Animal naming test at discharge is associated with hepatic encephalopathy after elective TIPS
Melisande Jorus, Philippe Sultanik, Charlotte Bouzbib, Sarah Mouri, Lyes Kheloufi, Maxime Gasperment, Nicolas Weiss, Charles Roux, Dominique Thabut, Marika Rudler

TL;DR
The animal naming test at discharge helps predict the risk of brain-related complications after a liver procedure called TIPS.
Contribution
The study shows that the animal naming test at discharge, not before TIPS, is a novel predictor of overt hepatic encephalopathy.
Findings
ANT at discharge was an independent predictor of OHE with an 8% increased risk per 1-point decrease.
Pre-TIPS ANT was not predictive of OHE, but post-TIPS ammonia levels and ANT were.
The cumulative incidence of OHE was 30% after elective TIPS placement.
Abstract
Overt hepatic encephalopathy (OHE) is the most feared complication after transjugular intrahepatic portosystemic shunt (TIPS) placement. We aimed to evaluate the usefulness of the animal naming test (ANT) in predicting the occurrence of OHE after elective TIPS placement. The ANT (1 min) was evaluated before TIPS, at discharge, and at 1, 3, and 6 months in all patients treated with elective TIPS between September 2019 and November 2024. We included 100 consecutive patients (80% men; median age 59 years; median MELD score 11). Indications for TIPS were ascites, secondary prophylaxis, hydrothorax, and pre-surgery in 63%, 19%, 5%, 13%, respectively; 24% had a history of OHE. The median ANT before TIPS was 21 (IQR 17–27). The cumulative incidence of OHE was 30%, considering death and liver transplantation as competing events. In multivariate analysis, independent predictors of OHE…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
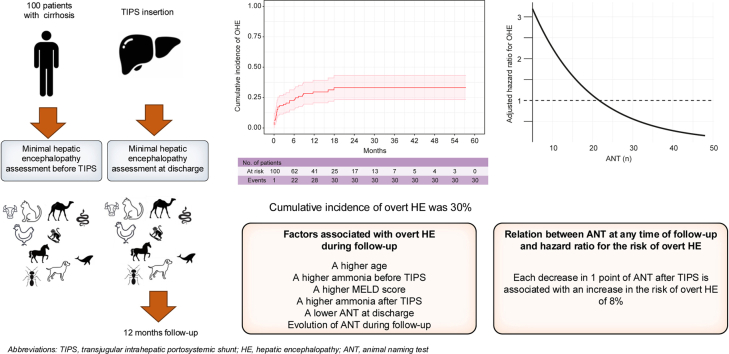 Figure 1
Figure 1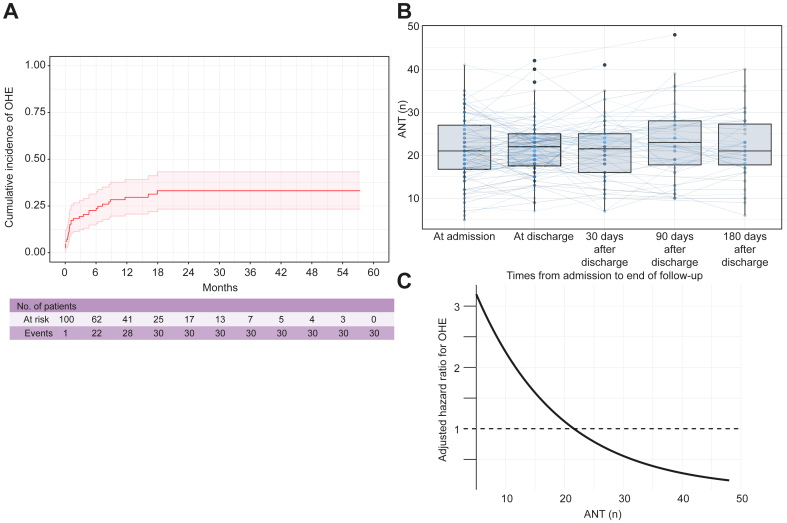 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease and Transplantation · Liver Disease Diagnosis and Treatment · Organ Transplantation Techniques and Outcomes
Introduction
Overt hepatic encephalopathy (OHE) is a significant concern following elective transjugular intrahepatic portosystemic shunt (TIPS) procedures, with studies reporting incidence rates between 30% and 50%, influenced by patient characteristics and the indication for TIPS placement.[1], [2], [3], [4], [5], [6] The impact of OHE on prognosis after TIPS remains a subject of debate. While some studies suggest a negative influence,6 others involving a large cohort of over 600 patients indicated that episodic OHE did not elevate mortality risk after elective TIPS.5 The timing of OHE onset may also be a factor, with some studies suggesting that early OHE after TIPS could be particularly detrimental.7
