patients, significant differences in testing time were observed among AI+ and Ag- patients (n = 127, median 18 hours (IQR 10–27)), AI+ and Ag+ patients (n = 125, median 24 hours (IQR 18–41)), and AI- and Ag+ patients (n = 144, median 27 hours (IQR 17–47)) (p < 0.001 by Kruskal-Wallis test; p < 0.001 between AI+ and Ag- patients vs. AI+ and Ag+ patients, and between AI+ and Ag- patients vs. AI- and Ag+ patients by Steel-Dwass test) (Fig 2A). This difference remained significant among paediatric patients (<15 years old) (Fig 2B) but not among adults (age ≥ 15 years old) (Fig 2C). Representative pharyngeal images for each AI and Ag test result pair are shown in Fig 3: the presence of Ikura (follicular) nodules on the posterior pharyngeal wall in AI+ and Ag- cases (Fig 3A), fusion of nodules in AI+ and Ag+ cases (Fig 3B), and disappearance of nodules in AI- and Ag+ cases (Fig 3C). These findings suggest that AI-powered diagnostic systems may have an advantage in earlier detection after symptom onset compared with Ag testing, particularly among paediatric patients.
Difference in time from symptom onset to testing among influenza testing positives.Differences in time from symptom onset to testing among AI+ and Ag- patients, AI+ and Ag+ patients, and AI- and Ag+ patients, (A) in all, (B) paediatric, and (C) adult patients are shown. Kruskal-Wallis (K-W) test was conducted with post-hoc analysis using the Steel-Dwass test (**; p < 0.001).*
Posterior pharyngeal wall images in influenza infection.Representative pharyngeal images for each AI and Ag test result pair are shown. (A) The presence of Ikura (follicular) nodules (arrows) on the posterior pharyngeal wall is observed in AI+ and Ag- cases, (B) fusion of nodules (arrows) in AI+ and Ag+ cases, and (C) disappearance of nodules in AI- and Ag+ cases.
Patient background and symptomatic differences between AI-positive and Ag-positive cases
We next analyzed differences in patient backgrounds and symptoms between those with AI+ and Ag- patients (n = 127) and those with AI- and Ag+ patients (n = 144). Compared with AI- and Ag+ patients, AI+ and Ag- patients were more frequently paediatric (OR 3.4 (95% CI 1.6-7.2), p = 0.001), tested earlier after symptom onset (<24 hours) (OR 2.6 (95% CI 1.3-4.9), p = 0.005), had a contact history with infected individuals (OR 4.6 (95% CI 2.2-9.3), p < 0.001), and more commonly presented with cough (OR 11 (95% CI 4.7-27), p < 0.001) and fever (≥38.0°C) (OR 5.6 (95% CI 2.8-11), p < 0.001). In contrast, they had a lower frequency of gastrointestinal symptoms (OR 0.2 (95% CI 0.05-0.9), p = 0.04) (Table 2). In subgroup analyses stratified by age (paediatric <15 years; adult ≥15 years) and testing time (early <24 hours; late ≥24 hours), the higher frequencies of paediatric age, early testing, contact history, and cough and fever among AI+ and Ag- patients remained significant in the paediatric and early-testing subgroups (S5 Table). However, in adults, the significance of early testing (OR 1.2 (95% CI 0.4–3.9), p = 0.8), contact history (OR 2.1 (95% CI 0.6-7.5), p = 0.3), and cough (OR 5.0 (95% CI 0.9-28), p = 0.07) was no longer observed. In the late-testing subgroup, the higher frequency of paediatric cases also became non-significant (OR 2.9 (95% CI 0.9–9.3), p = 0.07). Conversely, AI+ and Ag- patients exhibited lower frequencies of gastrointestinal symptoms in the paediatric subgroup (OR 0.03 (95% CI 0.001-0.5), p = 0.02) and lower frequencies of runny nose in the early-testing subgroup (OR 0.2 (95% CI 0.07-0.6), p = 0.006). These findings suggest that the AI system was more likely to yield positive influenza diagnoses in younger patients or those tested earlier after symptom onset—particularly among individuals with a contact history, cough, or fever—compared with Ag testing.
