Timing for Minimally Invasive Surgery in Lipoleiomyoma: Insights From Two Cases
Yoko Suzuki, Sakura Kataoka, Misato Ueda, Natsuki Nagashima, Asuka Yoshiara, Hidetaka Sato, Naoko Nakazawa

TL;DR
This paper discusses the timing and management of minimally invasive surgery for lipoleiomyoma through two case studies and a literature review.
Contribution
The paper emphasizes the underutilization of minimally invasive surgery for lipoleiomyoma despite its benign nature and feasibility.
Findings
Only 12 out of 50 reported cases of lipoleiomyoma were managed with minimally invasive surgery.
A laparoscopic approach is safe and feasible with proper preoperative evaluation and planning.
Abstract
Lipoleiomyoma, a subtype of leiomyoma, may demonstrate hypertrophic growth, leading to tumor enlargement and presenting with clinical features such as postmenopausal bleeding and symptoms mimicking malignancy. These characteristics highlight the importance of careful evaluation and management in outpatient settings to ensure appropriate treatment. We report two cases of lipoleiomyoma with classical scenarios. The first case was initially misdiagnosed as an ovarian tumor and managed conservatively. Following tumor enlargement, laparoscopic surgery was performed after shared decision‐making with the patient. The second case mimicked malignancy and was managed surgically via laparotomy. These cases highlight typical clinical scenarios of lipoleiomyoma. From our first case to April 2024, a review of 50 reported cases revealed that only 12 were managed using minimally invasive surgery (MIS)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
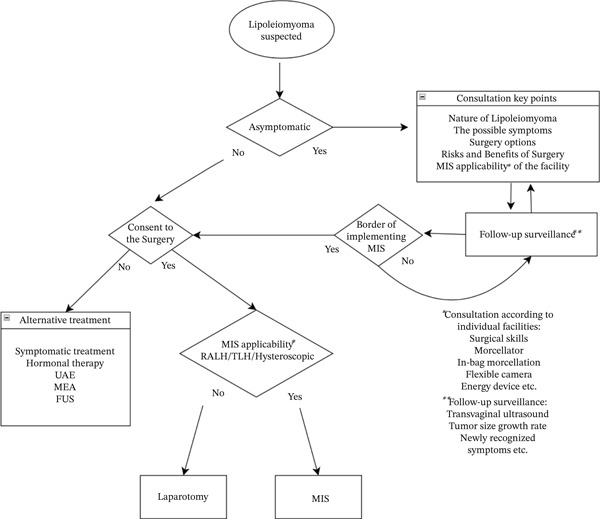 Figure 3
Figure 3| Feature | Case 1 | Case 2 |
|---|---|---|
| Age | 55‐year‐old | 49‐year‐old |
| Parity | Nulliparous | Nulliparous |
| Menopause | Postmenopausal | Premenopausal |
| Chief Complaint | Incidental finding during medical checkup | Abnormal genital bleeding for 18 days, fever(39 C) |
| Initial diagnosis | Left ovarian tumor with fatty components | Uterine sarcoma and coexisting kidney tumor |
| Ultrasound | Hyperechoic well‐circumscribed mass | Heterogeneous uterine mass |
| Imaging | MRI: 4 × 3 × 2 cm subserous uterine lipoleiomyoma | CT: 10.4 × 6.6 cm uterine mass and 2.6 cm kidney tumor |
| Complication | Hypertension, glaucoma, Type 2 diabetes mellitus, hyperlipidemia | Bacteremia (gram‐negative bacilli), suspected pyelonephritis |
| Surgery | TLH + BSO | TAH + BSO (median longitudinal incision) |
| Pathology | Lipoleiomyoma | Lipoleiomyoma, coexisting uterine leiomyomas |
| Year | Author | Age | Symptoms | Parity | Size | MP | Surgery |
|---|---|---|---|---|---|---|---|
| 2010 | [ | 60 | Abnormal vaginal bleeding for 3 months | NA | 5.6 × 4.4 | 51 | Dilatation and curettage + removal of the device + TLH |
| 2015 | [ | 55 | Hot flashes | 3 | 4 × 3.5, 2.4 × 1 | No | TLH + BSO |
| 45 | Abd discomfort | 1 | 21 × 18 | No | TLH + BSO | ||
| 2022 | [ | 55 | 4 cm size 4 years ago, increase to 5.8 cm in the last year | 2 | 6.8 × 4.5 × 0.6 | 50 | Laparoscopic resection + BSO |
| 2022 | [ | 38 | Abd Pain, AUB, pregnancy | 3 | 7 × 6 | No | Laparoscopic resection after 45 days of abortion |
| 2022 | [ | 58 | Increased urinary frequency | NA | 10 × 7 × 8 | Yes | TLH + BSO |
| 58 | AUB | NA | 1.5 × 1.4 × 1.7 | Yes | TLH + BSO | ||
| 45 | Hypermenorrhea | NA | 5.7 × 5.2 × 3.4 | No | TLH + BS | ||
| 2023 | [ | 55 | Vaginal bleeding | NA | 8.0 × 6.0 | Yes | TLH |
| 2023 | [ | 57 | 6‐month history of pelvic pain | 5 | 4 × 3 × 2.5 cm | Yes | Laparoscopic resection |
| 2023 | [ | 47 | Health checkup, asymptomatic | NA | 3.8 cm × 3.5 cm × 3.0 cm | No | Laparoscopic resection |
| 2023 | [ | 53 | AUB and difficulty emptying her bladder | 0 | 8.8 | No | RALH |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUterine Myomas and Treatments · Tuberous Sclerosis Complex Research · Ovarian cancer diagnosis and treatment
