Exploring the application of generative artificial intelligence in nursing: a cross-sectional study
Jinling Wu, Mengmeng Yang, Xiujuan Wei, Yanan Zheng, Jiexin Deng

TL;DR
This study explores how generative AI is being used by nurses in China, finding high adoption rates and role-specific benefits, but also concerns about accuracy and clinical autonomy.
Contribution
The study provides empirical evidence on GAI adoption in nursing in China, highlighting usage patterns and challenges specific to the local context.
Findings
GAI has a high adoption rate (92.81%) among Chinese nurses, with seniority predicting usage frequency.
Locally developed platforms like DeepSeek and Doubao are preferred, used for tasks like generating health education materials.
Role-specific benefits include reduced administrative workload for managers and improved efficiency for clinical nurses.
Abstract
This study aims to systematically investigate the application of Generative Artificial Intelligence (GAI) in nursing practice within China. It seeks to map current usage patterns, identify perceived benefits and implementation challenges, and uncover the functional needs of nursing staff regarding GAI. Additionally, the research will assess the real-world performance and adoption of emerging local GAI platforms. The findings are expected to provide foundational evidence to guide the scientifically sound and contextually appropriate development of GAI in nursing. The convenience sampling method was used to select nurse interns, staff nurses, and nurse managers from 20 provinces between April and June 2025 as survey respondents. We designed the questionnaire through a literature review as well as evidence extraction. A panel of experts assessed the content validity of the questionnaire.…
Click any figure to enlarge with its caption.
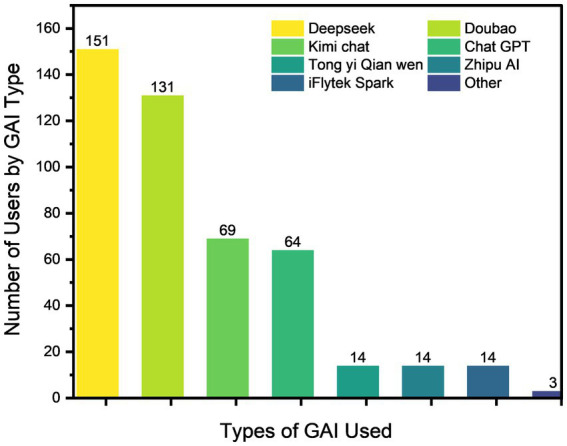 Figure 1
Figure 1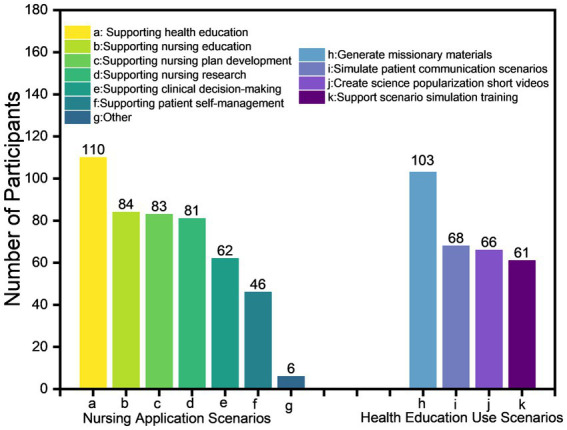 Figure 2
Figure 2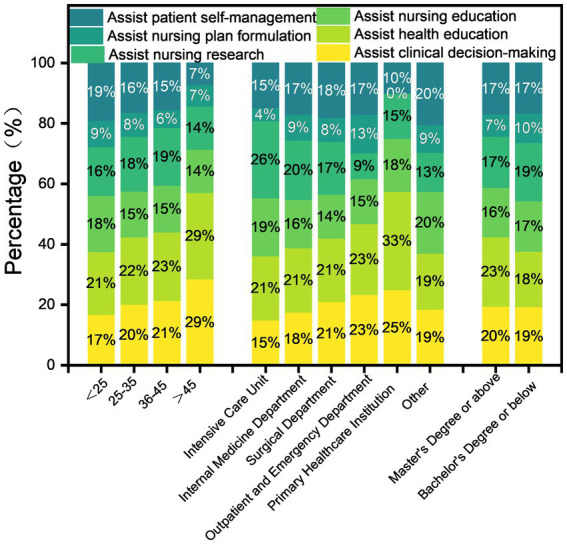 Figure 3
Figure 3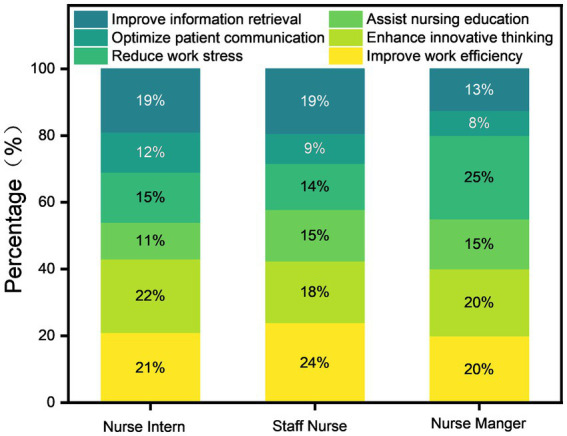 Figure 4
Figure 4| Literature | Indicators of GAI application in nursing | Contributions of GAI to nursing | Limitations of the GAI application in nursing |
|---|---|---|---|
| Von Gerich ( | Clinical decision-making | Improve information retrieval efficiency | Ethical challenges |
| O’Connor ( | Clinical Decision-making | Improve work efficiency | Risks to the accuracy of information |
| Seibert ( | Nursing Education | Improve work efficiency | Risks to the accuracy of information |
| King ( | Clinical Decision-making | Improve work efficiency | Risks to the accuracy of information |
| Wang ( | Clinical decision-making | Improve work efficiency | Ethical challenges |
| Kurniawan ( | Patient self-management | Improve work efficiency | Difficulty adapting to complex environments |
| Variables | Category | Frequency (persons) | Percentage (%) |
|---|---|---|---|
| Gender ( | Male | 23 | 12.70 |
| Female | 158 | 87.29 | |
| Age ( | < 25 | 59 | 32.59 |
| 25–35 | 85 | 46.96 | |
| 36–45 | 31 | 17.12 | |
| > 45 | 6 | 3.31 | |
| Education attainment ( | Bachelor’s degree | 136 | 75.13 |
| Master’s degree | 34 | 18.78 | |
| Associate degree | 8 | 4.41 | |
| Doctoral degree | 3 | 1.65 | |
| Hospital gradea ( | Tertiary hospital | 142 | 78.45 |
| Secondary hospital | 20 | 11.05 | |
| Primary hospital | 19 | 10.49 | |
| Geographic distribution ( | Central China | 67 | 37.1 |
| North China | 48 | 26.52 | |
| East China | 43 | 23.76 | |
| Southwest China | 11 | 6.08 | |
| South China | 9 | 4.97 | |
