Active Surveillance and Polymerase Chain Reaction (PCR) Between Two Passive Surveillance Periods Improve Detection and Characterization of Pleural Empyema: A 20-Year Study in Tijuana, Mexico
Erika Z Lopatynsky, Jaime A Rodriguez-Valencia, Enrique Chacón-Cruz

TL;DR
A 20-year study in Tijuana, Mexico, showed that using active surveillance and PCR improved detection and understanding of pleural empyema in children.
Contribution
The study demonstrates how integrating active surveillance and PCR diagnostics enhances detection and vaccine impact evaluation for pleural empyema.
Findings
Active surveillance with PCR increased detection of pleural empyema cases and identified causative pathogens.
The study showed the effectiveness of pneumococcal conjugate vaccines (PCV7 and PCV13) in reducing disease burden.
Molecular diagnostics improved antimicrobial susceptibility profiling and informed better clinical management.
Abstract
Pleural empyema (PE) surveillance was conducted at Tijuana General Hospital in Tijuana, Mexico, across three distinct periods: passive surveillance (2000-2005), active clinical surveillance with the incorporation of polymerase chain reaction (PCR)-based diagnostics (2005-2018), and a subsequent return to passive surveillance (2022-2024). The implementation of active surveillance coupled with molecular diagnostics substantially improved the detection of PE cases and the identification of causative pathogens, while also enabling the evaluation of the impact of pneumococcal conjugate vaccines (PCVs), including the 7-valent vaccine (PCV7; 2005-2012) and the 13-valent vaccine (PCV13; 2012-2018). This integrated approach provided a more accurate characterization of the etiologic spectrum of PE in children and adolescents, improved antimicrobial susceptibility profiling to better inform…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
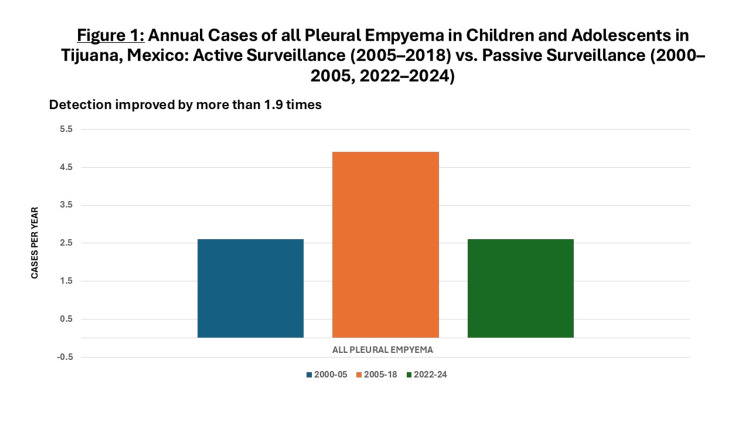 Figure 1
Figure 1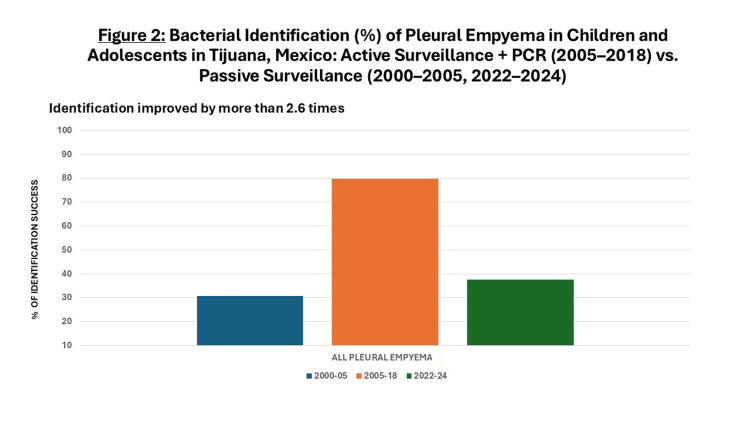 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumonia and Respiratory Infections · Pleural and Pulmonary Diseases · Microbial infections and disease research
Introduction
Pleural empyema (PE) is a serious complication of bacterial pneumonia (BN) associated with high morbidity, prolonged hospitalization, potential sequelae, and, in some cases, death [1-3]. Among children beyond the neonatal period, the leading causative pathogens of both BN and PE are Streptococcus pneumoniae, Staphylococcus aureus, and *Haemophilus influenzae *[3-6].
At Tijuana General Hospital in Tijuana, Mexico, pediatric PE was monitored across three distinct phases: passive surveillance (2000-2005), active surveillance incorporating polymerase chain reaction (PCR) diagnostics (2005-2018), and a subsequent return to passive surveillance (2022-2024).
