Beyond the spike: Functional (dissociative) seizures as a key to holistic attitudes in seizure disorders
Mahinda Yogarajah, Barbara Dworetzky, Josemir W. Sander, Angel Aledo‐Serrano

TL;DR
This paper suggests that understanding functional seizures can improve care for all seizure patients by adopting a holistic approach.
Contribution
The paper highlights the mechanistic overlap between epileptic and functional seizures, advocating for a unified biopsychosocial approach.
Findings
Functional and epileptic seizures share mechanisms involving interoception, emotion, and stress dysregulation.
Both seizure types have similar rates of psychiatric and neurological comorbidities.
A holistic approach benefits all seizure patients and aligns with modern epilepsy care models.
Abstract
Epileptologists can improve outcomes through follow‐up and coordination of care for patients with functional seizures. Epileptic and functional seizures share some mechanistic overlap involving interoceptive, emotional, and stress dysregulation, and disorders of agency and perception. Similar psychiatric and neurological comorbidities occur at comparable rates in both functional and epileptic seizure populations. A holistic, biopsychosocial approach benefits all seizure patients and reflects modern models of epilepsy care.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
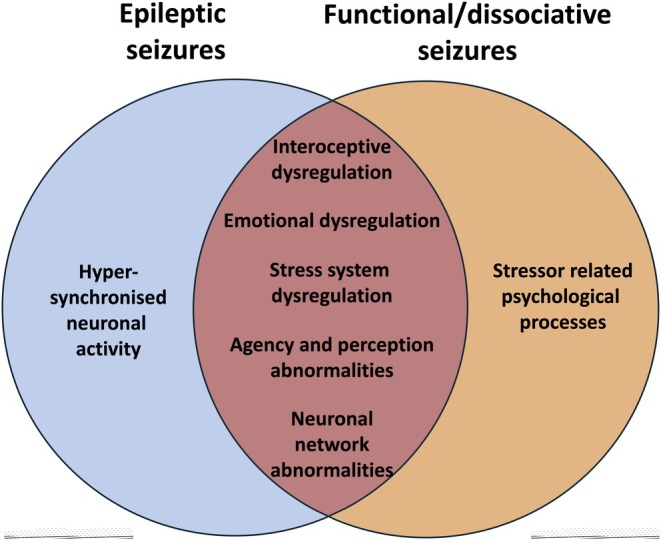 FIGURE 1
FIGURE 1| Domain | Rationale |
|---|---|
| Prevalence & burden | Functional seizures are common in seizure clinics and carry similar morbidity, mortality, and health care costs as epilepsy |
| Clinical responsibility | Neurologists diagnose FDS and are well placed to optimize ASM use, assess new symptoms, and coordinate care |
| Treatment impact | Even brief neurologist‐led interventions (e.g., motivational interviewing, outpatient follow‐up) can reduce seizure frequency and improve outcomes |
| Comorbidity overlap | High rates of psychiatric and neurological comorbidities (e.g., PTSD, ASD, TBI) are present in both FDS and epilepsy |
| Mechanistic convergence | Shared network dysfunction, stress biology, autonomic and interoceptive pathways, and abnormalities of perception link FDS and epilepsy |
| Therapeutic cross‐benefit | Neurobehavioral therapies developed for FDS may benefit epilepsy patients, suggesting overlapping treatment targets |
| Mixed diagnosis | Many patients have both epileptic and functional seizures, requiring integrated and nuanced management |
| Changing models of epilepsy | Network‐based and biopsychosocial models of epilepsy align with FDS frameworks, challenging rigid spike‐based definitions |
| Health system precedent | Other specialties (e.g., gastroenterology, movement disorders) take active roles in managing functional conditions |
- —Medical Research Council10.13039/501100000265
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPsychosomatic Disorders and Their Treatments · Epilepsy research and treatment · Mental Health and Psychiatry
INTRODUCTION
1
People with functional or dissociative seizures (FDS) are at least as common as those with multiple sclerosis,1, 2, 3 with an incidence ≈3/100 000/year and prevalence of 24–109/100 000. However, these values likely underestimate the true frequency, given that most studies restrict case ascertainment to video‐electroencephalographic (EEG) telemetry‐confirmed diagnoses, which is the minority in routine practice. In a typical seizure disorder clinic, more than one fifth of people attending for the first time have FDS and not epileptic seizures (ES).4 Beyond diagnostic considerations, however, epilepsy specialists and funding agencies are often reluctant to engage clinically and academically with this disorder. FDS are typically dismissed as outside the remit of epileptologists. Arguments against involvement include the absence of hypersynchronized neuronal discharges in FDS and the perceived greater psychiatric complexity of these individuals.5 The result is a significant gap in care and research funding.6 This neglect has clinical and economic consequences, as people with FDS incur health care costs,7 morbidity levels,8 and premature mortality rates9 similar to those associated with ES.