| Northwest China | 3 | 1.66 | |
| Type of nurse ( | Nurse intern | 29 | 16.02 |
| Staff nurse | 139 | 76.79 | |
| Nurse manager | 13 | 7.18 | |
| Departmentb ( | Surgery department | 50 | 32.89 |
| Internal medicine department | 36 | 23.68 | |
| Primary healthcare institution | 19 | 12.50 | |
| Intensive care unit | 17 | 11.18 | |
| Outpatient and emergency department | 16 | 10.52 | |
| Other | 14 | 9.21 | |
| Years of experiencec ( | <1 year | 28 | 18.42 |
| 1–5 years | 53 | 34.84 | |
| 6–10 years | 21 | 13.81 | |
| > 10 years | 50 | 32.89 | |
| Professional titled ( | Junior | 96 | 63.15 |
| Intermediate | 50 | 32.89 | |
| Senior | 6 | 3.94 |
| Category | Unstandardized coefficients | Standardized coefficients |
|
| Collinearity diagnostics | ||
|---|---|---|---|---|---|---|---|
|
| Standard error |
| VIF | Tolerance | |||
| Constant | 1.996 | 0.294 | – | 6.788 | 0.000*** | – | – |
| Age | 0.042 | 0.097 | 0.055 | 0.432 | 0.666 | 2.753 | 0.363 |
| Years of experience | −0.083 | 0.065 | −0.163 | −1.265 | 0.208 | 2.882 | 0.347 |
| Education attainment | 0.180 | 0.091 | 0.156 | 1.973 | 0.050 | 1.083 | 0.923 |
| Type of nurse | −0.037 | 0.110 | −0.029 | −0.338 | 0.736 | 1.267 | 0.789 |
|
| |||||||
| D-W value | 1.789 | ||||||
|
|
|
|
|
|
| ||
|---|---|---|---|---|---|---|---|
|
|
|
|
|
| |||
| Constant | 1.873 | 0.289 | - | 6.486 | 0.000*** | - | - |
| Age | 0.027 | 0.096 | 0.036 | 0.288 | 0.774 | 2.753 | 0.363 |
| Years of experience | −0.145 | 0.064 | −0.289 | −2.250 | 0.026* | 2.882 | 0.347 |
| Education attainment | 0.078 | 0.090 | 0.068 | 0.870 | 0.386 | 1.083 | 0.923 |
| Type of nurse | 0.199 | 0.108 | 0.157 | 1.844 | 0.067 | 1.267 | 0.789 |
|
| |||||||
| D-W value | 2.027 | ||||||
|
|
|
|
|
|---|---|---|---|
| 1. What are some of the main problems you have encountered with GAI? a( | Lack of familiarity with the generate command | 93 | 27.11 |
| Inadequate understanding of system features | 80 | 23.32 | |
| Slow system response time | 59 | 17.20 | |
| Lack of credibility in generated results | 50 | 14.58 | |
| Low patient trust in GAI-generated content | 40 | 11.66 | |
| Complexity of operation | 21 | 6.12 | |
| 2. What are your concerns about GAI? ( | Impact on autonomy in clinical decision-making | 120 | 26.61 |
| Concerns over patient privacy breaches | 81 | 17.96 | |
| Ethical conflicts and value misalignment | 76 | 16.85 | |
| Challenges in accountability attribution | 70 | 15.52 | |
| Insufficiency of emotional support in nurse–patient interactions | 59 | 13.08 | |
| Risk of role substitution in the nursing profession | 45 | 9.98 | |
| 3. If you could be trained in GAI techniques, what are the areas of interest? ( | Clinical practice training | 115 | 20.65 |
| Nursing research training | 111 | 19.93 | |
| Training in home care for assisted patients | 97 | 17.41 | |
| Basic Operations and Ethics Training | 97 | 17.41 | |
| Training in the application of the care management system | 73 | 13.11 | |
| Applied training in nursing education | 64 | 11.49 |
|
|
|
|
|
|
|---|---|---|---|---|
| 1. Which GAI capabilities are most needed in clinical nursing work? ( | Clinical operations support | GAI assistant for basic care operations | 22 | 25.90 |
| GAI-based clinical risk monitoring | 9 | |||
| GAI-facilitated nurse–patient communication | 7 | |||
| GAI-guided clinical workflow development | 5 | |||
| Expertise support | Intelligent Nursing Knowledge Update System | 25 | 19.27 | |
| Nursing Innovation Support Platform | 4 | |||
| Anthropomorphic Intelligent Thinking Engine | 3 | |||