1. Introduction
Uterine lipoleiomyoma is a benign subtype of leiomyoma. The incidence rate has been reported to be about 0.03%–0.28% [1]. Once a lipoleiomyoma is diagnosed, it can be treated in the same way as a uterine leiomyoma. Asymptomatic cases typically do not require interventions. Although minimally invasive surgery (MIS) is generally preferred, a substantial proportion of reported cases ultimately require laparotomy because tumors enlarge during follow‐up or cannot be clearly distinguished from malignancy. We present two cases that highlight how these common challenges affect the timing and feasibility of MIS.
2. Case Presentation
2.1. Case 1
A 55‐year‐old postmenopausal nulliparous woman underwent a medical checkup 4 months ago, revealing a left ovarian mass. She was asymptomatic during her visit to our department. Her medical history includes hypertension and glaucoma.
2.1.1. Imaging Findings
Transvaginal ultrasonography showed a 4 × 3 × 2 cm hyperechoic (Figure 1a), well‐circumscribed mass near the left uterus with no vascularity (4.1), initially thought to be an ovarian tumor with a fatty component. MRI later identified it as a subserosal uterine lipoleiomyoma leading to a conservative follow‐up (Figure 1c).
Figure 1(a) Transvaginal ultrasound of first visit; (b) transvaginal ultrasound 1 year after during follow‐up; (c) MRI; (d) gross pathology; and (e) tissue pathology (H&E, X400).(a)(b)(c)(d)(e)
Over a year, the mass increased to 6 × 3 × 2 cm (Figure 1b). After reviewing the diagnosis and discussing options, the patient requested surgery.
2.1.2. Examination Findings
Preoperative exams revealed Type 2 diabetes mellitus and hyperlipidemia, leading to a referral to internal medicine for medication. The ophthalmologist cautioned that surgery might elevate intraocular pressure, exacerbating glaucoma due to the Trendelenburg position. Robotic hysterectomy typically requires a 25°–40° head‐down tilt, whereas laparoscopic surgery often maintains less than 20°.
2.1.3. Management
To manage her glaucoma risk, a laparoscopic total hysterectomy with bilateral salpingo‐oophorectomy was chosen. Pathology: postoperative pathology confirmed a well‐circumscribed fatty mass with multiple tan‐white whorled cut surfaces in the myometrium (Figure 1d) and scattered lipid droplets in the leiomyoma (Figure 1e). The patient recovered smoothly without complications, including no changes in glaucoma status.
2.2. Case 2
A 49‐year‐old nulliparous woman presented at the hospital with a complaint of abnormal genital tract bleeding lasting for 18 days, accompanied by a notable escalation in bleeding over the preceding 10 days. Pelvic examination revealed an intra‐abdominal mass up to the umbilicus.
2.2.1. Imaging Findings
Transvaginal ultrasound showed a heterogeneous echo of more than 10 cm mass in the anterior wall of the uterus.
Contrast‐enhanced CT imaging revealed a dense mass measuring 66 × 104 mm in the anterior wall of the uterus and a tumor located in the upper pole of the right kidney, exhibiting a heterogeneous enhancement (Figure 2a).
Figure 2(a) Contra‐enhanced CT and (b) gross pathology.(a)(b)
A dynamic contrast‐enhanced CT of the kidney was conducted 3 days after admission. A 26 mm hypovascular invasive tumor was once more observed in the right kidney, suggesting differential diagnoses of duplicate malignancies such as malignant lymphoma, Bellini′s tubular carcinoma, or a metastatic lesion from the uterine tumor.
MRI could not be conducted due to the patient′s claustrophobia.
2.2.2. Examination Findings
Cervical cytology and endometrial histology were obtained. The patient presented with a temperature of 39°C, a WBC count of 11,400/μL, and a CRP level of 13.9 mg/dL. Blood culture revealed gram‐negative bacilli, diagnosing bacteremia.