Table 2: Differences in patient background and symptom frequencies between influenza AI positives (AI+ and Ag-) and Ag positives (AI- and Ag+). Results from multivariable binary logistic regression analysis are shown.
Misdiagnosis by AI: False positive by AI for influenza in COVID-19 cases
We next investigated misdiagnosed cases by AI. Among the 100 COVID-19 Ag-positive cases (shown on the right side of the participant flow diagram in Fig 1), one case had dual infection (COVID-19 Ag+ and influenza Ag B+). Among the remaining 99 influenza Ag-negative cases, 77% (76/99) were negative by both influenza AI and Ag (AI- and Ag-), whereas 23% (23/99) were negative by Ag but positive by AI (AI+ and Ag-). PCR testing confirmed that all AI+ and Ag- cases were COVID-19 positive and influenza negative, indicating that these were false-positive diagnoses by the AI system. In comparisons between AI false-positive cases (n = 23) and AI-negative cases (n = 76), higher frequencies of cough (OR 28 (95% CI 2.5-327), p = 0.007) and fever (≥38.0°C) (OR 16 (95% CI 2.4-100), p = 0.004) were observed among the AI false positives (Table 3).
Table 3: Differences in patient background and symptom frequencies between influenza AI false positives and AI negatives. Results from multivariable binary logistic regression analysis are shown.
Representative pharyngeal images of COVID-19-positive patients misdiagnosed as influenza-positive by AI are shown in Fig 4. Case 1: A 9-year-old male presented 21 hours after symptom onset with a body temperature of 36.9°C, headache, cough, sore throat, general fatigue, chill, and no known contact history with infected individuals. Multiple follicular nodules were observed on the posterior pharyngeal wall (Fig 4A).
Misdiagnosis by AI.Although rapid antigen tests showed COVID-19 positive and influenza negative results, AI misdiagnosed the cases as influenza positive. (A) In Case 1, Ikura (follicular) nodules were observed on the posterior pharyngeal wall, while (B) in Case 2, round redness was noted.
Case 2: A 57-year-old male presented 17 hours after symptom onset with a body temperature of 38.8°C, headache, cough, sore throat, runny nose, general fatigue, sweating, and no known contact history with infected individuals. Round redness was observed on the posterior pharyngeal wall (Fig 4B).
These findings suggest that COVID-19 patients with prominent respiratory and systemic symptoms may exhibit pharyngeal findings similar to those of influenza virus infection, making it challenging for AI to accurately distinguish between the two viruses.
Finally, a summary of the differences in patient backgrounds and symptoms between AI-positive and Ag-positive cases is presented in Table 4. When compared with variables associated with crude influenza test positivity (AI+ or Ag+), summarized in S2 Table, younger age, cough, fever, and contact history were consistently associated with higher frequencies among AI-positive cases, as shown in Table 4. In contrast, runny nose was consistently associated with higher frequencies among Ag-positive cases. These findings highlight how patient background and symptomatic characteristics were strongly associated with test positivity for each diagnostic modality.
Table 4: Summary of differences in patient background and symptoms between AI-positive and Ag-positive cases.
Discussion
This cross-sectional study investigated the differences in patient backgrounds and symptoms between individuals who tested positive using a conventional rapid antigen (Ag) test and those who tested positive using a novel AI-powered pharyngeal endoscopy system. Compared with Ag-positive cases, AI-positive cases were more frequently paediatric patients, were tested earlier after symptom onset, were more likely to have had contact with infected individuals, and exhibited more pronounced symptoms. Additionally, this study identified several instances of AI misdiagnosis, particularly cases in which COVID-19–positive patients were incorrectly diagnosed by the AI system as having influenza virus infection.