| Clinical decision support | Smart Planning for Nursing | 7 | 18.67 | |
| Clinical Auxiliary Diagnostic Support | 10 | |||
| Evidence-based nursing decision support | 14 | |||
| Instrumental support | Intelligent Nursing Document Generation | 11 | 14.45 | |
| Intelligent PPT, image generation | 5 | |||
| Intelligent generation of health education videos | 8 | |||
| Research support | GAI-powered writing assistant | 13 | 9.03 | |
| GAI-facilitated literature analysis | 2 | |||
| health promotion | Personalized health promotion | 13 | 7.83 | |
| Emotional support | Emotional support capabilities | 5 | 4.81 | |
| Patient-centered communication facilitation | 3 | |||
| 2. What do you think are the advantages of GAI in nursing? ( | Enhancement of clinical productivity | Enhanced usability | 32 | 55.19 |
| Improved operational efficiency | 69 | |||
| Intelligent knowledge support systems | Intelligent Information Panorama | 24 | 16.94 | |
| Intelligent precision cognition | 7 | |||
| Intelligent assistance to reduce the burden | Intelligent clinical burden reduction | 21 | 14.21 | |
| Intelligent labor cost optimization | 5 | |||
| Intelligent efficiency gains in quality of care | Developing innovative thinking | 9 | 8.74 | |
| Decision support | 7 | |||
| No advantage | 9 | 4.92 | ||
| 3. What do you think are the shortcomings of GAI in nursing? ( | Low clinical accuracy | Insufficient accuracy of information | 39 | 40.96 |
| Insufficient professionalism | 29 | |||
| Lack of humanized services | Lack of empathetic response | 16 | 16.26 | |
| Depersonalization of care | 11 | |||
| Technological immaturity | Limited functionality and inefficiency | 12 | 15.66 | |
| Weak emergency decision-making capacity | 3 | |||
| Mechanical rigidity and lack of trust | 11 | |||
| Application maturity | Limitations in application and difficulty in popularization | 8 | 13.85 | |
| Weak autonomous judgment | 8 | |||
| Data security risks | 7 | |||
| Adequate | 22 | 13.25 | ||
| 4. What are your suggestions for GAI? ( | Intelligent, evidence-based nursing assistant | Providing evidence-based precision responses | 33 | 55.64 |
| Increase specialization and adaptability | 28 | |||
| Expanding the authoritative medical knowledge base | 8 | |||
| Provide concise, easy-to-understand explanations | 5 | |||
| Standardized training and smart upgrades | Standardized training in the use of GAI | 10 | 31.58 | |
| Popularization of science and dissemination of values | 9 | |||
| Technology development and performance breakthrough | 23 | |||
| Intelligent care interaction with humanization | Warm intelligent interaction | 6 | 9.77 | |
| Humanized communication | 6 | |||
| Intelligent privacy protection | Protection of privacy | 5 | 3.76 |
- —Henan University10.13039/501100004773
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsArtificial Intelligence in Healthcare and Education · Simulation-Based Education in Healthcare · Advanced Technologies in Various Fields
Introduction
1
Generative artificial intelligence (GAI) is revolutionizing digital content creation by producing high-quality, human-like outputs (1). In healthcare, the rapid advancement of AI technology is fostering innovations in medical research and driving shifts in clinical practice (2). While studies indicate that GAI has the potential to improve efficiency in domains such as clinical documentation and diagnostic support, it also presents challenges, including model hallucinations, data biases, and regulatory ambiguities (3).
