Thrombocytopenia and Bleeding in Patients With Oncologic Emergencies Following Cancer Therapy
Le Tian, Jia‐Xin Huang, Xi Zhang, Ning Li, Zhi‐Min Bian, Na Li, Shao‐Ming Wang, Xin‐Qi Liu, Zhi‐Yong Li, Qing‐Long Jiang, Chao Wang, Cong Zhao, Wei Wei, Ming‐Hua Cong

TL;DR
This study examines cancer therapy-induced thrombocytopenia in emergency oncology patients, identifying risk factors for bleeding and highlighting the need for clinical vigilance.
Contribution
The study provides new insights into CTIT and its risk factors for bleeding in Chinese emergency oncology patients.
Findings
13.5% of 8590 emergency oncology cases had CTIT, with 5.24% experiencing overt organ hemorrhage.
Fever and pleural effusion were identified as independent risk factors for CTIT-related bleeding.
Lung cancer was the most common malignancy in CTIT cases with bleeding.
Abstract
There is a lack of studies investigating Cancer therapy‐induced thrombocytopenia (CTIT) and the risk factors predicting CTIT‐related hemorrhage in the emergency oncology patient population. This study aimed to present Chinese data on CTIT and organ bleeding in patients undergoing emergency oncology. This retrospective study was conducted in the Oncology Emergency Department. We evaluated the clinical features and outcomes of CTIT and associated organ hemorrhage. A retrospective analysis collected data from 8590 cases of malignant tumor emergency visits. Among these, 1164 cases (13.5%) of CTIT met the inclusion criteria, with a median patient age of 61 years. 61 (5.24%) of the 1164 CTIT cases were associated with overt organ hemorrhage. Independent risk factors predicting CTIT deterioration included Eastern Cooperative Oncology Group (ECOG) score of 2–4 (odds ratio [OR] = 4.883), stage…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
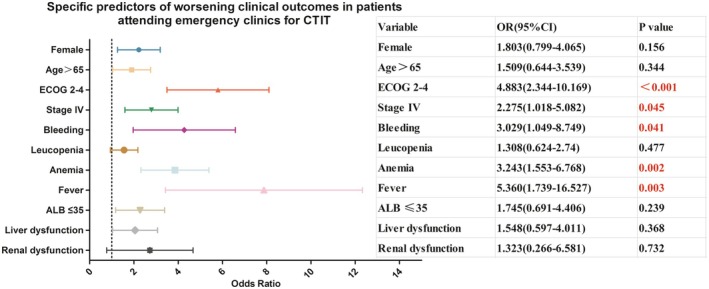 FIGURE 1
FIGURE 1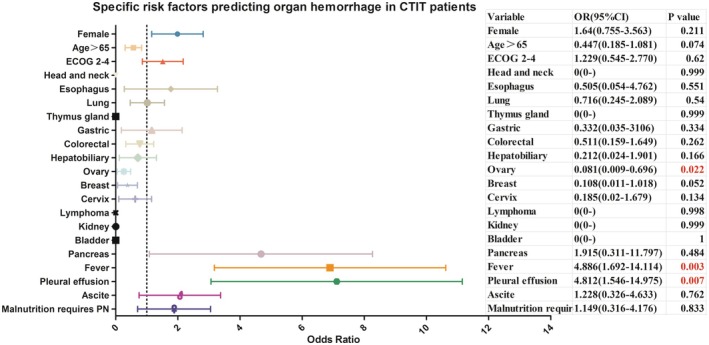 FIGURE 2
FIGURE 2| Variable | Total (%) | Bleeding (%) | Non‐bleeding (%) | χ2 |
| |
|---|---|---|---|---|---|---|
| Sex | Male | 593 (50.9) | 31 (50.8) | 562 (51) | 0.000 | 0.984 |
| Female | 571 (49.1) | 30 (49.2) | 541 (49) | |||
| Year | ≤ 65 | 797 (68.5) | 46 (75.4) | 751 (68.1) | 1.436 | 0.231 |
| > 65 | 367 (31.5) | 15 (24.6) | 352 (31.9) | |||
| ECOG | 0–1 | 923 (79.3) | 48 (78.7) | 875 (79.3) | 0.014 | 0.904 |
| 2–4 | 241 (20.7) | 13 (21.3) | 228 (20.7) | |||
| Tumor site | 30.153 | 0.007 | ||||
| Head and neck | 16 (1.4) | 0 (0) | 16 (1.5) | 0.897 | 1.000 | |
| Esophagus | 47 (4.1) | 1 (1.6) | 46 (4.2) | 0.956 | 0.509 | |
| Lung | 399 (34.5) | 25 (41.0) | 374 (34.2) | 1.285 | 0.257 | |
| Thymus gland | 11 (1) | 0 (0) | 11 (1.0) | 0.614 | 1.000 | |
| Gastric | 86 (7.4) | 5 (8.2) | 81 (7.4) | 0.061 | 0.800 | |
| Colorectal | 156 (13.5) | 9 (14.8) | 147 (13.4) | 0.101 | 0.750 | |
| Hepatobiliary | 66 (5.7) | 1 (1.6) | 65 (5.9) | 1.955 | 0.251 | |
| Ovary | 118 (10.2) | 3 (4.9) | 115 (10.5) | 1.925 | 0.165 | |