In recent years, AI systems have been extensively developed and widely applied in the medical field, especially in image-based diagnostics. For example, AI has been incorporated into gastroendoscopy for cancer detection, assessment of invasion depth, and prediction of pathological diagnoses [7]. The novel AI-powered pharyngeal endoscopy system examined in this study diagnoses influenza virus infection by analyzing mucosal lesions—such as follicular nodules on the posterior pharyngeal wall and swelling of the lateral pharyngeal bands—in combination with clinical information [5]. Follicular nodules on the posterior pharyngeal wall, commonly referred to as “influenza follicles” or “Ikura follicles” (where ikura refers to fish caviar, derived from the Russian икра and Japanese ikura), typically appear in the early stage of infection as part of the host immune response to viral invasion, approximately eight hours after symptom onset [6]. In contrast, the sensitivity of rapid antigen testing increases over time, particularly after 24 hours from symptom onset [8,9], which is later than the appearance of follicular nodules. Consistent with this, in our study, the interval from symptom onset to testing was shorter among AI-diagnosed positive cases than among Ag-diagnosed positive cases. These findings underscore the importance of selecting diagnostic methods based on the time elapsed since symptom onset: AI testing may be more suitable for patients examined within 24 hours of symptom onset, whereas Ag testing may be more appropriate for those tested 24 hours or more after onset.
The higher frequency of paediatric patients among AI test positives compared with Ag test positives likely reflects differences in the underlying diagnostic mechanisms. Whereas Ag tests detect infection based on pathogen viral load, the AI system identifies infection through host immune responses. Age-related differences in immune function may therefore influence diagnostic outcomes. Thymic involution is a key age-related change, leading to reduced naïve T-cell production and a consequent decline in immune responsiveness to novel antigens [10,11]. This decline, known as immunosenescence, contributes to reduced vaccine efficacy and milder side effects in older adults compared with younger individuals [12–15]. The higher proportion of paediatric patients among AI test positives may thus reflect stronger immune responses to influenza virus infection in this group, resulting in more prominent mucosal lesions such as follicular nodules and more severe respiratory and systemic symptoms (e.g., cough and fever), thereby increasing the likelihood of a positive AI diagnosis. Previous studies identifying cough and fever as strong predictors of influenza infection support this interpretation [16,17]. In terms of immune responses and infection diagnosis, vaccination history was not identified as a significant factor associated with differences in test positivity between AI and Ag testing in this study. Humoral and cellular immunity acquired through vaccination may respond to viral infection at an early stage, thereby limiting both viral load and host immune responses, which could consequently reduce test positivity for both methods. Indeed, vaccination history was ranked as the least influential variable associated with test positivity in this AI model, contributing less than any respiratory or systemic symptom [5]. Furthermore, a recent study reported that high-dose influenza vaccination reduced disease severity compared with standard-dose vaccination [18]. Influenza infection following high-dose vaccination may therefore be associated with lower test positivity across both testing modalities.
Beyond age, timing of testing, and symptom profile, a history of contact with infected individuals was also more frequent among AI positives than Ag positives. This may be partly attributable to the AI model itself. In the original report on the development of this AI-powered endoscopy system, pharyngeal images were the most influential variable for diagnostic prediction, followed by body temperature, cough, and contact history [5]. Thus, the weighting of contact history as an important diagnostic feature may have contributed to its higher prevalence among AI positives in this study. Similarly, during the COVID-19 pandemic, contact history was reported as a significant predictor of test positivity in drive-through PCR testing [19]. These findings suggest that incorporating information on contact history is crucial for improving AI-based diagnostic accuracy through deep learning. In this study, the diagnostic performance of the AI model for Ag-positive cases showed an AUROC of 0.59, with a sensitivity of 47% and a specificity of 71%. These results indicate the presence of diagnostic discrepancies between the two tests. Implementing novel AI-based influenza testing that accounts for patient age, time from symptom onset, symptoms, and contact history may enhance point-of-care diagnostics in outpatient settings, particularly by complementing the moderate sensitivity (40%–80%) of conventional Ag testing [20].