Concurrently, AI is reshaping education systems by broadening educational access and enabling personalized learning; however, it also introduces challenges pertaining to curriculum adaptation, assessment methods, data privacy, and algorithmic bias (4). In the nursing sector, AI applications are anticipated to mitigate time-consuming, routine tasks, thereby optimizing service delivery and reallocating nursing time toward direct patient care (5). Additional prospective benefits encompass process optimization (6), the delivery of personalized care (7), and enhanced healthcare accessibility (8). Corroborating this, a systematic review underscores AI’s potential to improve workflow efficiency and resource utilization within clinical nursing (9).
However, the practical integration of GAI faces several significant barriers, including insufficient region-specific data, constrained clinical performance, high operational costs, a lack of clear regulatory guidelines, and uneven resource distribution (10, 11). As emphasized by Reddy et al., successful deployment requires robust data protection protocols, human-in-the-loop oversight, and rigorous local validation (11). Although studies on nurses’ perceptions and attitudes toward AI have been conducted in several countries (12, 13), systematic investigations into the current application status and post-implementation effectiveness of GAI in nursing practice remain scarce. Furthermore, research specifically addressing the functional needs of nursing staff and offering development recommendations for GAI in this field is particularly limited (13).
Furthermore, research on the integration of GAI into the daily workflows of nurses in non-Western settings—particularly within China’s unique healthcare system—remains limited. Although local GAI platforms, such as DeepSeek and Doubao, are increasingly adopted owing to their open-source architecture and user-friendly interfaces, empirical evidence regarding their practical efficacy and depth of integration into nursing workflows is still lacking.
This study aims to address these research gaps through a systematic investigation of the GAI application landscape among nurses in China. Specifically, it examines context-specific usage patterns, assesses the real-world performance of local GAI platforms, and explores how nurses’ professional roles are evolving as they interact with the functional capabilities of these technologies. In doing so, the research moves beyond the prior literature’s primary focus on preliminary attitudes and adoption willingness.
Objects and methods
2
Subjects of the survey
2.1
From April to June 2025, nursing personnel from 20 provinces (cities) spread throughout six regions of China—East China, Central China, South China, Southwest China, North China, and Northeast China—were recruited as survey participants using convenience sampling.
Participants were included if they (a) participated voluntarily and (b) held one of the following professional roles: nursing managers with at least one year of experience, licensed staff nurses, or nursing interns who had completed a minimum of 3 months of clinical rotation. Exclusion criteria were (a) withdrawal from the study, (b) provision of incomplete survey responses, and (c) age under 18 years. The study protocol received approval from the Biomedical Research Ethics Subcommittee of Henan University (Approval No. HUSOM2025-703), and Informed consent was obtained from all participants.
Survey instruments
2.2
Questionnaire development
2.2.1
The survey questionnaire was developed based on a systematic extraction of evidence from key literature. We first conducted a systematic review of major evidence-based clinical resources—including UpToDate, BMJ Best Practice, the Joanna Briggs Institute (JBI), the National Guideline Clearinghouse (NGC), and the Cochrane Library—as well as comprehensive bibliographic databases such as PubMed, Embase, Web of Science, the China National Knowledge Infrastructure (CNKI), and the Wanfang Database. Search strategies incorporated both controlled vocabulary (e.g., MeSH terms) and free-text keywords related to “Generative Artificial Intelligence,” “Chatbot,” “Large Language Model,” “Nursing,” and “Application.”
The literature search identified six key publications (14–19) that formed the basis for the questionnaire design. The final set of selected literature included three systematic reviews, two narrative reviews, and one clinical guidance document. All selected publications underwent a rigorous quality assessment and satisfied the predefined inclusion criteria.
Based on the synthesis of this literature, a structured framework was developed, encompassing six application indicators, 11 application limitations, and six potential contributions of GAI to nursing (Table 1). This framework subsequently informed the initial draft of the questionnaire.
Questionnaire refinement and structure
2.2.2
Based on the initial draft, a pilot test was administered to a convenience sample of 30 nursing professionals in Beijing, encompassing nurse interns, staff nurses, and nurse managers with diverse levels of clinical experience. Feedback regarding item ambiguity and clarity was incorporated to refine the wording, yielding the final version of the questionnaire.
The finalized instrument consisted of five sections: 1. Demographic Information (10 items on institutional and individual characteristics); 2. Current Status of GAI Application (10 items on GAI utilization at the individual level); 3. Departmental Integration of GAI Technology (3 items on current departmental adoption); 4. Evaluation and Perspectives on GAI (6 items on GAI evaluation, implementation barriers, and training interests); and 5. Open-Ended Questions (4 items on desired functionalities, perceived benefits, potential limitations, and general suggestions for GAI applications).