Predicting neurological outcomes in patients with cirrhosis before elective TIPS is challenging,8 but several risk factors for OHE have been identified. These include age, minimal HE (MHE), sarcopenia, a lower portal pressure gradient post-TIPS, renal dysfunction, and hyponatremia, all of which have been associated with a higher likelihood of OHE.6^,^[9], [10], [11], [12] Careful patient selection based on individual risk factor assessment, combined with rifaximin prophylaxis in elective settings, represents the most effective approach to preventing OHE after elective TIPS.13^,^14 The impact of MHE is controversial; some studies show good predictive value for tools such as critical flicker frequency,12 whereas others fail to demonstrate any additional predictive value of three tests of MHE before TIPS, including the animal naming test (ANT), the psychometric hepatic encephalopathy score, and the critical flicker frequency.15 More recently, one study provided evidence that ammonia levels measured early after TIPS insertion (and before discharge) are an excellent and readily available biomarker for identifying patients at high risk for post-TIPS OHE,16 suggesting that the very early consequences of TIPS, more than the baseline characteristics of patients before TIPS, are important in the pathogenesis of post-TIPS OHE. Thus, in this study, we aimed to evaluate whether ANT measured before TIPS and within the first days after elective TIPS could identify patients at high risk of OHE.
Materials and methods
This is a retrospective study using a prospective cohort of patients treated with TIPS and hospitalized in the Department of Hepatology at La Pitié-Salpêtrière Hospital, Paris, France. This cohort was approved by the research ethics committee of Sorbonne University (CER-2022-074). All consecutive patients treated with TIPS who were hospitalized between September 2019 and September 2024 were screened for inclusion after their non-opposition was recorded in a prospective database. Inclusion criteria were: patients with cirrhosis (previously known or newly diagnosed during hospitalization, confirmed histologically or based on clinical or radiological criteria); elective TIPS placement; and TIPS indications including refractory or recurrent ascites, failure of secondary prophylaxis for acute variceal bleeding, or preoperative management. Exclusion criteria were: age <18; previous liver transplantation (LT); or emergency TIPS (salvage, rescue, or preemptive). ANT was evaluated on the day of TIPS placement, at discharge, and at 1, 3, and 6 months after TIPS insertion during scheduled follow-up visits. Information on the TIPS insertion procedure, follow-up (including clinical evaluation, testing for ANT and OHE, and biological data), and statistics are provided in the supplementary methods. Regarding the use of lactulose or rifaximin as primary or secondary prophylaxis, we applied the following strategy: before the publication of Bureau et al.’s study,13 all patients with a previous episode of OHE received lactulose as secondary prophylaxis. After the publication of Bureau et al.’s study,13 all patients with a previous episode of OHE received lactulose as secondary prophylaxis plus rifaximin, starting 15 days before TIPS and continuing for 6 months after TIPS. Also, after Bureau et al.’s study,13 all patients without a previous episode of OHE received rifaximin, starting 15 days before TIPS and continuing for 6 months after TIPS. During the study period, 270 patients received a TIPS, and 100 patients met the inclusion criteria.