We highlight the inherent contradictions in these arguments (Table 1). We advocate that seizure specialists should take a more central clinical and academic role regarding FDS, ideally within a multidisciplinary framework.
A ROLE BEYOND MAKING A DIAGNOSIS
2
Because people with FDS present to seizure disorder clinics, specialists in these settings have an established diagnostic role. However, the idea that this is their only role, while management and research are left to others, is at odds with other functional disorders. Although specialized epilepsy‐led multidisciplinary services for FDS are limited, there exist gastroenterology‐led and coordinated multidisciplinary services for irritable bowel syndrome.10 Even within neurology, in an international survey of 864 movement disorder specialists, 60% considered that their primary responsibility was not only to provide a diagnosis, but also to coordinate interdisciplinary management of functional movement disorders.11 This is in contrast to the opinions expressed by epileptologists in a comparable study where only a minority held similar views.12
In individuals with FDS alone, seizure specialists play an essential research and clinical role. Even the minimum of care, that is, the provision of follow‐up appointments, has indirect benefits. Seizure specialists are best placed to wean inappropriately prescribed antiseizure medications (ASMs), assess new seizure manifestations, and manage common comorbid neurological conditions such as migraine. Optimizing the management of these conditions typically improves the frequency of the FDS.13 More implicit benefits arise from the finding that people with FDS view their seizures as biological and psychological.14 Continuing neurology input leads to increased engagement with psychological/psychiatric services, resulting in improved outcomes. In the CODES (Cognitive Behavioral Therapy Versus Standardized Medical Care for Adults With Dissociative Non‐Epileptic Seizures) study, which is the largest study of cognitive behavioral therapy (CBT) in FDS, there was no difference in seizure frequency when comparing standardized medical care alone and standardized medical care with CBT.15 This may partly have been because standardized medical care consisted of structured neurology input, alongside psychiatric follow‐up.16 A smaller Australian study showed significant health economic savings in individuals with FDS when there was continuing neurology follow‐up.17
With appropriate resources and training, interested seizure disorder specialists could provide more direct care for these individuals. This could range from helping to coordinate multidisciplinary care among psychiatrists and psychologists already embedded within a seizure disorder service18 to delivering brief but impactful interventions. A randomized controlled trial showed that a neurologist with minimal training and using a single 30‐min session of motivational interviewing doubled psychotherapy uptake. Moreover their interviewing also led to a measurable reduction in seizure frequency, even among those who never accessed therapy.19
Lastly, seizure disorder specialists should also engage with this condition beyond diagnosis, because of the frequent co‐occurrence of both epileptic and functional seizures.20 The challenge is not only to distinguish between the two seizure types, but to manage them holistically, especially given that one is primarily treated pharmacologically with ASMs, and the other requires a multidisciplinary, nonpharmacological approach.
Seizure specialists have the expertise to make a diagnosis of FDS, and general psychiatrists are frequently either skeptical regarding the diagnosis or lack confidence and experience in managing it.5, 21 It is therefore essential that seizure specialists step forward to help coordinate the management and deliver care to these individuals.