2.2.3. Management
Based on clinical findings, we first suspected a sarcoma. As inflammation subsided, a total hysterectomy with bilateral salpingo‐oophorectomy was performed via a median longitudinal incision on the 10th day postadmission. The 1‐hour, 41‐minute operation had a 150 ml blood loss, and the specimen weighed 1050 g. She recovered uneventfully and was discharged on the 8th day.
2.2.4. Pathology
Postoperative pathology showed a 10 cm yellow, soft tumor and coexisting uterine leiomyomas (Figure 2b). Histology confirmed lipoleiomyoma with mature adipose tissue.
Shortly after discharge, a comprehensive kidney tumor evaluation, including urine cytology and contrast‐enhanced CT, showed reduced hypoenhanced areas consistent with inflammatory pyelonephritis.
3. Discussion
3.1. Presented Two Case
Lipoleiomyoma predominantly affects postmenopausal women [2]. The edematous or hypertrophic changes can lead to tumor growth that mimics malignancy—often misdiagnosed with an ovarian tumor before surgery if MRI is not implemented. In addition, these tumors grow more rapidly than conventional uterine leiomyomas, complicating treatment decision‐making compared with usual leiomyomas [3].
In our institution, only two cases mentioned above were pathologically confirmed lipoleiomyoma among 798 cases of uterine leiomyoma in the past 15 years (0.25%, Table 1). These cases illustrate key diagnostic and management challenges.
The first case, initially misdiagnosed as an ovarian tumor, was correctly identified as a uterine leiomyoma via MRI. If diagnosed earlier as a leiomyoma, follow‐up might have been deemed unnecessary, potentially missing the timing for MIS.
The second case, a preexisting uterine leiomyoma, unmonitored due to menopause, coincided with an infection. Claustrophobia prevented an MRI, leading to insufficient information to rule out malignancy, resulting in a longitudinal incision that later revealed benign pathology.
These cases demonstrate some classical scenarios, as reported in a case series study in which 16% of all cases were diagnosed with another disease, such as teratoma [4]. Differential diagnosis from malignancy is occasionally problematic, especially when contrast‐enhanced MRI is unavailable, and it hinders the application of MIS [5].
4. Literature Review
To contextualize our experience, we reviewed the literature on lipoleiomyomas, including reports that specifically mentioned treatment, in PubMed, MEDLINE, and Web of Science, and identified 50 studies. Among these reports, despite this condition′s benign nature and MIS′s widespread availability, only 12 cases were reported as having been managed using MIS [6–14]. Seven laparoscopic hysterectomies, four laparoscopic tumor resections, and one robotic‐assisted hysterectomy are reported (Table 2). This reflects the situation in which most cases missed the appropriate timing for MIS despite the benign nature of the condition and the widespread availability of this surgical approach.
Bosoteanu et al. discuss a case of a giant uterine tumor identified as a lipoleiomyoma, emphasizing their potential to reach a significant size if left untreated [15]. The case for adopting laparoscopic approaches, even for larger uterine sizes previously considered unsuitable, has been strengthened by technical advancements and growing surgical expertise; the size of the uterus is no longer an absolute contraindication to endoscopic surgery.
Yuan et al. [5] provide an exhaustive literature review on the pathogenesis, diagnosis, and treatment of uterine lipoleiomyomas, detailing the role of imaging and biopsy in accurate diagnosis and the consideration for surgery in symptomatic cases or when the diagnosis is uncertain. In Japan, preoperative MRI is performed in almost all cases. Contrast‐enhanced MRI is performed when differentiation from malignancy is required based on clinical symptoms or transvaginal ultrasound findings. On the other hand, a uterine leiomyoma, without indication for surgery, would not have a regular MRI. Hence, if a leiomyoma with a significant adipose component is detected on transvaginal ultrasound, it is preferable to obtain an MRI to confirm the diagnosis. Although some reports indicate that MRI may fail to diagnose specific types with dispersed or low concentrations of fatty components [4], the tool remains a powerful tool in identifying adipose tissues.
Needless to say, MIS offers many advantages over traditional laparotomy. However, the choice between MIS and laparotomy often depends on the medical center′s policy. When retrospectively reviewing cases, some patients were initially diagnosed at a smaller stage, making them suitable candidates for MIS. Therefore, it is essential to inform patients about the institution′s capability and any size limitations associated with MIS when diagnosing lipoleiomyoma. Providing thorough informed consent facilitates shared decision‐making between physicians and patients. Ensuring patients are actively involved in choosing the most appropriate treatment approach is essential. The clinical workflow illustrated in Figure 3 underscores the versatility of laparoscopic techniques, enabling optimal tumor resection while minimizing patient burden.
Proposed flow chart of shared decision‐making in lipoleiomyoma patients and physicians.