To date, no published studies have systematically compared passive and active surveillance for PE. The objective of this study is precisely to evaluate the impact of implementing active surveillance by comparing the detection rates and characterization of all variables associated with PE during periods of passive versus active surveillance, as well as after active surveillance was discontinued.
Materials and methods
All children and adolescents aged three months to 16 years admitted to Tijuana General Hospital with a clinical diagnosis of pneumonia and chest radiography suggestive of PE underwent diagnostic thoracentesis. PE was defined by the presence of purulent pleural fluid, and patients meeting this criterion were included as cases in the study. Clinical and laboratory data were compiled in a Microsoft Excel database (Microsoft Corporation, Redmond, WA, USA), and descriptive statistical analyses were performed.
Because the study was conducted using standard-of-care procedures, the Institutional Review Board determined that formal approval was waived.
Three distinct surveillance periods were evaluated.
2000-2005: retrospective passive surveillance
Data were collected from hospital records of patients younger than 16 years diagnosed with PE.
2005-2018: prospective active surveillance
Active, prospective surveillance was initiated in the emergency department. Following pleural puncture, pleural fluid samples were immediately inoculated into radiometric broth media (BACTEC®, Becton Dickinson, Franklin Lakes, NJ, USA) and incubated at 37 °C with 5% carbon dioxide (CO₂). Final bacterial identification was performed using the Vitek/Microscan Vitek2® system (bioMérieux, Hazelwood, MO, USA).
For real-time PCR (RT-PCR), DNA was extracted from PF using the QIAamp DNA Blood Mini Kit (QIAGEN®, Shanghai, China) according to the manufacturer’s instructions. A 200 μL pleural fluid aliquot was processed, and DNA was eluted in 100 μL of TE buffer. RT-PCR was performed on the Mx3000P qPCR System (Stratagene®, La Jolla, CA, USA), targeting seven common bacterial pathogens associated with PE via specific gene markers: 16S (Escherichia coli (E. coli)), femA (Staphylococcus aureus (S. aureus)), hly (Listeria monocytogenes (L. monocytogenes)), ctrA (Neisseria meningitidis (N. meningitidis)), lytA (Streptococcus pneumoniae (S. pneumoniae)), bexA (Haemophilus influenzae (H. influenzae)), and cfb (Group B Streptococcus).
S. pneumoniae serotypes were identified by Quellung reaction (Statens Serum Institut®, Copenhagen, Denmark) and/or multiplex PCR following the CDC-recommended sequential method. Serotype-specific primers were validated with individual reference strains and subsequently tested against 5-10 additional clinical isolates to ensure broad detection within each serotype. For S. aureus, methicillin resistance was determined using 6 μg/mL oxacillin in Mueller-Hinton agar supplemented with 4% NaCl, or by PCR detection of the mecA gene.
2022-2024: passive surveillance reinstatement
Following the COVID-19 pandemic (2020-2022), when hospital admissions were limited to SARS-CoV-2 cases, passive surveillance for pediatric PE was reestablished.
Results
2000-2005: retrospective passive surveillance
Between 2000 and 2005, 13 cases of PE were reported (2.6 cases per year). Pathogens were isolated by conventional culture in only four cases (30.7%): two S. pneumoniae, one S. aureus, and one Streptococcus pyogenes (S. pyogenes). Antimicrobial susceptibility testing was not performed for S. pneumoniae isolates. For* S. aureus* and S. pyogenes, testing by the disk diffusion method showed that the S. aureus strain was susceptible to oxacillin and glycopeptides, while the S. pyogenes strain was susceptible to penicillin.
2005-2018: prospective active surveillance
Between 2005 and 2018, 64 cases of PE were actively identified (4.9 cases per year), representing a 1.9-fold increase attributable to clinical active surveillance only compared with the 2000-2005 period (Figure 1). The addition of PCR to active surveillance enabled pathogen identification in 51 cases (79.7%), a 2.6-fold improvement in detection compared to the earlier period (Figure 2). The predominant organisms were S.pneumoniae (29; 56.8%), S. aureus (14; 27.4%), and S. pyogenes (3; 5.9%). Single cases were also attributed to Peptostreptococcus sp., Pseudomonas aeruginosa (P. aeruginosa), Klebsiella oxytoca (K. oxytoca), Streptococcus salivarius (S. salivarius), and Streptococcus milleri (S. milleri).
Annual Data of all Pleural Empyema Cases in Children and Adolescents in Tijuana, Mexico: Active Surveillance (2005–2018) vs. Passive Surveillance (2000–2005, 2022–2024)
Bacterial Identification (%) of Pleural Empyema in Children and Adolescents in Tijuana, Mexico: Active Surveillance + PCR (2005–2018) vs. Passive Surveillance (2000–2005, 2022–2024)PCR: polymerase chain reaction
Detailed clinical, laboratory, imaging, treatment, and outcome data for each patient, as well as the impact of polysaccharide-protein pneumococcal conjugate vaccines (PCV7 and PCV13), have been previously published [7]. Briefly, that study reported PCV13 effectiveness of 53.8% against pneumococcal PE; however, an increase in PE caused by S. aureus was observed, predominantly due to methicillin-sensitive strains.
