SCARCE: aSymptomatic respiratory viral Carriage in pre-lung transplant recipients and the effect on eArly-post lung tRansplant CoursE
Myrthe B. Bolt, Johanna P. van Gemert, Coretta van Leer-Buter, Erik A.M. Verschuuren

TL;DR
This study examines asymptomatic respiratory viral carriage in lung transplant recipients and finds no significant impact on early post-transplant outcomes.
Contribution
The study is the first to investigate asymptomatic respiratory viral carriage before lung transplantation and its effect on early outcomes.
Findings
10.4% of lung transplant recipients tested positive for asymptomatic respiratory viral carriage.
No significant differences in primary graft dysfunction or secondary outcomes were observed between CARV-positive and CARV-negative recipients.
Abstract
Asymptomatic community-acquired respiratory viral (CARV) carriage before lung transplantation (LTx) has not been studied. This study analyzed CARV carriage pre-LTx and its impact on early post-LTx outcome. This retrospective cohort study included adult LTx recipients at UMC Groningen from January 2017 to August 2023. Pre-LTx viral swabs were routinely tested for CARV. The primary outcome was incidence of primary graft dysfunction (PGD) at 48 or 72 h post-LTx. Secondary outcomes included mechanical ventilation duration, ICU stay, hospital length of stay (LOS), 30- and 90-day mortality, and early rejection therapy. Of 222 recipients, 23 (10.4%) tested positive for a CARV, most commonly rhinovirus (n=10). PGD grade 3 occurred in 14.3% of CARV-positive vs. 9.1% of CARV-negative recipients (p=0.434). No differences were observed in secondary outcomes. Our study provides early data suggesting…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
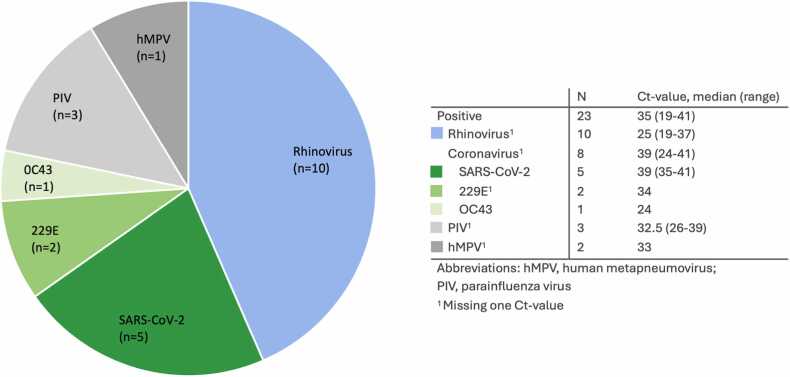 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Respiratory viral infections research · Viral Infections and Immunology Research
Introduction
Asymptomatic community-acquired respiratory viruses (CARV) carriage is quite common1, 2, 3 and might pose a risk to lung transplant (LTx) recipients in the early phase after lung transplantation due to high immunosuppression.2 CARV has been associated with chronic lung allograft dysfunction (CLAD),4, 5 however CARV at the time of LTx remain unexamined.
Primary graft dysfunction (PGD) occurs in up to 30% of cases within the first 3 days post-transplant, causing significant short- and long-term morbidity and mortality.6, 7 Furthermore, studies have suggested the role of a pro-inflammatory state in PGD development.6, 7 Yet, the relationship between PGD and asymptomatic CARV carriage at time of LTx, which might also cause an inflammatory state,8 remains unexplored. We studied if asymptomatic virus carriage leads to clinical disease during early immunosuppression.
Materials and methods
Population
This retrospective cohort study included all adult lung transplant recipients at the University Medical Center Groningen (UMCG), Netherlands, from January 2017 to August 2023. Since 2017, pre-LTx CARV swabs were routinely performed upon arrival for LTx and results usually became available post LTx. Data were collected from the UMCG LTx database and Electronic Patient Records. Recipients without CARV swab data were excluded. Included recipients were asymptomatic or previously infected without signs of active infection. At our center, a transplant team member contacts the patient at the time of a donor offer. If the patient shows symptoms of an exacerbation or infection, they are not admitted for transplantation. No antiviral treatment was given post-LTx in case of a positive swab. Immunosuppression included induction with Basiliximab, followed by Tacrolimus, Mycophenolate mofetil (MMF) and methylprednisolone. Immunosuppression was not modified based on CARV results.