The following situations require special attention. In small asymptomatic cases, follow‐up is often discontinued after menopause; however, when ultrasound suggests a substantial fatty component, clinicians should make an effort to obtain an MRI and provide appropriate management guidance. Whereas in large symptomatic lipoleiomyomas—such as cases requiring urgent intervention for severe hemorrhage—the presence of significant adipose tissue should prompt clinicians to consider lipoleiomyoma in the differential diagnosis whenever possible and to avoid excessive or overly aggressive treatment when this benign condition is likely.
Finally, recent advances in AI‐based image recognition may further improve the accuracy of preoperative diagnosis for lipoleiomyoma.
5. Limitation
Case reports often focus on unique cases or those involving specific treatments, underrepresenting cases that underwent conservative management or follow‐up; it remains unknown how many of the cases under follow‐up would eventually necessitate surgery.
6. Conclusion
Uterine lipoleiomyoma is a benign leiomyoma subtype that may exhibit hypertrophic growth, causing tumor enlargement, postmenopausal bleeding, and malignancy‐like symptoms. MRI is vital for accurate diagnosis. Treatment is generally unnecessary for asymptomatic cases, but surgical decisions depend primarily on lesion size and the facility′s MIS capabilities. Timely surgical intervention is crucial to prevent progression that could complicate surgery or recovery.
Funding
No funding was received for this manuscript.
Consent
No written consent has been obtained from the patients as there is no patient identifiable data included in this case report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Willén R. , Gad A. , and Willén H. , Lipomatous Lesions of the Uterus, Virchows Archiv. A, Pathological Anatomy and Histology. (1978) 377, no. 4, 351–361, 10.1007/BF 00507135, 2-s 2.0-0017853541.150107 · doi ↗ · pubmed ↗
- 2Swanson A. A. , Michal M. , Xing D. , Židlík V. , Cheek-Norgan E. H. , Keeney M. E. , Keeney G. L. , Sukov W. R. , Gupta S. , Nucci M. R. , and Schoolmeester J. K. , Benign Female Genital Tract Smooth Muscle Tumors With Adipocytic Differentiation: A Morphologic, Immunohistochemical and MDM 2 Fluorescence In Situ Hybridization Study of 44 Conventional Lipoleiomyomas and Lipoleiomyoma Variants, Human Pathology. (2023) 142, 51–61, 10.1016/j.humpath.2023.10.006, 37972871.37972871 · doi ↗ · pubmed ↗
- 3Akbulut M. , Gündoğan M. , and Yörükoğlu A. , Clinical and Pathological Features of Lipoleiomyoma of the Uterine Corpus: A Review of 76 Cases, Balkan Medical Journal. (2014) 31, no. 3, 224–229, 10.5152/balkanmedj.2014.13079, 2-s 2.0-84907265140, 25625021.25625021 PMC 4299967 · doi ↗ · pubmed ↗
- 4Lee S. , Chae H. , Jeong B. , Kwon S. K. , Kim S. H. , Kim C. H. , and Kang B. M. , A Clinical Review of Uterine Lipoleiomyoma: A Study for Value and Limitations of Radiologic Evaluation in Preoperative Diagnosis of Lipoleiomyoma, Korean Journal of Obstetrics & Gynecology. (2012) 55, no. 12, 953–957, 10.5468/KJOG.2012.55.12.953. · doi ↗
- 5Yuan Y. , Chen L. , Zhao T. , and Yu M. , Pathogenesis, Diagnosis and Treatment of Uterine Lipoleiomyoma: A Review, Biomedicine & Pharmacotherapy. (2021) 142, 112013, 10.1016/j.biopha.2021.112013, 34388526.34388526 · doi ↗ · pubmed ↗
- 6Ding D.-C. , Chu T. Y. , and Hsu Y. H. , Lipoleiomyoma of the Uterus, Taiwanese Journal of Obstetrics & Gynecology. (2010) 49, no. 1, 94–96, 10.1016/S 1028-4559(10)60018-6, 2-s 2.0-77953251233.20466302 · doi ↗ · pubmed ↗
- 7Oh S. R. , Cho Y. J. , Han M. , Bae J. W. , Park J. W. , and Rha S. H. , Uterine Lipoleiomyoma in Peri or Postmenopausal Women, Journal of Menopausal Medicine. (2015) 21, no. 3, 165–170, 10.6118/jmm.2015.21.3.165, 26793683.26793683 PMC 4719092 · doi ↗ · pubmed ↗
- 8Kim Y. S. and Lee J. H. , A Case Report of Pelviscopic Resection of Lipoleiomyoma Originating From the Uterine Cervix in a Postmenopausal Woman, Medicine. (2022) 101, no. 39, e 30665, 10.1097/MD.0000000000030665, 36181050.36181050 PMC 9524862 · doi ↗ · pubmed ↗