Results
Baseline characteristics of the patients are provided in Table S1, for the whole cohort, and according to the predefined cut-off value of ANT of 20/minute for MHE in France. Patients with an ANT <20/min on the day of TIPS placement were significantly older (62 vs. 58 years, p = 0.01) and had poorer liver function, as assessed by Child-Pugh (8 vs. 7, p <0.001) or MELD (12 vs. 10, p = 0.04) score. They were more frequently treated with lactulose before TIPS (51 vs. 26%, p = 0.02). The median duration of hospitalization was 3.5 days, and only 13 patients were discharged more than 7 days after TIPS. During a median follow-up of 364 days (IQR 54–754 days), 30 patients (30%) developed an OHE episode, and 26 patients (26%) died or were transplanted. Fig. 1A displays the cumulative incidence of OHE (considering LT and death as competing risks) after TIPS. Univariable and multivariable analyses of factors associated with subsequent development of OHE are provided in Table S2A and B: older age (subdistribution hazard ratio [sHR] 1.05; 95% CI 1.00–1.10; p = 0.048), a higher baseline ammonia level before TIPS (sHR 1.01; 95% CI 1.01–1.01; p <0.001), a lower ANT at discharge (sHR 0.91; 95% CI 0.83–0.99; p = 0.032), and a higher ammonia level at discharge (sHR 1.02; 95% CI 1.01–1.03; p = 0.04) were independently associated with OHE after TIPS, but not ANT on the day of TIPS placement (sHR 0.96; 95% CI 0.90–1.03; p = 0.06). The evolution of ANT between the day of TIPS, discharge, and 1, 3, and 6 months after TIPS is provided in Fig. 1B. The relation between ANT at any time after TIPS placement and the HR of post-TIPS OHE is shown in Fig. 1C. A proportionality test revealed that the prognostic value of post-TIPS ANT was stable over time. Each decrease of ANT of 1 point was associated with an increased risk of OHE of 8%.Fig. 1. Association between ANT performance and the risk of OHE after TIPS.(A) Cumulative incidence of OHE after TIPS. The cumulative incidence of OHE (considering LT and death as competing risks) was 30%. (B) Trajectory of ANT before TIPS and at discharge, 1, 3 and 6 months after TIPS insertion. (C) Relation between ANT at any time of follow-up and hazard ratio for the risk of OHE. Each decrease in ANT of 1 point after TIPS is associated with an increase in the risk of OHE of 8%. ANT, animal naming test; OHE, overt hepatic encephalopathy; TIPS, transjugular intrahepatic portosystemic shunt.Fig. 1
Cumulative mortality (LT as a competing event) was 26% at 1 year after TIPS. ANT, before or at each time point after TIPS, was never associated with a higher risk of death or LT (HR 0.92; 95% CI 0.82-1.03; p = 0.13).
Discussion
In this study, we confirm that ANT, evaluated before elective TIPS placement, is not associated with subsequent development of OHE. However, we suggest for the first time that assessment of this test at discharge – which varied among patients but occurred a median of 3.5 days after elective TIPS placement in our study – may be a useful tool for predicting OHE. Second, ammonia levels before TIPS could be a good biomarker for identifying patients at risk of OHE after TIPS. Recent studies have demonstrated the prognostic value of ammonia, both in outpatients (predicting hospitalization, OHE, and death)17 and in patients hospitalized for acute decompensation (predicting acute-on-chronic liver failure and death).18 Our team also conducted a recent study comparing the prevalence and risk factors of OHE after elective or preemptive TIPS and found that baseline ammonia was an independent factor associated with OHE after elective but not after preemptive TIPS, although baseline ammonia was significantly higher in the preemptive TIPS group.19 In a recent report by Labenz et al.,16 ammonia measured after TIPS insertion was found to be useful for identifying patients at risk for OHE. The authors hypothesized that if ammonia homeostasis is dramatically changed by TIPS insertion, the severity of the change in ammonia metabolism is not predictable. Our results align with these findings, suggesting that early changes after TIPS (in ANT or ammonia levels) may have an early impact on brain function, act as an initial cerebral insult, and contribute to early cognitive impairment detected by ANT after TIPS, which is predictive of OHE. Interestingly, both ANT and ammonia are linked to further OHE, suggesting that the ANT might be sensitive to changes in ammonia levels and to causes of neurocognitive impairment other than covert HE, as previously described in outpatients with cirrhosis and cognitive complaints.20
In conclusion, our study provides evidence that ANT assessed at discharge may help identify patients at high risk of post-TIPS OHE. This easily obtainable measure could contribute to more tailored management of high-risk patients from a neurological perspective, such as intensified surveillance and treatment based on discharge ANT, avoidance of additional cerebral risk factors, patient education, and early consideration of shunt reduction and/or LT.