2022-2024: passive surveillance reinstatement
Between 2022 and 2024, eight cases of PE were reported (2.6 cases per year), representing a 1.9-fold decrease compared with the 2005-2018 period (Figure 1). Pathogens were isolated in only three cases (37.5%), reflecting a 2.1-fold reduction in bacterial identification relative to the prior period (Figure 2). The isolated organisms were S.pneumoniae, S. aureus, and *Klebsiella pneumoniae *(K. pneumoniae), one of each, with no antimicrobial susceptibility data available.
Discussion
As mentioned in the introduction, the objective of this study is precisely to evaluate the impact of implementing active surveillance by comparing the detection rates and characterization of all variables associated with PE during periods of passive versus active surveillance, as well as after active surveillance was discontinued.
For pneumococcal disease, multiple studies have demonstrated that active surveillance combined with molecular diagnostics (PCR) is crucial-not only for improving case detection across the spectrum of pneumococcal infections, but also for monitoring serotype dynamics following the introduction of PCVs. This approach enables a more accurate characterization of clinical outcomes, sequelae, morbidity, mortality, and the identification of other pathogens involved [8-15].
Particularly for PE, there are various publications of pediatric PE by implementing active surveillance.
In Germany, Forster et al. conducted a prospective study using PCR to evaluate the impact of prehospital antibiotic therapy on clinical outcomes and pathogen detection in 1,724 children with parapneumonic pleural effusion or empyema between 2010 and 2018. Their findings showed that while prehospital antibiotic administration significantly reduced bacterial pathogen detection by culture, it did not affect detection by PCR. Moreover, prehospital antibiotic use was associated with fewer infectious complications but did not influence the overall duration of illness [16].
In Turkey, pleural fluid samples from 156 children diagnosed with pneumonia complicated by empyema across 13 hospitals between 2010 and 2012 were collected via thoracentesis and tested for 14 S. pneumoniae serotypes/serogroups using a Bio-Plex multiplex antigen detection assay. The estimated serotype coverages for PCV7, PCV10, and PCV13 were 16.3%, 45.4%, and 60%, respectively. The authors concluded that active surveillance studies are essential to monitor shifts in S. pneumoniae serotypes causing empyema, in order to guide optimal pneumococcal vaccine selection [17]. Similar results were found in children with parapneumonic pneumonia in Italy and Japan [18, 19].
Our first publication in 2019 not only demonstrated an increase in the detection of PE cases but also provided enhanced insights into: (1) clinical, demographic, and patient outcomes; (2) the impact of PCV7 and PCV13 on pneumococcal serotype distribution and replacement; and (3) the contribution of pathogens other than S. pneumoniae [7]. Additionally, through active surveillance combined with molecular diagnostics (PCR), we observed the emergence of PE cases caused by S. aureus.
Although studies from the United States have not shown an increase in S. aureus-associated pneumonia following PCV13 implementation [20], several reports have documented a potential rise in S. aureus-related PE cases after the introduction of PCV13.
In Italy, Carloni et al. analyzed 43 pediatric cases and found a significant reduction in hospitalizations for necrotizing pneumonia (including PE) between the early (1.5/1000 admissions/year) and intermediate (0.35/1000 admissions/year) post-PCV13 periods (p = .001), followed by an increasing trend thereafter. S. pneumoniae remained the predominant pathogen in both periods (pre-PCV13: 11/18, 61%; post-PCV13: 13/25, 52%), with serotype 3 being the most frequent strain (pre-PCV13: 3/11, 27%; post-PCV13: 4/13, 31%). Although the overall etiology did not change substantially over time, most infections caused by S. pyogenes or S. aureus occurred during the post-PCV13 period [21].
In Germany, Lise et al. conducted a prospective study incorporating PCR in 1,447 children with parapneumonic pleural effusion or empyema between 2010 and 2017. Their findings showed an increase in S. pyogenes infections following PCV13 introduction, but no corresponding rise in S. aureus cases [22].
It is imperative to acknowledge the following limitations of this study. Prior to the implementation of active surveillance, the presence of purulent pleural fluid constituted the operational definition of PE at our institution. To ensure methodological consistency and comparability across all three study periods, we maintained this definition and therefore excluded non-purulent cases. We acknowledge that this approach may have resulted in the exclusion of some non-purulent PE cases; however, it allowed for consistent case ascertainment across study periods.