Another notable finding was the occurrence of AI misdiagnoses. Pharyngitis can be caused by a range of pathogens, and the host immune response to these pathogens can result in similar follicular nodules on the posterior pharyngeal wall. Pathogens such as influenza virus, SARS-CoV-2, rhinovirus, enterovirus, and Mycoplasma pneumoniae have all been reported to cause such findings [21–24]. Moreover, COVID-19-infected patients have been observed to exhibit aggregated, millet-sized white spots surrounded by redness or ulcerative lesions on the posterior pharyngeal wall [25]. Among COVID-19 variants, the Omicron strain shows higher replication in the upper respiratory tract compared with earlier strains [26]. and has been associated with a higher frequency of sore throat than pre-Omicron variants [19,27]. During the study period, Omicron was the predominant strain; thus, the presence of follicular nodules and areas of redness in COVID-19 cases may have led to AI misdiagnosis as influenza virus infection. In the field of infectious diseases, AI has been extensively studied and applied to anti-infective drug discovery and antigen selection for vaccine development [28]. However, unlike drug discovery applications, the use of AI for infectious disease diagnostics remains challenging. Advancing AI-based diagnostic systems will require further collaboration between AI engineers and medical staff [29]. In this study, for instance, improving pathogen differentiation will likely require more advanced deep learning techniques that integrate imaging and clinical data from a variety of respiratory pathogens with similar symptoms, together with regional and seasonal epidemiological information.
Beyond diagnostic accuracy, the introduction of AI systems for point-of-care testing may help alleviate the burden associated with nasal swab collection required for Ag testing, thereby reducing both patient discomfort (e.g., nasal pain) and healthcare worker exposure risk [30]. Furthermore, diversifying point-of-care diagnostic tools beyond Ag kits would enhance preparedness for future pandemics by mitigating the risk of supply shortages of medical materials—such as Ag test kits—a challenge that was experienced globally during the COVID-19 pandemic [31].
This study has several limitations. First, influenza infection was not confirmed by PCR testing, introducing a potential risk of false-positive or false-negative results in both Ag and AI testing. Indeed, the reported diagnostic performance of the AI model for PCR-confirmed influenza infection includes an AUROC of 0.90, with sensitivity and specificity of 76% and 88% respectively [5]. Therefore, evaluation of AI and Ag test results in PCR-confirmed cases is warranted to more accurately assess diagnostic differences between the two tests. Second, immunological background information was not analyzed as a potential confounding factor. Given that the AI system operates on the basis of host immune responses, such background factors may influence AI test performance. For example, previous studies have reported stronger vaccine-related adverse reactions among individuals with autoimmune disorders or allergy histories following mRNA COVID-19 vaccination [13]. Incorporating immunological background information as an additional input may further refine and improve the diagnostic accuracy of AI systems. Third, the study population was predominantly paediatric (median 14 years, with relatively few elderly participants (adult median age 36.5 years). Further studies including a larger number of elderly patients are warranted to better assess the impact of age and to confirm the potential advantages of AI-based diagnosis leveraging host immune responses in paediatric populations. Finally, because of the limited sample size for analyses, several variables showed statistically significant associations accompanied by wide 95% confidence intervals—such as cough and fever in Table 3—indicating the need for cautious interpretation.
In conclusion, this study highlights the differences in patient backgrounds and symptoms between cases testing positive by conventional rapid Ag assays and those testing positive by a novel AI-powered pharyngeal endoscopy system. The introduction of this AI-based system into point-of-care influenza diagnostics—particularly for patients tested shortly after symptom onset, paediatric patients, symptomatic individuals with fever or cough, and those with a history of contact with infected persons—may enhance diagnostic performance and help compensate for the limited sensitivity of conventional rapid Ag testing. Understanding the diagnostic mechanisms underlying each test will facilitate appropriate selection between Ag and AI testing, thereby supporting more accurate point-of-care diagnostics. Furthermore, this study underscores the potential of AI-powered medical diagnostic systems to advance pathogen differentiation in pharyngitis, including influenza and COVID-19.