Abbreviations
ANT, animal naming test; LT, liver transplantation; MELD, model for end stage liver disease; MHE, minimal hepatic encephalopathy; OHE, overt hepatic encephalopathy; TIPS, transjugular intrahepatic portosystemic shunt.
Authors’ contributions
Melisande Jorus: collecting data, analysis and interpretation of data, drafting the manuscript. Philippe Sultanik: statistical analysis, critical review of the manuscript. Charlotte Bouzbib: management of patients, collecting data critical review of manuscript. Sarah Mouri: management of patients, collecting data critical review of manuscript. Lyes Kheloufi: critical review of manuscript. Nicolas Weiss: critical review of manuscript. Dominique Thabut: study design, management of patients, critical review of manuscript. Marika Rudler: study design, management of patients, analysis and interpretation of data, drafting the manuscript, critical review of manuscript.
Data availability
Data available on justified request.
Financial support
No financial support was received to produce this manuscript.
Conflict of interest
The authors declare no conflicts of interest pertaining to this manuscript.
Please refer to the accompanying ICMJE disclosure forms for further details.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rudler M.Hernández-Gea V.Procopet B.D.For International Variceal Bleeding Observational Study Group: a Baveno Cooperation. Hepatic encephalopathy is not a contraindication to pre-emptive TIPS in high-risk patients with cirrhosis with variceal bleeding Gut 7242023 Apr 7497583632877210.1136/gutjnl-2022-326975 · doi ↗ · pubmed ↗
- 2Bouzbib C.Cluzel P.Sultanik P.Prognosis of patients undergoing salvage TIPS is still poor in the preemptive TIPS era Clin Res Hepatol Gastroenterol 4562021 Nov 10159310.1016/j.clinre.2020.10159333667917 · doi ↗ · pubmed ↗
- 3Walter A.Rudler M.Olivas P.Salvage TIPS Group Combination of model for end-stage liver disease and lactate predicts death in patients treated with salvage transjugular intrahepatic portosystemic shunt for refractory variceal bleeding Hepatology 7442021 Oct 208521013401862710.1002/hep.31913 · doi ↗ · pubmed ↗
- 4Bureau C.Thabut D.Oberti F.Transjugular intrahepatic portosystemic shunts with covered stents increase transplant-free survival of patients with cirrhosis and recurrent ascites Gastroenterology 15212017 Jan 1571632017 Sep;153(3):8702766360410.1053/j.gastro.2016.09.016 · doi ↗ · pubmed ↗
- 5Nardelli S.Riggio O.Marra F.Episodic overt hepatic encephalopathy after transjugular intrahepatic portosystemic shunt does not increase mortality in patients with cirrhosis J Hepatol 8042024 Apr 5966023809711310.1016/j.jhep.2023.11.033 · doi ↗ · pubmed ↗
- 6Bai M.Qi X.Yang Z.Predictors of hepatic encephalopathy after transjugular intrahepatic portosystemic shunt in cirrhotic patients: a systematic review J Gastroenterol Hepatol 2662011 Jun 9439512125106710.1111/j.1440-1746.2011.06663.x · doi ↗ · pubmed ↗
- 7Hartl L.Kornfehl A.Reiberger T.Does encephalopathy with early onset after TIPS impact on mortality?J Hepatol 8162024 Dece 269e 2703883895810.1016/j.jhep.2024.05.035 · doi ↗ · pubmed ↗
- 8Rudler M.Weiss N.Perlbarg V.Combined diffusion tensor imaging and magnetic resonance spectroscopy to predict neurological outcome before transjugular intrahepatic portosystemic shunt Aliment Pharmacol Ther 4882018 Oct 8638743017887010.1111/apt.14938 · doi ↗ · pubmed ↗