| Breast | 67 (5.8) | 1 (1.6) | 66 (6.0) | 2.011 | 0.253 | |
| Cervix | 48 (4.2) | 2 (3.3) | 46 (4.2) | 0.116 | 1.000 | |
| Lymphoma | 46 (4.0) | 0 (0) | 46 (4.2) | 2.649 | 0.168 | |
| Kidney | 2 (0.2) | 0 (0) | 2 (0.2) | 0.111 | 1.000 | |
| Bladder | 1 (0.1) | 0 (0) | 1 (0.1) | 0.055 | 1.000 | |
| Pancreas | 17 (1.5) | 3 (4.9) | 14 (1.3) | 5.347 | 0.055 | |
| Other or unknown primary | 75 (6.5) | 11 (18) | 64 (5.9) | 14.343 | 0.001 | |
| Pathological classification | Adenocarcinoma | 530 (62.3) | 37 (71.2) | 493 (61.7) | 4.932 | 0.424 |
| Squamous carcinoma | 118 (13.9) | 5 (9.6) | 113 (14.1) | |||
| Small cell | 87 (10.2) | 7 (13.5) | 80 (10.0) | |||
| Sarcoma | 3 (0.4) | 0 (0) | 3 (0.4) | |||
| Lymphoma | 25 (2.9) | 0 (0) | 25 (3.1) | |||
| Other | 88 (10.3) | 3 (5.8) | 85 (10.6) | |||
| Stage | I‐III | 82 (7.0) | 4 (6.6) | 78 (7.1) | 0.049 | 0.976 |
| IV | 333 (28.6) | 17 (27.9) | 316 (28.6) | |||
| Tumor control | CR/PR | 2 (0.2) | 0 (0) | 2 (0.2) | 0.246 | 0.884 |
| SD | 610 (66.8) | 35 (64.8) | 575 (66.9) | |||
| PD | 301 (33.0) | 19 (35.2) | 282 (32.8) | |||
| Chemotherapy | Yes | 1124 (96.6) | 59 (96.7) | 1065 (96.6) | 0.005 | 0.945 |
| No | 40 (3.4) | 2 (3.3) | 38 (3.4) | |||
| Radiotherapy | Yes | 49 (4.2) | 2 (3.3) | 47 (4.3) | 0.138 | 0.710 |
| No | 1115 (95.8) | 59 (96.7) | 1056 (95.7) | |||
| Immunotherapy | Yes | 97 (8.3) | 5 (8.2) | 92 (8.3) | 0.002 | 0.968 |
| No | 1067 (91.7) | 56 (91.8) | 1011 (91.7) | |||
| Target therapy | Yes | 66 (5.7) | 6 (9.8) | 60 (5.4) | 2.089 | 0.148 |
| No | 1098 (94.3) | 55 (90.2) | 1043 (94.6) | |||
| Fever | Yes | 39 (3.4) | 7 (11.5) | 32 (2.9) | 13.123 | < 0.001 |
| No | 1125 (96.6) | 54 (88.5) | 1071 (97.1) | |||
| Liver dysfunction | Yes | 149 (12.8) | 9 (14.8) | 140 (12.7) | 0.220 | 0.639 |
| No | 1015 (87.2) | 52 (85.2) | 963 (87.7) | |||
| Renal dysfunction | Cr > 97 | 35 (3.0) | 2 (3.3) | 33 (3.0) | 0.016 | 0.898 |
| Cr ≤ 97 | 1129 (97) | 59 (96.7) | 1070 (97) | |||
| Malignant plasmapheresis | Pleural effusion | 32 (4.5) | 5 (11.4) | 27 (4.0) | 9.954 | 0.007 |
| Ascite | 45 (6.3) | 6 (13.6) | 39 (5.8) | |||
| No | 635 (89.2) | 33 (75) | 602 (90.1) | |||
| ALB (g/L) | ≤ 35 | 108 (9.3) | 8 (13.1) | 100 (9.1) | 1.126 | 0.289 |
| > 35 | 1056 (90.7) | 53 (86.9) | 1003 (90.9) | |||
| Malnutrition requires PN | Yes | 37 (3.2) | 6 (9.8) | 31 (2.8) | 9.270 | 0.002 |
| No | 1127 (96.8) | 55 (90.2) | 1072 (97.2) | |||
| Anemia | Yes | 186 (16.0) | 12 (19.7) | 174 (15.8) | 0.654 | 0.419 |
| No | 978 (84.0) | 49 (80.3) | 929 (84.2) | |||
| Leucopenia | Yes | 684 (58.8) | 37 (60.7) | 647 (58.7) | 0.095 | 0.758 |
| No | 480 (41.2) | 24 (39.3) | 456 (41.3) | |||
| Raise PLT strategy | Rh‐TPO | 852 (73.2) | 45 (73.8) | 807 (73.2) | 40.292 | < 0.001 |
| TPO‐RA | 13 (1.1) | 1 (1.6) | 12 (1.1) | |||
| Rh‐TPO+ TPO‐RA | 82 (7.0) | 15 (24.6) | 67 (6.1) | |||
| IL‐11 | 24 (2.1) | 0 (0) | 24 (2.2) | |||