Materials and methods
Ethics statement
This study was approved by the ethical review boards of Sasebo Memorial Hospital and Moriyama Clinic Ethics Committee, Japan (approval number 2023-09). The research involving human data use complied with all relevant national regulations and institutional policies and was conducted in accordance with the principles outlined in the Declaration of Helsinki. Written informed consent was obtained from all participants; for participants aged <18 years, consent was obtained from a parent or legal guardian.
Subjects and data collection
Patients aged five years or older who underwent nasopharyngeal swab-based rapid antigen testing for influenza virus and COVID-19 were recruited from Sasebo Memorial Hospital and Moriyama Clinic between February 2024 and March 2025. Rapid antigen tests were performed using kits from multiple manufacturers that are approved for clinical diagnosis and routinely used as point-of-care tests in outpatient settings. Patients younger than five years of age or those unable to comply with instructions for pharyngeal image acquisition required for AI testing were excluded from the study. A total of 864 patients were registered in the study. Among them, 51 patients (5.9%) failed to complete the AI-based influenza test because the AI system was unable to recognize the pharyngeal images. Thus, 813 patients had valid results for both Ag and AI testing. Because patient background and symptom information were collected as mandatory inputs in the AI testing system prior to image acquisition, no data were missing for these variables, and all were used in the analyses for this study. In cases where the AI system diagnosed influenza infection in patients who were positive for COVID-19 antigen and negative for influenza antigen (COVID-19 Ag + , influenza Ag-, and influenza AI+), confirmatory PCR testing for COVID-19 and influenza viruses was conducted using swab specimens at a commercial laboratory (Genesis Healthcare, Tokyo, Japan).
AI system
The AI-powered pharyngeal endoscopy system for influenza diagnosis was originally developed and reported by Okiyama et al. [5]. Briefly, the system operates as follows: (1) Input of background and symptom information: Patient background and symptom data—including sex, age, time of first symptom onset, history of contact with infected individuals, use of antipyretics, and influenza vaccination status—are collected at the outpatient visit and entered into the AI system as mandatory fields prior to testing. (2) Pharyngeal image acquisition: To ensure image quality, rapid continuous shooting (18 images over 3.0 seconds) is performed to minimize motion blur. A light-emitting diode light source and a disposable clear camera cover are used to depress the tongue and prevent fogging from exhalation. The viewing angle is appropriately restricted to reduce image distortion. The system automatically recognizes the posterior pharyngeal wall; if recognition fails, image acquisition is repeated. (3) AI-based diagnosis: The diagnostic AI model was developed using pharyngeal images and background/clinical information from PCR-confirmed influenza cases. The model is an ensemble comprising a multimodal convolutional neural network (MM-CNN), a multi-view convolutional neural network (MV-CNN), and boosting models. Data from 7,831 participants in the training stage and 659 participants in the validation stage, collected from hospitals in Japan, were used for model development. Pharyngeal images were ranked as the most influential predictors of influenza diagnosis, followed by body temperature and cough. The reported diagnostic performance of the AI model for PCR-confirmed influenza infection includes an AUROC of 0.90, with sensitivity and specificity of 76% and 88%, respectively.
Statistical analysis
Statistical analyses were performed using EZR (developed by Jichi Medical University, Saitama, Japan) [32]. To minimize bias in symptom assessment attributable to COVID-19 infection, analyses of influenza test positivity were restricted to COVID-19 Ag- cases. Differences in symptom frequencies between influenza testing-positive and influenza testing-negative cases were assessed using Fisher’s exact test. The sensitivity and specificity of the AI system relative to Ag test results were evaluated using the AUROC. The time from symptom onset to testing among the AI+ and Ag-, AI+ and Ag + , and AI- and Ag+ groups was analyzed using the Kruskal-Wallis test, followed by the Steel-Dwass test for post-hoc comparisons. Multivariate binary logistic regression was conducted to identify patient background factors and symptoms associated with (a) AI positives (AI+ and Ag-) versus Ag positives (AI- and Ag+), and (b) false-positive AI results (AI false+) versus AI negatives (AI-) among COVID-19–infected patients. Patient background and symptom variables included in the multivariate models were those collected as mandatory input information for AI testing. To assess multicollinearity among the independent variables, variance inflation factors (VIFs) were calculated, and no variable exceeded a VIF of 5 (S6 Table). Calibration was evaluated using the Hosmer-Lemeshow goodness-of-fit test, which showed no significant lack of fit (p ≥ 0.05) in each test (S6 Table).