BIOLOGY BEYOND HYPERSYNCHRONIZATION
3
Despite the disinterest in FDS, epilepsy specialists readily engage clinically and academically with other types of seizures in individuals without epilepsy, such as provoked seizures caused by other conditions. The argument offered is that there are common seizure mechanisms, such as neuronal hypersynchronization, so that the study of provoked seizures can help to understand how external and/or internal factors modulate epileptic seizures. However, FDS also provide a window for understanding how other, more distal mechanisms may be relevant in epileptic seizures. Research into the neurobiology of FDS has shown that stress biology, autonomic and interoceptive dysfunction, and emotional dysregulation can modulate FDS.22 These biological systems are also relevant to people with epilepsy, where it is accepted that autonomic dysfunction has a role in sudden unexpected death in epilepsy.23 Psychological stress can exacerbate ES, and emotional dysregulation plays a role in psychiatric comorbidity and quality of life.24 The overlap is reflected in contemporary mechanistic models of functional neurological disorders and FDS. These disorders can be conceptualized within the framework of abnormal functioning of relevant brain networks, such as the default mode, salience and attentional networks, alongside psychosocial factors.25 This network‐based perspective aligns with recent shifts in epilepsy research, where the disorder, and especially interictal comorbidity, are now increasingly viewed as a disruption across interconnected brain systems.26, 27 In acknowledging the possibility of mechanistic overlap, it follows that treatment for FDS may offer some benefit to those with epileptic seizures. A prospective trial of neurobehavioral therapy demonstrated that a structured, multimodal psychotherapy originally developed for FDS could also significantly reduce seizure frequency in people with epilepsy during the active treatment phase.28 The epilepsy cohort experienced a 34% reduction in monthly seizure frequency during neurobehavioral therapy, with seizure freedom achieved in 74% of participants by the end of treatment. However, these gains were not sustained at the 1‐year follow‐up. These improvements occurred without changes to ASMs. They may be due to shared neurobiological mechanisms between epilepsy and FDS, involving arousal, stress, and emotional regulation, all of which are targeted in neurobehavioral therapy. Neurobehavioral therapy integrates cognitive, psychodynamic, mindfulness, and self‐regulation strategies, which may support improved seizure control through greater self‐awareness, reduction of trigger sensitivity, and enhanced stress resilience. The observed improvements suggest that such therapies warrant further exploration in epilepsy care as adjunctive treatments.
Other mechanistic overlaps have emerged through the use of long‐term subcutaneous EEG recordings in people with epilepsy.29 Individuals report events that are not epileptic seizures and miss events that are epileptic seizures. The most recent study of long‐term subcutaneous EEG recording in 31 individuals with epilepsy over 6 months noted that self‐reported nonepileptic events (n = 84) and unreported electrographic seizures (n = 14) both outnumbered self‐reported electrographic seizures.30 This raises a critical question: where do ES end and FDS begin in these individuals, most of whom would not be categorized as having "typical functional seizures." In ES, there are inherent and underexplored disturbances in perception, agency, and consciousness, concepts that fundamentally define functional seizures.31
Taking more of an interest in the biological underpinnings of FDS may help us understand why seizure reporting is often inaccurate in ES, and how higher order factors such as stress, attention, and emotion affect epileptic seizures. Dismissing FDS because they lack EEG spikes risks ignoring mechanisms relevant to both conditions (Figure 1).
The mechanistic overlap between epileptic and functional/dissociative seizures.
BEYOND ASMs: NEED FOR A BIOPSYCHOSOCIAL APPROACH
4
Some argue that FDS are too complex because of significant psychosocial comorbidities. However, one third of people with FDS have no significant psychiatric comorbidity.16 In the remainder, although meta‐analyses confirm that psychiatric comorbidity is approximately 1.3 times more common in FDS than ES,32 there are high levels of psychiatric comorbidity in drug‐resistant epilepsy, with rates of >50% in large studies.33 Psychiatric comorbidities traditionally associated with FDS such as posttraumatic stress disorder and somatic symptom disorder are now recognized to be present at elevated rates (18%34 and 24%,35 respectively) in people with ES. There are complex interactions between comorbidities, including depression, anxiety, and somatic symptom disorder, that determine the quality of life in ES individuals.36, 37 Similarly, autism spectrum disorder38 and traumatic brain injury,39 which have long been associated with epilepsy, are now recognized in nearly 20%40 and 70%,41 respectively, of individuals with functional seizures. Comorbidities in both disorders have roots in a complex interplay of biological, psychiatric/psychological, and social processes. Complexity is not unique to FDS. The biopsychosocial model, long recognized as integral to the management of FDS, should be extended to those with ES, where it may likewise improve outcomes.42
THE WAY FORWARD
5
If one defines epilepsy so narrowly that only spike‐driven events fall within its remit, one must accept that this definition also fails many of those with epilepsy too, particularly those with unmeasurable, subjective, or comorbid phenomena that nonetheless define their lived experience. If this is acknowledged, then it follows that epilepsy specialists have a central role in treating what individuals experience as seizures, regardless of mechanism. FDS, especially when comorbid with epilepsy, falls squarely within the remit of an epileptologist.