| Observation | 193 (16.6) | 0 (0) | 193 (17.5) | |||
| Fact | Improvement (%) | Worse (%) | Hospitalization (%) | χ2 |
|
|---|---|---|---|---|---|
| Total | 1126 (96.7) | 29 (2.5) | 9 (0.8) | ||
| Sex | 5.08 | 0.079 | |||
| Male | 580 (97.8) | 11 (1.9) | 2 (0.3) | ||
| Female | 546 (95.6) | 18 (3.2) | 7 (1.2) | ||
| Age | 0.703 | 0.704 | |||
| ≤ 65 | 772 (96.9) | 20 (2.5) | 5 (0.6) | ||
| > 65 | 354 (96.5) | 9 (2.5) | 4 (1.1) | ||
| ECOG | 33.133 | < 0.001 | |||
| 0–1 | 907 (98.3) | 12 (1.3) | 4 (0.4) | ||
| 2–4 | 219 (90.9) | 17 (7.1) | 5 (2.1) | ||
| Stage | 22.065 | < 0.001 | |||
| I‐III | 79 (96.3) | 0 (0) | 3 (3.7) | ||
| IV | 314 (94.3) | 14 (4.2) | 5 (1.5) | ||
| unknown | 733 (97.9) | 15 (2.0) | 1 (0.1) | ||
| Tumor control | 3.239 | 0.519 | |||
| CR/PR | 2 (100) | 0 (0) | 0 (0) | ||
| SD | 589 (96.6) | 15 (2.5) | 6 (1.0) | ||
| PD | 284 (94.4) | 14 (4.7) | 3 (1.0) | ||
| Bleeding | 14.723 | 0.001 | |||
| Yes | 55 (90.2) | 6 (9.8) | 0 (0) | ||
| No | 1071 (97.1) | 23 (2.1) | 9 (0.8) | ||
| Leucopenia | 3.018 | 0.221 | |||
| Yes | 659 (96.3) | 21 (3.1) | 4 (0.6) | ||
| No | 467 (97.3) | 8 (1.7) | 5 (1.0) | ||
| Anemia | 18.764 | < 0.01 | |||
| Yes | 171 (91.9) | 13 (7.0) | 2 (1.1) | ||
| No | 955 (97.6) | 16 (1.6) | 7 (0.7) | ||
| Liver dysfunction | 2.948 | 0.229 | |||
| Yes | 143 (96.0) | 6 (4.0) | 0 (0) | ||
| No | 983 (96.8) | 23 (2.3) | 9 (0.9) | ||
| Renal dysfunction | 11.519 | 0.003 | |||
| Yes | 32 (91.4) | 1 (2.9) | 2 (5.7) | ||
| No | 1094 (96.9) | 28 (2.5) | 7 (0.6) | ||
| Fever | 29.497 | < 0.001 | |||
| Yes | 32 (82.1) | 6 (15.4) | 1 (2.6) | ||
| No | 1094 (97.2) | 23 (2.0) | 8 (0.7) | ||
| ALB (g/L) | 13.781 | 0.001 | |||
| ≤ 35 | 98 (90.7) | 8 (7.4) | 2 (1.9) | ||
| > 35 | 1028 (97.3) | 21 (2.0) | 7 (0.7) |
| Factor | Multivariate | |
|---|---|---|
| OR (95% CI) |
| |
| Sex | ||
| Male | Reference | |
| Female | 1.803 (0.799–4.065) | 0.156 |
| Age | ||
| ≤ 65 | Reference | |
| > 65 | 1.509 (0.644–3.539) | 0.344 |
| ECOG | ||
| 0–1 | Reference | |
| 2–4 | 4.883 (2.344–10.169) | < 0.001 |
| Stage | ||
| I‐III | Reference | |
| IV | 2.275 (1.018–5.082) | 0.045 |
| unknown | 2.236 (0.596–8.395) | 0.233 |
| Bleeding | ||
| Yes | 3.029 (1.049–8.749) | 0.041 |
| No | Reference | |
| Leucopenia | ||
| Yes | 1.308 (0.624–2.74) | 0.477 |
| No | Reference | |
| Anemia | ||
| Yes | 3.243 (1.553–6.768) | 0.002 |
| No | Reference | |
| Fever | ||
| Yes | 5.360 (1.739–16.527) | 0.003 |
| No | Reference | |
| ALB (g/L) | ||
| ≤ 35 | 1.745 (0.691–4.406) | 0.239 |
| > 35 | Reference | |
| Liver dysfunction | ||
| Yes | 1.548 (0.597–4.011) | 0.368 |
| No | Reference | |
| Renal dysfunction | ||
| Yes | 1.323 (0.266–6.581) | 0.732 |
| No | Reference | |
| Factor | Univariate | Multivariate | |||
|---|---|---|---|---|---|
| OR (95% CI) |
| OR (95% CI) |
| ||
| Gender | Male | Reference | Reference | ||
| Female | 1.005 (0.6–1.684) | 0.984 | 1.64 (0.755–3.563) | 0.211 | |