Recipients provided written informed consent, and the study was approved by the UMCG Ethics Committee (CTc 18250).
Primary outcome was the incidence of PGD stage 3 at 48 h or 72 h post-LTx, categorized according to the International Society for Heart and Lung Transplantation (ISHLT) classification.6 Secondary outcomes included duration of post-LTX mechanical ventilation, intensive care unit (ICU) stay, hospital length of stay (LOS), 30-day and 90-day mortality rate, and incidence of acute rejection within 90 days post-LTx. During the first three months post-transplant, rejection is often diagnosed clinically. Therefore, data on specific type of rejection is not routinely available. Rejection therapy consisted of pulse methylprednisolone.
Statistical analysis
For quantitative outcomes, median and interquartile range (IQR) were used by swab result. Group differences were tested with the Mann-Whitney U test. For qualitative outcomes, frequencies and percentages were compared using Fisher’s exact or Chi-square test. A two-tailed p-value <0.05 was considered significant. Analyses were performed in SPSS23. Recipients who died within 72 h post-LTx were excluded from all outcomes except mortality. Logistic regression was performed to identify possible confounders.
Virology
Positive CARV was defined as positive polymerase chain reaction (PCR) of a respiratory sample for rhinovirus, respiratory syncytial virus (RSV), human metapneumovirus (hMPV), influenza virus, para-influenza virus (PIV), and coronaviruses including SARS-CoV-2 (COVID-19). Samples included nasopharyngeal swabs, nasal washes and sputum. PCR was tested as described before.9
Results
Of 243 recipients transplanted during the study period, 21 were excluded due to missing data. Of the 222 recipients, 23 (10.4%) had a positive pre-LTx CARV swab (Table 1 and Figure 1). Detected viruses included Rhinovirus (n=10), SARS-CoV-2 (n=5), Coronaviruses OC43/229E (n=3), PIV (n=3), and hMPV (n=2) (Figure 1). The median time from positive test until LTx was 10.9 h (IQR 4.7–14.8 h).Table 1. Recipient DemographicsTable 1All RecipientsPre-LTx CARV SwabTotalPositiveNegativep-valueRecipients22223199Sex, female (%)105 (47.3)7 (30.4)98 (49.2)0.087bAge, y (IQR)57.8 (50.1-62.2)58.0 (51.2-60.9)58.6 (51.9-62.7)0.424cUnderlying disease, n (%)0.747d Emphysema/ COPD116 (52.4)11 (47.8)105 (52.8) Cystic fibrosis9 (4.1)0 (0.0)9 (4.5) Pulmonary hypertension25 (11.3)2 (8.7)23 (11.6) Fibrosis56 (25.2)8 (34.8)48 (24.1) Graft-failure5 (2.3)1 (4.3)4 (2.0) Bronchiectasis3 (1.4)0 (0.0)3 (1.5) Othera8 (3.6)1 (4.3)7 (3.5)Transplant type, n (%)1.00d Single9 (4.1)1 (4.3)8 (4.0) Double212 (95.5)22 (95.7)190 (95.5) Lung-liver1 (0.5)0 (0.0)1 (0.5)Continuous data are displayed as medians with interquartile range (IQR)Abbreviations: COPD, chronic obstructive pulmonary disease.aOther underlying disease (histiocytosis, sarcoidosis, Stevens-Johnson syndrome, graft versus host disease, bronchiectasis, post-SARS-cov-2)bP-value from Chi-square testcP-value from Mann-Whitney U testdP-value from Fisher’s exactFigure 1CARV swab results.Figure 1
Overall, 9.6% (19/197) of recipients developed PGD grade 3 at 48 or 72 h. PGD grade 3 occurred in 14.3% (3/21) of CARV-positive and 9.1% (16/174) of CARV-negative recipients (p=0.434) (Table 2). There were no significant differences in duration of post transplant mechanical ventilation, ICU stay, total hospital LOS, 30-day mortality rate, occurrence of acute rejection (Table 2). Focusing on SARS-CoV-2, we saw a longer ventilation time, but no excess mortality. (Table 3). Two SARS-CoV-2–related cases were transplanted for COVID-induced lung fibrosis and were bridged with