Functional seizures offer valuable insights and relevant information to enhance our understanding of ES and their management. Integrating FDS into epilepsy practice and research is feasible and essential to the holistic evolution of comprehensive care and research. We urge funding agencies to include functional seizures in research agendas, and health care providers to foster a more inclusive environment that addresses the multifaceted nature of seizure disorders. Interdisciplinary training, research grants, and integrated care models are avenues to enhanced understanding, improved individual and quality of life outcomes, and lower health care costs regardless of seizure type.
AUTHOR CONTRIBUTIONS
All authors contributed to all aspects of the article.
FUNDING INFORMATION
M.Y. is funded by an MRC CARP award (MR/V037676/1).
Abbreviations: ASD, autism spectrum disorder; ASM, antiseizure medication; FDS, functional or dissociative seizures; PTSD, posttraumatic stress disorder; TBI, traumatic brain injury.
CONFLICT OF INTEREST STATEMENT
M.Y. has served as a consultant providing specialist medicolegal advice regarding functional seizures. B.D. is president of the Functional Neurological Disorder Society. The other authors have no conflicts of interest to declare concerning this article. We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Villagrán A , Eldøen G , Duncan R , Aaberg KM , Hofoss D , Lossius MI . Incidence and prevalence of psychogenic nonepileptic seizures in a Norwegian county: a 10‐year population‐based study. Epilepsia. 2021;62:1528–1535.34075579 10.1111/epi.16949 · doi ↗ · pubmed ↗
- 2Asadi‐Pooya AA . Incidence and prevalence of psychogenic nonepileptic seizures (functional seizures): a systematic review and an analytical study. Int J Neurosci. 2023;133:598–603.34126844 10.1080/00207454.2021.1942870 · doi ↗ · pubmed ↗
- 3GBD 2017 US Neurological Disorders Collaborators , Feigin VL , Vos T , Alahdab F , Amit AML , Bärnighausen TW , et al. Burden of neurological disorders across the US from 1990‐2017: a global burden of disease study. JAMA Neurol. 2021;78:165–176.33136137 10.1001/jamaneurol.2020.4152 PMC 7607495 · doi ↗ · pubmed ↗
- 4Lee SH , Gillespie C , Bandyopadhyay S , Nazari A , Ooi SZY , Park JJ , et al. National audit of pathways in epileptic seizure referrals (NAPIER): a national, multicentre audit of first seizure clinics throughout the UK and Ireland. Seizure Eur J Epilepsy. 2023;111:165–171.10.1016/j.seizure.2023.08.01037639958 · doi ↗ · pubmed ↗
- 5Rawlings GH , Reuber M . Health care practitioners' perceptions of psychogenic nonepileptic seizures: a systematic review of qualitative and quantitative studies. Epilepsia. 2018;59:1109–1123.29750340 10.1111/epi.14189 · doi ↗ · pubmed ↗
- 6Stephen CD , Fung V , Perez DL , Espay AJ . Comparison of inpatient and emergency department costs to research funding for functional neurologic disorder: an economic analysis. Neurology. 2025;104:e 213445.39999398 10.1212/WNL.0000000000213445 PMC 11863780 · doi ↗ · pubmed ↗
- 7O'Mahony B , Nielsen G , Baxendale S , Edwards MJ , Yogarajah M . Economic cost of functional neurologic disorders: a systematic review. Neurology. 2023;101:e 202–e 214.37339887 10.1212/WNL.0000000000207388 PMC 10351557 · doi ↗ · pubmed ↗
- 8Jungilligens J , Michaelis R , Popkirov S . Misdiagnosis of prolonged psychogenic non‐epileptic seizures as status epilepticus: epidemiology and associated risks. J Neurol Neurosurg Psychiatry. 2021;92:1341–1345.34362852 10.1136/jnnp-2021-326443 PMC 8606439 · doi ↗ · pubmed ↗