| Age | ≤ 65 | Reference | Reference | ||
| > 65 | 0.696 (0.383–1.263) | 0.233 | 0.447 (0.185–1.081) | 0.074 | |
| ECOG | 0–1 | Reference | Reference | ||
| 2–4 | 1.039 (0.554–1.951) | 0.904 | 1.229 (0.545–2.770) | 0.620 | |
| Tumor site | Head and neck | — | 0.998 | — | 0.999 |
| Esophagus | 0.126 (0.016–1.014) | 0.052 | 0.505 (0.054–4.762) | 0.551 | |
| Lung | 0.389 (0.182–0.829) | 0.014 | 0.716 (0.245–2.089) | 0.54 | |
| Thymus gland | — | 0.999 | — | 0.999 | |
| Gastric | 0.359 (0.119–1.086) | 0.07 | 0.332 (0.035–3.106) | 0.334 | |
| Colorectal | 0.356 (0.141–0.902) | 0.029 | 0.511 (0.159–1.649) | 0.262 | |
| Hepatobiliary | 0.09 (0.011–0.714) | 0.023 | 0.212 (0.024–1.901) | 0.166 | |
| Ovary | 0.152 (0.041–0.564) | 0.005 | 0.081 (0.009–0.696) | 0.022 | |
| Breast | 0.088 (0.011–0.703) | 0.022 | 0.108 (0.011–1.018) | 0.052 | |
| Cervix | 0.253 (0.054–1.196) | 0.083 | 0.185 (0.02–1.679) | 0.134 | |
| Lymphoma | — | 0.997 | — | 0.998 | |
| Kidney | — | 0.999 | — | 0.999 | |
| Bladder | — | 1.0 | — | 1.0 | |
| Pancreas | 1.247 (0.307–5.063) | 0.758 | 1.915 (0.311–11.797) | 0.484 | |
| Other or unknown primary | Reference | Reference | |||
| Stage | I‐III | Reference | |||
| IV | 0.909 (0.317–2.608) | 0.859 | |||
| unknown | 0.954 (0.532–1.708) | 0.873 | |||
| Tumor control | CR/PR | Reference | |||
| SD | — | 0.999 | |||
| PD | — | 0.999 | |||
| Fever | Yes | 4.339 (1.832–10.276) | 0.001 | 4.886 (1.692–14.114) | 0.003 |
| No | Reference | Reference | |||
| ALB (g/L) | ≤ 35 | 1.514 (0.7–3.274) | 0.292 | ||
| > 35 | Reference | ||||
| Liver dysfunction | Yes | 1.19 (0.574–2.469) | 0.639 | ||
| No | Reference | ||||
| Renal dysfunction | Yes | 1.099 (0.258–4.691) | |||
| No | Reference | ||||
| Malignant plasmapheresis | Pleural effusion | 3.378 (1.222–9.336) | 0.019 | 4.812 (1.546–14.975) | 0.007 |
| Ascite | 2.807 (1.109–7.1) | 0.029 | 1.228 (0.326–4.633) | 0.762 | |
| No | Reference | Reference | |||
| Malnutrition requires parenteral nutrition | Yes | 3.772 (1.511–9.421) | 0.004 | 1.149 (0.316–4.176) | 0.833 |
| No | Reference | Reference | |||
- —National High Level Hospital Clinical Research Funding
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeutropenia and Cancer Infections · Platelet Disorders and Treatments · Hematological disorders and diagnostics
Introduction
1
Thrombocytopenia is a common complication of antineoplastic therapy [1], and thrombocytopenia‐induced hemorrhage remains one of the leading causes of mortality among oncology patients. This condition restricts the timely and optimal administration of antineoplastic drugs, increases the demand for transfusions, and exacerbates the medical and economic burden of care [2, 3, 4, 5, 6]. Large‐scale data on the clinical characteristics and treatment outcomes of emergency patients with Cancer therapy‐induced thrombocytopenia (CTIT) remain limited in China. Moreover, a reduced