invasive ventilation.Table 2. Post-LTx OutcomesTable 2All RecipientsPre-LTx CARV SwabTotalPositiveNegativep-valueRecipients22223199PGD at 48 or 72 h n, (%)0.434a Grade 0-2Grade 3178 (90.4)19 (9.6)18 (85.7)3 (14.3)160 (90.9)16 (9.1)Duration mechanical ventilation, days (IQR)1 (1-5)2 (1-13)1 (1-4)0.318bICU stay, days (IQR)5 (3-13)12 (2-26)5 (3-11)0.434bHospital LOS, days (IQR)33 (23-50)37 (29-65)32 (23-49)0.216bRejection therapy used^,^ n (%)91 (41.0)8 (34.8)83 (41.7)0.656c30-day mortality, n (%)11 (5.0)0 (0.0)11 (5.5)0.610a90-day mortality, n (%)20 (9.0)0 (0.0)20 (10.1)0.238aContinuous data are displayed as medians with interquartile range (IQR)Abbreviations: ICU, intensive care unit; LOS, length of stay; PGD, primary graft dysfunction.aP-value from Fisher’s exactbP-value from Mann-Whitney U testcP-value from Chi-square testdRejection therapy included methylprednisolone.Table 3. Post-hoc Analysis of COVID-19 and Post-LTx OutcomesTable 3All RecipientsPre-LTx CARV SwabTotalCOVID-19Negativep-valueRecipients2045199PGD at 48 or 72 h n, (%)0.3931 Grade 0-2Grade 3164 (90.6)17 (9.4)4 (80.0)1 (20.0)160 (90.9)16 (9.1)Duration mechanical ventilation, days (IQR)1 (1-5)8 (5.5-14)1 (1-4)0.0082ICU stay, days (IQR)5 (3-12.5)15 (11-33.5)5 (3-11)0.0222Hospital LOS, days (IQR)32 (23-48.5)42 (25-61.5)32 (23-49)0.6202Rejection therapy use3, n (%)85 (41.7)2 (40.0)83 (41.7)1.00130-day mortality, n (%)11 (5.0)0 (0.0)11 (5.5)1.00190-day mortality, n (%)20 (9.0)0 (0.0)20 (10.1)1.001Continuous data are displayed as medians with interquartile range (IQR)Abbreviations: ICU, intensive care unit; LOS, length of stay; PGD, primary graft dysfunction.1P-value from Fisher’s exact2P-value from Mann-Whitney U test3Rejection therapy included methylprednisolone.
In multivariate analysis, male sex was associated with lower risk for PGD (OR 0.25, 95% CI 0.08–0.72, p=0.011), whereas CARV positivity showed no higher risk (OR 2.08, 95% CI 0.52–8.24, p=0.298) (Table 4).Table 4. Univariate and Multivariate Regression AnalysisTable 4Univariate OR (95% CI)p-valueMultivariate OR (95% CI)p-valueSex0.26 (0.09–0.75)0.0130.25 (0.08–0.72)0.011Age0.98 (0.94–1.02)0.263--Underlying disease1.19 (0.92–1.53)0.186--Transplant type1 (double vs other)1.01 (0.05–19.8)0.998--CARV positive1.67 (0.44-6.28)0.4502.08 (0.52-8.24)0.298Abbreviations: OR, odds ratio; CI, confidence interval1Due to small numbers in this category, analysis was performed using ‘Double’ versus ‘Other’ transplants.
Discussion
This study shows that pre-LTx CARV carriage is common (10.4%) among asymptomatic LTx candidates. Our findings suggest that asymptomatic CARV carriage does not impact early outcomes, however the limited sample size restricts firm conclusions.
Our CARV detection rate is slightly higher than rates among ambulatory adults in New York (4.3–6%), which is likely due to increased susceptibility in pre-LTx recipients with underlying lung disease.10 Moreover, our study aligns with asymptomatic CARV rates reported among LTx recipients on average 3–4 years after LTx.3, 11 Rhinovirus was most frequently detected (43%) in our study cohort, consistent with prior studies.1, 3, 11, 12
Thus far, studies have shown that symptomatic infections are linked to adverse outcomes such as CLAD or graft loss, while asymptomatic infections do not.3, 5 Our findings are consistent with this and expand on the early post-LTx period. Similarly, a study analyzing CARV in bronchoscopy samples one day post-LTx found no association with PGD.12 This likely reflects donor-derived rather than recipient-derived CARV, given the lower respiratory tract sampling. In contrast, our study focused exclusively on recipient-derived CARV.