Validity assessment
2.3
To ensure the methodological rigor of the newly developed survey instrument, a formal content validity assessment was conducted. An expert panel comprising six nursing professionals with specialized backgrounds in smart nursing (n = 2), nursing management (n = 1), inpatient nursing (n = 2), and outpatient nursing (n = 1) was convened. Panel members had professional experience ranging from 18 to 26 years, held bachelor’s (n = 2) or master’s (n = 4) degrees, and included four senior-level and two intermediate-level professionals.
The assessment employed a standard 4-point rating scale (1 = not relevant, 4 = highly relevant) to evaluate each item’s relevance to the research topic of “generative artificial intelligence applications in nursing.” Results were quantified using both the Item-level Content Validity Index (I-CVI) and the Questionnaire-level Content Validity Index (S-CVI).
The analysis established robust content validity. I-CVI scores ranged from 0.833 to 1.000, exceeding the accepted threshold of 0.78 for item-level validity (20). The Questionnaire-level Content Validity Index/Universal Agreement (S-CVI/UA) reached 0.833, while the Questionnaire-level Content Validity Index/Average (S-CVI/Ave) was 0.972. These indices meet or surpass established benchmarks for satisfactory content validity (S-CVI/UA ≥ 0.8; S-CVI/Ave ≥ 0.90) (21, 22), confirming that the questionnaire demonstrates strong content validity at both item and overall instrument levels.
Data collection
2.4
The sample size was determined according to the Kendall (23)method, which recommends 5 to 10 times the number of questionnaire items. With 24 core items (excluding demographic questions) and an anticipated 20% rate of invalid responses, the minimum required sample size was calculated as 150. The study ultimately recruited 181 participants, exceeding this minimum threshold.
The questionnaire was administered electronically in a structured online format. Prior to commencing the survey, all participants were presented with an informed consent form. Only those who provided their digital consent were granted access to and could proceed with the subsequent questions. To improve response efficiency and maintain data integrity, technical restrictions were implemented to permit only one response per device. The questionnaire was configured to require responses for all closed-ended items and employed conditional branching, whereby subsequent questions were dynamically presented based on participants’ prior selections. Upon data collection, invalid responses were excluded according to the following pre-specified criteria: (a) uniform responses across all items; (b) completion time of less than 200 s; (c) logically inconsistent answers; and (d) blank responses to all open-ended questions.
Statistical analysis
2.5
Missing data were restricted to the four open-ended questions. As these items were optional and positioned at the end of the questionnaire, their missing responses were deemed Missing Completely at Random (MCAR). Accordingly, analyses about these questions were conducted only among respondents who provided answers. The number of excluded cases in each analysis was minimal and had a negligible impact on the overall results.
Data were managed in Excel and analyzed using SPSS 27.0. Normally distributed continuous variables are presented as mean ± standard deviation, non-normally distributed variables as median and interquartile range, and categorical data as frequency (percentage). Between-group differences were assessed using the chi-square test for categorical variables and one-way analysis of variance (one-way ANOVA) for continuous measures. Associations with key outcomes were examined through multiple linear regression and binary logistic regression, with results reported as regression coefficients (for linear regression), odds ratios (for logistic regression), and their respective 95% confidence intervals. A p-value < 0.05 was considered statistically significant.
Results
3
General information on respondents
3.1
The final sample consisted of 181 valid questionnaires out of 200 distributed, resulting in an effective response rate of 90.5%. Geographically, the respondents were predominantly from Central, North, and East China. The number of nurses per department exhibited a skewed distribution, with a median of 18 (IQR: 12–27) and a range from 2 to 260. Detailed demographic characteristics of the nursing staff are summarized (Table 2).
Description of the current status of the GAI application
3.2
Among the 181 nurses surveyed, 168 (92.81%) reported using GAI. Chi-square analysis revealed no significant differences in GAI usage across age, work experience, education level, or professional roles (all p > 0.05), as shown in Supplementary Table B-1. A binary logistic regression model further confirmed that none of these demographic variables were significant predictors of GAI adoption (all p > 0.05), as all odds ratios had confidence intervals including 1: age (OR = 1.113, 95% CI: 0.325–3.817), work experience (OR = 1.160, 95% CI: 0.495–2.719), education level (OR = 0.834, 95% CI: 0.242–2.882), and type of nurse (OR = 0.356, 95% CI: 0.077–1.657). These results indicate that GAI adoption among Chinese nurses is not limited to specific demographic subgroups, suggesting the involvement of broader influencing factors, shown in Supplementary Table B-2.
The frequency of GAI usage among nurses was distributed as follows: 35.12% (59) reported using it several times per week, 27.38% (46) occasionally, 21.43% (36) frequently, 11.31% (19) several times per month, and 4.76% (8) once daily. One-way ANOVA revealed significant differences in usage 4.76% (8) frequency by age (F = 3.317, p = 0.021) and work experience (F = 7.501, p < 0.001), as shown in Supplementary Table B-3. These findings were further supported by multiple linear regression, which identified work experience as a significant positive predictor of usage frequency (B = 0.507, t = 3.326, p = 0.001) in an overall statistically significant model (F = 6.322, p < 0.001), as shown in Supplementary Table B-4.