platelet count is not the sole factor contributing to organ bleeding in oncology patients, yet cohort studies specifically examining bleeding during CTIT are lacking. The clinical risk factors associated with organ bleeding in patients with CTIT have not been established. Therefore, this study aims to analyze the clinical characteristics of emergency CTIT patients, identify risk factors influencing their clinical outcomes, and assess both the characteristics and predictive factors of CTIT‐related bleeding.
Methods
2
A total of 8590 patients who visited the Emergency Department of Oncology at the Cancer Hospital of the Chinese Academy of Medical Sciences between January 2023 and May 2023 were retrospectively enrolled. Among them, 1164 patients met the inclusion criteria and were enrolled in the study. Follow‐up: The final follow‐up was conducted in May 2024.
The inclusion criteria: (1) A malignant tumor confirmed by pathological or cytological diagnosis at our hospital; (2) A Platelet count of < 100 × 10^9^/L following anti‐tumor therapy (including chemotherapy, radiotherapy, immunotherapy, or targeted therapy).
Exclusion criteria: (1) Absence of a confirmed malignant tumor diagnosis; (2) No history of antitumor treatment; (3) Thrombocytopenia due to other causes, such as aplastic anemia, acute leukemia, hypersplenism, and bone marrow metastases.
Treatment strategies included platelet‐raising drugs such as recombinant human thrombopoietin (rh‐TPO), interleukin‐11 (IL‐11), and TPO receptor analogs. Additional supportive measures comprised hemostatic agents, parenteral and intranasal nutritional support, anti‐infective therapy, hepatoprotective agents, and gastric acid suppression therapy. For patients with mild thrombocytopenia, clinical management will determine whether to observe or administer thrombopoietic agents based on the specific clinical condition.
Short‐term (28 days of follow‐up) clinical outcomes of disease regression were categorized as follows: (1) improvement: defined by the resolution or alleviation of symptoms, signs, and test marker abnormalities; (2) worsening of disease, characterized by worsening symptoms, signs, test markers, or death; and (3) hospital admission: necessitated by disease progression or other indications for hospitalization. The primary outcome was clinical worsening and the secondary outcome was hospital admission within 28 days of the emergency department visit.
Statistics
2.1
Statistical analyses were performed using IBM SPSS (Version 20.0. Armonk, NY: IBM Corp). Continuous variables were analyzed using the T‐test or Mann–Whitney U test, depending on their distribution. Categorical variables were reported as absolute numbers or percentages and compared using a χ^2^ test. Logistic regression analysis was performed to identify independent predictive risk factors. Statistical significance was set at a two‐tailed p‐value of < 0.05.