Supporting information
S1 TableStudy dataset.(XLSX)
S2 TableDifferences in background and symptom frequencies between influenza testing positives (AI+ or Ag+) and negatives (AI- and Ag-).(XLSX)
S3 TableConcordance between antigen (Ag) and artificial intelligence (AI) testing for influenza.P values by Fisher’s exact tests are shown.(XLSX)
S4 TableDifference in influenza vaccination frequency between AI positives and Ag positives.P values by Fisher’s exact tests are shown.(XLSX)
S5 TableSubgroup analyses of differences in background and symptom frequencies between influenza AI positives (AI+ and Ag-) and Ag positives (AI- and Ag+).Results from multivariable binary logistic regression analysis are shown.(XLSX)
S6 TableVariance inflation factor (VIF) scores and Hosmer–Lemeshow goodness-of-fit test results for each binary logistic regression analysis.(XLSX)
S1 FigSensitivity and specificity of AI testing relative to Ag testing.Receiver operating characteristic (ROC) curve and the area under the curve (AUC) with 95% confidence intervals are shown.(TIF)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Takahashi H, Nagamatsu H, Yamada Y, Toba N, Toyama-Kousaka M, Ota S, et al. Surveillance of seasonal influenza viruses during the COVID-19 pandemic in Tokyo, Japan, 2018-2023, a single-center study. Influenza Other Respir Viruses. 2024;18(1):e 13248. doi: 10.1111/irv.13248 38188373 PMC 10767599 · doi ↗ · pubmed ↗
- 2Bajema KL, Bui DP, Yan L, Li Y, Rajeevan N, Vergun R, et al. Severity and long-term mortality of COVID-19, influenza, and respiratory syncytial virus. JAMA Intern Med. 2025;185(3):324–34. doi: 10.1001/jamainternmed.2024.7452 39869355 PMC 11773409 · doi ↗ · pubmed ↗
- 3Shirley JD, Bennett SA, Binnicker MJ. Current regulatory landscape for viral point-of-care testing in the United States. J Clin Virol. 2023;164:105492. doi: 10.1016/j.jcv.2023.105492 37210882 · doi ↗ · pubmed ↗
- 4Pondaven-Letourmy S, Alvin F, Boumghit Y, Simon F. How to perform a nasopharyngeal swab in adults and children in the COVID-19 era. Eur Ann Otorhinolaryngol Head Neck Dis. 2020;137(4):325–7. doi: 10.1016/j.anorl.2020.06.001 32646750 PMC 7274641 · doi ↗ · pubmed ↗
- 5Okiyama S, Fukuda M, Sode M, Takahashi W, Ikeda M, Kato H, et al. Examining the use of an artificial intelligence model to diagnose influenza: development and validation study. J Med Internet Res. 2022;24(12):e 38751.10.2196/38751 PMC 982357836374004 · doi ↗ · pubmed ↗
- 6Miyamoto A, Watanabe S. Influenza follicles and their buds as early diagnostic markers of influenza: typical images. Postgrad Med J. 2016;92(1091):560–1. doi: 10.1136/postgradmedj-2016-134271 27466411 PMC 5013091 · doi ↗ · pubmed ↗
- 7Okagawa Y, Abe S, Yamada M, Oda I, Saito Y. Artificial intelligence in endoscopy. Dig Dis Sci. 2022;67(5):1553–72.34155567 10.1007/s 10620-021-07086-z · doi ↗ · pubmed ↗
- 8Chartrand C, Leeflang MMG, Minion J, Brewer T, Pai M. Accuracy of rapid influenza diagnostic tests: a meta-analysis. Ann Intern Med. 2012;156(7):500–11. doi: 10.7326/0003-4819-156-7-201204030-00403 22371850 · doi ↗ · pubmed ↗