Regarding the types of GAI used, non-domestic tools accounted for only 64 (13.91%) of the user base, whereas the local platforms DeepSeek and Doubao constituted 151 (32.83%) and 131 (28.48%) of users, respectively (Figure 1). This notable preference for domestic platforms likely reflects their enhanced Chinese language processing capabilities, fits more naturally into the digital tools nurses already use daily, and reduces accessibility barriers for users in China.
Describing the types of GAI usage.
In nursing application scenarios, 110 (65.48%) nurses employ GAI as a health education tool. Among these, 103 nurses (61.30%) used GAI to generate textual and graphic content for health education (Figure 2). This may be attributed to GAI’s ability to efficiently create patient education materials, thereby compensating for nurses’ time constraints. The usage scenarios of GAI across departments, age groups, and education levels are as shown in Figure 3.
Descriptive summary of GAI functions across usage scenarios.
Descriptive overview of GAI use scenarios across education, department, and age groups.
An “Other” option was incorporated to encompass unanticipated scenarios; its uptake was negligible (e.g., only six participants selected it for GAI applications), and all open-text responses were devoid of substantive content.
Description of the current status of GAI use in departments
3.3
The survey on the importance of GAI in the all department showed 92 (50.82%) as average, 78 (43.08%) as important, and 11 (6.07%) as not important. The survey of the availability of training in GAI in the departments was 122 (67.4%) without training and 59 (32.6%) with training. As for whether the department used GAI techniques in clinical work, 75 (41.43%) did and 106 (58.57%) did not. The limited level of clinical application of GAI, along with the absence of a training system, reveals the challenges in transitioning the technology from awareness to clinical implementation, and further uncovers significant deficiencies in institutional support, professional capacity building, and deep integration with clinical scenarios.
Description of the evaluation and barriers to GAI
3.4
Survey results indicated that 72.39% of nurses perceived GAI outputs as accurate or very accurate, while 79.75% reported being satisfied or very satisfied with GAI. Univariate analysis revealed significant associations between perceived accuracy and education level (F = 6.977, p < 0.001) and between satisfaction and work experience (F = 3.835, p = 0.011), as shown in Supplementary Table B-3. Multiple linear regression further demonstrated that work experience significantly predicted lower satisfaction (B = –0.145, p = 0.026), while education level showed a marginally significant positive relationship with accuracy perceptions (B = 0.180, p = 0.050), as shown in supplementary material (Tables 3, 4). These findings suggest that higher education levels correlate with more favorable accuracy assessments, whereas greater clinical experience is associated with reduced satisfaction regarding GAI implementation.
The perceived benefits of GAI demonstrated role-specific patterns across nursing positions. Nurse managers reported primarily reduced work pressure, staff nurses emphasized improved work efficiency, and nurse interns highlighted enhanced innovative thinking (Figure 4). This functionally specialized assistance aligns with their distinct workflow priorities and task demands: managers benefit from administrative load reduction, clinical nurses from optimized task execution, and interns from expanded learning and innovation opportunities.
Descriptive profile of GAI benefits across caregiving roles.
Survey results identified several key challenges in GAI adoption among nurses (Table 5). The most prevalent challenge was unfamiliarity with how to formulate effective instructions for AI tools (27.11%), which is consistent with the reported lack of adequate GAI training by respondents. Concerns about the potential erosion of clinical autonomy (26.61%) primarily stemmed from underlying reliability concerns regarding GAI outputs, underscoring the necessity of human-supervised implementation frameworks. Training in clinical application skills represented the most urgently expressed need (20.65%), with no respondents selecting the “Other” category.
Description of nursing staff’s functional needs, evaluation, and technical recommendations for GAI
3.5
Analysis of functional needs revealed that clinical operational support was the most frequently requested GAI function (25.9%). Improving work efficiency was the most commonly recognized benefit (55.19%). However, concerns about insufficient clinical accuracy represented the most frequently cited barrier (40.96%), while concerns about data security were also commonly expressed. For future development, 55.64% of nursing staff recommended developing GAI as an intelligent, evidence-based nursing assistant (Table 6). These findings collectively indicate a practical demand for and generally positive reception of GAI, while underscoring persistent challenges regarding clinical accuracy.
Discussion
4
The application of GAI among a sample of Chinese nurses: high popularity and low frequency of use
4.1
The survey revealed a high adoption rate of GAI among the sampled Chinese nursing staff, indicating widespread adoption. However, usage frequency remained generally low, with only 26.19% of respondents reporting daily or more frequent use. Regression analysis identified work experience as a significant positive predictor of usage frequency (B = 0.507, p = 0.001), suggesting greater integration into daily workflows among experienced nurses, consistent with findings reported by Kang et al. (24). The most widely used GAI platforms were DeepSeek and Doubao. According to Wu (25), the broad adoption of DeepSeek across multiple fields can be attributed to its high-performance yet low-cost training paradigm, robust on-premises deployment capability, and commitment to open-source collaboration.