In our study, all of our recipients were asymptomatic upon arrival for LTx despite a positive swab. This may be because respiratory symptoms may be masked in patients with end-stage lung disease. Alternatively, viral RNA can be obtained at any point during infection, encompassing recipients recovering from a CARV, who continue to shed the virus post-infection, a phenomenon well-documented in COVID-19 cases.8 This could explain the high Ct values, reflecting minimal viral loads, however some recipients had higher loads.
Among the five SARS-CoV-2–positive recipients, two were transplanted due to COVID-induced lung fibroses and were bridged with invasive ventilation pre-transplant, possibly contributing to longer post-transplantation ventilation. Post hoc analysis showed no increase in mortality or hospital LOS.
This study’s retrospective design and small sample size are important limitations. We could not stratify outcomes by virus type or viral load, and seasonal trends were not assessed. The broad time frame (2017–2023) spans the COVID-19 pandemic, when respiratory virus circulation patterns were disrupted. Non-COVID CARVs were virtually undetected early in the pandemic, likely underestimating asymptomatic CARV carriage among our cohort. Furthermore, follow-up swabs were not routinely obtained post-LTx, limiting our understanding of viral clearance or recurrences. However, there was no clinical suspicion of CARV post-LTx in these recipients.
Although treating detected CARV peri-transplant may seem intuitive, treatment options are limited for most CARV. Our study aimed to assess whether these CARV posed an unrecognized clinical issue rather than to guide antiviral therapy, making this an initial exploration of their peri-transplant relevance.
In conclusion, this study provides early data on pre-LTx asymptomatic CARV carriage, suggesting asymptomatic carriage is not associated with worse short-term outcomes. Importantly, our results show no reason to cancel a LTx due to asymptomatic CARV positivity. Overall, we believe routine testing of asymptomatic LTx candidates for CARV offers limited added value.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Generative AI and AI-assisted technologies in the writing process
During the preparation of this work the author(s) used ChatGPT during the writing process in order to improve the readability and language of the manuscript. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the published article.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tomlinson R.H.Harrison L.G.Meals E.A.De Vincenzo J.P.Do asymptomatic respiratory viral infections occur?J Clin Virol 1022018939410.1016/j.jcv.2018.03.00229529485 PMC 7128593 · doi ↗ · pubmed ↗
- 2Munting A.Manuel O.Viral infections in lung transplantation J Thorac Dis 131120216673669410.21037/jtd-2021-2434992844 PMC 8662465 · doi ↗ · pubmed ↗
- 3Bridevaux P.O.Aubert J.D.Soccal P.M.Incidence and outcomes of respiratory viral infections in lung transplant recipients: a prospective study Thorax 6912014323810.1136/thoraxjnl-2013-20358124025442 · doi ↗ · pubmed ↗
- 4de Zwart A.Riezebos-Brilman A.Lunter G.Respiratory syncytial virus, human metapneumovirus, and parainfluenza virus infections in lung transplant recipients: a systematic review of outcomes and treatment strategies Clin Infect Dis 741220222252226010.1093/cid/ciab 96935022697 PMC 9258934 · doi ↗ · pubmed ↗
- 5Allyn P.R.Duffy E.L.Humphries R.M.Graft loss and CLAD-onset is hastened by viral pneumonia after lung transplantation Transplantation 1001120162424243110.1097/TP.000000000000134627467538 PMC 5077663 · doi ↗ · pubmed ↗
- 6Morrison M.I.Pither T.L.Fisher A.J.Pathophysiology and classification of primary graft dysfunction after lung transplantation J Thorac Dis 91020174084409710.21037/jtd.2017.09.0929268419 PMC 5723840 · doi ↗ · pubmed ↗
- 7Van Slambrouck J.Van Raemdonck D.Vos R.A focused review on primary graft dysfunction after clinical lung transplantation: a multilevel syndrome Cells 114202274510.3390/cells 1104074535203392 PMC 8870290 · doi ↗ · pubmed ↗
- 8Boyton R.J.Altmann D.M.The immunology of asymptomatic SARS-Co V-2 infection: what are the key questions?Nat Rev Immunol 2112202176276810.1038/s 41577-021-00631-x 34667307 PMC 8525456 · doi ↗ · pubmed ↗