Additionally, incidence rates and corresponding confidence intervals could not be estimated because population-based denominators were unavailable, as Tijuana General Hospital does not serve a clearly defined catchment population. However, our study is the first to directly compare the benefits of implementing active surveillance and to demonstrate the substantial loss of essential epidemiologic information that occurs when this methodology is discontinued. At the time PCR was implemented during the active surveillance period (2005-2018), although sensitivity for certain pathogens may have been moderate (approximately 60-70%), the specificity of this molecular approach was close to 100%. However, despite these limitations, our study also has significant strengths.
Beyond pathogen identification and shifting serotype patterns, this study underscores that the true value of active surveillance lies in its ability to drive evidence-based decision-making for national immunization programs by complementing passive surveillance and clinical trials [22].
Robust surveillance systems-especially those strengthened with enhanced and molecular tools such as genotyping-generate the high-quality, timely, and comprehensive data needed to evaluate vaccine effectiveness, ensure safety, sustain public confidence, and guide rational vaccine introduction [23-26].
Importantly, these systems create a continuous quality-improvement loop, enabling health authorities to monitor disease epidemiology, rapidly detect vaccine-preventable threats, and refine immunization strategies as new evidence emerges. In this way, active surveillance becomes not only a technical activity but a foundational mechanism that informs clinical practice, shapes public health policy, and ultimately strengthens both routine immunization efforts and future pandemic preparedness [27-28].
Conclusions
Active surveillance, incorporating immediate culturing and PCR sampling in the emergency department, doubled the detection rate of PE cases compared to passive surveillance. The combination of rapid culture and PCR enabled a 2.6-fold increase in bacterial identification, improved antimicrobial susceptibility testing, and supported more informed antibiotic decision-making.
Based on our observations, establishing active surveillance with molecular diagnostics also enabled evaluation of PCV effectiveness, with PCV13 demonstrating a strong impact in reducing pneumococcal PE, particularly those caused by vaccine-included serotypes.
As a surprising observational finding, PCV13 effectiveness for all pneumococcal PE was also associated with an increase in staphylococcal PE. Reinstating active surveillance with PCR is strongly recommended to ensure comprehensive pathogen detection and accurate epidemiologic monitoring and drive evidence-based vaccine policy-decision-making.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Empyema in children Turk Gogus Kalp Damar Cerrahisi Derg Kuru M Altinok T 03632202410.5606/tgkdc.dergisi.2024.25759 PMC 1099567938584781 · doi ↗ · pubmed ↗
- 2Parapneumonic empyema in children: a scoping review of the literature Ital J Pediatr Buonsenso D Cusenza F Passadore L 1365020243908079410.1186/s 13052-024-01701-1PMC 11290072 · doi ↗ · pubmed ↗
- 3Burden of all-cause and organism-specific parapneumonic empyema hospitalization rates prior to the SARS-Co V-2 pandemic in the United States Respir Med Wiese AD Grijalva CG 10711120720233659263910.1016/j.rmed.2022.107111 PMC 9803378 · doi ↗ · pubmed ↗
- 4Correction to: incidence, etiologies, and outcomes of severe pediatric community-acquired empyema before and after the pandemic: an Italian multicentric study Eur J Pediatr Buonsenso D Montagnani C Romani L 71318420254113137010.1007/s 00431-025-06521-x PMC 12549715 · doi ↗ · pubmed ↗
- 5Changes in empyema among U.S. children in the pneumococcal conjugate vaccine era Vaccine Wiese AD Griffin MR Zhu Y Mitchel EF Jr Grijalva CG 624362493420162783291810.1016/j.vaccine.2016.10.062PMC 5552045 · doi ↗ · pubmed ↗
- 6Emergence of parapneumonic empyema in the USA Thorax Grijalva CG Zhu Y Nuorti JP Griffin MR 6636686620112161716910.1136/thx.2010.156406 PMC 4820002 · doi ↗ · pubmed ↗
- 712 years active surveillance for pediatric pleural empyema in a Mexican hospital: effectiveness of pneumococcal 13-valent conjugate vaccine, and early emergence of methicillin-resistant Staphylococcus aureus Ther Adv Infect Dis Chacon-Cruz E Rivas-Landeros RM Volker-Soberanes ML Lopatynsky-Reyes EZ Becka C Alvelais-Palacios JA 2049936119839312620193098439610.1177/2049936119839312 PMC 6448099 · doi ↗ · pubmed ↗
- 8Molecular analysis improves pathogen identification and epidemiologic study of pediatric parapneumonic empyema Pediatr Infect Dis J Blaschke AJ Heyrend C Byington CL 2892943020112105737210.1097/INF.0b 013e 3182002 d 14PMC 3053443 · doi ↗ · pubmed ↗