Our findings reveal a distinct emphasis compared to those of Biswas and Castonguay (26, 27). While their studies highlighted AI applications in nursing education and documentation automation, our research—situated within China’s unique healthcare landscape—identifies health education as the dominant application area for Generative AI. This divergence likely reflects differences in nursing informatics infrastructure maturity and region-specific priorities, particularly China’s emphasis on preventive care. Powered by its robust natural language processing and content generation capabilities, GAI is progressively transforming traditional nursing workflows (28). It generates diverse simulated cases for training (28), utilizes speech recognition to facilitate structured documentation and improve efficiency (29), and rapidly produces personalized health guidance materials to support scalable, precise patient education and preventive care (30).
In conclusion, while GAI adoption is common among Chinese nurses, the depth and frequency of its use require enhancement. To fully realize its potential, we recommend targeted training programs, optimized functional design, and the expansion of application scenarios into broader aspects of clinical practice.
The degree of importance attached to GAI by the relevant departments needs to be improved
4.2
The study found that about 56% of nursing staff reported that their departments paid limited or no attention to GAI, suggesting that organizational recognition and support for GAI need to be strengthened. This limited organizational engagement may be related to current constraints in GAI’s clinical application. For instance, Shoja et al. (31) reported that GAI achieved only 71.7% accuracy in clinical decision-making tasks, with notable risks including the omission of critical clinical details and the generation of inaccurate information, particularly in complex cases.
In terms of training provision, only 32.6% of departments in this study reported having conducted GAI-related training. This proportion is lower than that reported by Chen (32), possibly reflecting differences in hospital levels and regional technological resources across studies. This gap highlights the importance of healthcare organizations collaborating with educational institutions to develop competency-based curricula that enhance nurses’ AI literacy, including skills in critically evaluating AI outputs and the ability to adhere to ethical guidelines in practice.
Based on these findings, healthcare organizations should strengthen institutional support and establish systematic training programs. Such initiatives are essential to bridge existing gaps and effectively leverage GAI’s potential in alleviating nursing workload, enhancing service quality and operational efficiency, and thereby improving patient satisfaction.
Coexistence of high satisfaction and deep concern: the overall appraisal of GAI among surveyed Chinese nurses
4.3
Most nurses considered GAI outputs satisfactory and accurate, consistent with reports by Noy and Chan (33, 34). However, regression analysis indicated that higher education levels marginally predicted more positive accuracy perceptions (B = 0.180, p = 0.050), while greater clinical experience significantly predicted lower satisfaction (B = –0.145, p = 0.026). This divergence suggests that although nurses generally acknowledge GAI’s technical capabilities, those with extensive clinical experience maintain more critical perspectives regarding its practical implementation, potentially reflecting concerns about its integration into complex clinical workflows. Unlike prior research on overall AI attitudes (35), few studies have systematically examined attitude differences based on years of clinical experience-an area that warrants further investigation.
However, during the application process, nurses encounter a number of issues and worries. Among these issues, prominent issues included unfamiliarity with generated instructions and poor comprehension of GAI functions, consistent with Ali (36), who found that over 50% of caregivers lacked systematic knowledge of AI basics, applications, and operations. Major concerns involved loss of clinical autonomy, potential privacy breaches, and inaccurate information. Chen and Rony (37, 38) indicated that GAI training relies on extensive patient data, raising privacy risks from model queries. Rony (38) also noted that nurses often worry about human-computer tension and constrained decision-making autonomy. In terms of training needs, nursing staff expressed strong demand for GAI education, particularly in clinical practice and nursing research, echoing Rony’s (39) findings.
To support the effective integration of GAI in nursing, multi-stakeholder collaboration is essential: nursing managers should formulate guidelines and launch pilot programs to clarify nurses’ roles in reviewing GAI output; nursing educators should foster students’ critical use of GAI; and developers should improve model professionalism, optimize workflow integration, and enhance data security. These coordinated efforts will help achieve safe and effective GAI deployment to empower nursing practice.
Based on these findings, while GAI demonstrates considerable adoption potential and is generally perceived as accurate and satisfactory among Chinese nurses, its effective integration into clinical practice requires addressing critical concerns regarding operational proficiency, clinical reliability, and workflow compatibility through coordinated multi-stakeholder efforts.
Clinical needs of GAI for nursing staff and advantages and limitations of its application
4.4
While GAI holds promise for nursing, most current research focuses on its applications, with few studies investigating caregivers’ actual needs. In this study, clinical operational assistance was the most anticipated application of GAI among nursing staff, aligning with Pepito et al. (40). This may be related to China’s high job demands, work pressure, resource constraints, and nursing shortages (41). Respondents identified improved clinical efficiency as the primary benefit of GAI, consistent with Nova et al. (42). However, key limitations were identified, particularly concerning clinical accuracy and data security—issues also emphasized by Almaghaslashi et al. (43). Furthermore, nurses provided constructive suggestions for GAI development, emphasizing the hope that it evolves into a knowledgeable, evidence-based assistant capable of providing clinical decision support grounded in reliable professional data. These findings differ from those of Martin-Hammond et al. (44, 45), who reported that nurses expected AI to aid mainly in risk recognition and routine task management. These discrepancies may be explained by variations in sample characteristics, research settings, or differences in nurses’ AI awareness.
To address low clinical accuracy and data security, it is crucial to establish robust data protection and clinical review mechanisms within healthcare organizations. Concurrently, policymakers may consider advancing specialized legislation and tool certification. Such coordinated efforts will be instrumental in ensuring the compliant and safe implementation of GAI.
In summary, GAI introduces new perspectives to nursing. Nursing staff should fully recognize the advantages and limitations of GAI and take the initiative to integrate and optimize its use in practice. Meanwhile, researchers and developers should strive to enhance the clinical applicability and accuracy of AI tools to address the core demands of nursing practice effectively.
Conclusion
5
This study reveals widespread but superficial adoption of Generative AI among Chinese nurses, characterized by dominant use of local platforms and primary application in health education. We identified role-specific benefits—reducing administrative pressure for managers, improving efficiency for staff nurses, and stimulating innovation for interns. Major barriers include concerns over professional accuracy and clinical autonomy. Future development should focus on enhancing clinical accuracy and providing systematic training to facilitate GAI’s evolution into an evidence-based nursing assistant.
Limitations and future directions
6
This study has several limitations. First, the survey instrument was developed specifically for this investigation due to the lack of validated scales in this emerging field. While content validity was established through expert review, the instrument has not undergone comprehensive psychometric validation, which may influence the interpretation of its constructs. Second, the use of a convenience sampling approach, though practical, may introduce self-selection bias, potentially overrepresenting nurses already interested in digital technologies. Although the sample reflected diversity in hospital levels, regions, and roles, it is not statistically representative of the national nursing population. Third, the analysis is primarily descriptive, which precludes causal inferences regarding certain relationships among some variables. Finally, as a cross-sectional design, this study cannot assess the evolution of attitudes or long-term integration of GAI tools, underscoring the need for longitudinal or mixed-methods approaches in future research. Despite these limitations, the methodological choices were appropriate for this exploratory study, which provides a foundational evidence base for subsequent confirmatory research.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Banh L Strobel G. Generative artificial intelligence. Electron Mark. (2023) 33:63. doi: 10.1007/s 12525-023-00680-1 · doi ↗
- 2Javanmard S. Revolutionizing medical practice: the impact of artificial intelligence (AI) on healthcare. Open Access J Appl Sci Technol. (2024) 2:07. doi: 10.33140/OAJAST.02.01.07 · doi ↗
- 3Rabbani SA El-Tanani M Sharma S Rabbani SS El-Tanani Y Kumar R . Generative artificial intelligence in health care: applications, implementation challenges, and future directions. Bio Med Informatics. (2025) 5:37. doi: 10.3390/biomedinformatics 5030037 · doi ↗
- 4Huong XV. The implications of artificial intelligence for educational systems: challenges, opportunities, and transformative potential. Am J Soc Sci Educ Innov. (2024) 6:101–11. doi: 10.37547/tajssei/Volume 06Issue 03-17 · doi ↗
- 5Ronquillo CE Peltonen L Pruinelli L Chu CH Bakken S Beduschi A . Artificial intelligence in nursing: priorities and opportunities from an international invitational think-tank of the nursing and artificial intelligence leadership collaborative. J Adv Nurs. (2021) 77:3707–17. doi: 10.1111/jan.14855, 34003504 PMC 7612744 · doi ↗ · pubmed ↗
- 6Pailaha AD. The impact and issues of artificial intelligence in nursing science and healthcare settings. SAGE Open Nurs. (2023) 9:23779608231196847. doi: 10.1177/23779608231196847, 37691725 PMC 10492460 · doi ↗ · pubmed ↗
- 7Johnson KB Wei W Weeraratne D Frisse ME Misulis K Rhee K . Precision medicine, AI, and the future of personalized health care. Clin Transl Sci. (2020) 14:86–93. doi: 10.1111/cts 1288432961010 PMC 7877825 · doi ↗ · pubmed ↗
- 8Kuwaiti AA Nazer K Al-Reedy A Al-Shehri S Al-Muhanna A Subbarayalu AV . A review of the role of artificial intelligence in healthcare. J Pers Med. (2023) 13:951. doi: 10.3390/jpm 13060951, 37373940 PMC 10301994 · doi ↗ · pubmed ↗