Results
3
Clinical Characteristics of CTIT Emergency Patients
3.1
A retrospective analysis was conducted on 8590 cases presented to the oncology emergency department at the Cancer Hospital of the Chinese Academy of Medical Sciences. The median patient age was 59 years, and 49.3% were female. Among these cases, 1164 (13.55%) developed thrombocytopenia as a complication of antitumor therapy, with a median age of 61 years (18–85) and a male‐to‐female ratio of 1.03:1. The median platelet count (Q1 Q3) across 1164 cases was 59 (39 77) × 10^9^/L. The median number (Q1 Q3) of platelets in the hemorrhage group and non‐hemorrhage groups was 48 × 10^9^/L (20 55) and 61 × 10^9^/L (40 78) respectively. Lung cancer was the most frequently observed tumor type in CTIT, accounting for 34.5% of cases. Adenocarcinoma was the most common pathological subtype (62.3%). Of the patients with CTIT, 96.6% had previously received chemotherapy, 8.3% had undergone treatment with immune checkpoint inhibitors, and 5.7% had received targeted therapy. Forty‐nine patients (4.2%) had undergone radiotherapy. Comorbid anemia was present in 16% (186) of CTIT cases, while leukopenia was observed in 58.8% (684). Overt organ bleeding occurred in 61 patients (5.24%), presenting as hemoptysis, hematemesis, hematochezia, hematuria, or vaginal bleeding. Platelet transfusions were administered to 2.5% (30/1164) of affected patients.
The clinical characteristics of the specific 1164 emergency patients with CTIT are shown in Table 1.
CTIT Clinical Treatment Regression
3.2
A total of 1164 CTIT cases were treated in the emergency department. Of these patients, 83.4% received thrombopoietic therapy, including 852 cases (73.1%) of rh‐TPO monotherapy and 82 cases (7.0%) of combined rh‐TPO and TPO‐RA therapy. Details are presented in Table 1. The clinical improvement rate among patients with CTIT was 96.7% (1126/1164), while 29 patients (2.5%) experienced disease progression. No short‐term mortality was observed. Following treatment with platelet‐stimulating medication, a total of 12 cases of thrombosis occurred, all involving lower limb venous thrombosis. Of these, 9 cases occurred in the rh‐TPO monotherapy group, 2 cases in the combination therapy group, and 1 case in the IL‐11 therapy group.
The rate of disease progression was significantly higher in patients with an ECOG score of 2–4 (7.1%) compared to those with an ECOG score of 0–1 (1.3%) (p < 0.001). Similarly, the deterioration rate was higher in patients with stage IV disease than in those with stages I–III (4.2% vs. 0%; p < 0.001). Patients with coexisting fever, anemia, and hypoproteinemia had a significantly higher rate of deterioration than those without these conditions (p < 0.05). Additionally, the proportion of patients showing clinical improvement was lower in those with concurrent renal insufficiency than in those without renal impairment (91.4% vs. 96.9%; p = 0.003). Furthermore, patients with concurrent organ hemorrhage had a higher deterioration rate (9.8%) compared to those without hemorrhage (2.1%; p = 0.001).
Specific CTIT emergency treatment regression characteristics are shown in Table 2.
Risk Factors Affecting CTIT Regression
3.3
Combined organ hemorrhage independently influenced clinical outcomes in patients with CTIT (odds ratio [OR] = 3.029, 95% confidence interval [CI]: 1.049–8.749, p = 0.041). Additionally, ECOG score of 2–4, stage IV disease, anemia, and fever were independent risk factors for treatment deterioration in emergency CTIT patients.
Specific predictors of worsening clinical outcomes in patients attending emergency clinics for CTIT are presented in Table 3 and Figure 1.
Specific predictors of worsening clinical outcomes in patients attending emergency clinics for CTIT.
Clinical Features of Cases of CTIT Combined With Visceral Overt Hemorrhage
3.4
Definition of visceral overt hemorrhage: Clinically observable bleeding symptoms include hemoptysis, hematemesis, hematochezia, hematuria, and vaginal bleeding. Skin hemorrhages and asymptomatic cases with occult blood positivity were excluded.
Among 1164 cases of CTIT, 61 (5.24%) were associated with overt visceral bleeding. Sixteen of these patients required red blood cell transfusions. The most common tumor site among patients with CTIT‐related hemorrhage was the lung (41%, 25/61). The incidence of concurrent fever was significantly higher in the hemorrhage group than in the non‐hemorrhagic group (11.5% vs. 2.9%, p < 0.001). Similarly, pleural and abdominal effusions were more prevalent in the hemorrhage group than in the non‐hemorrhage group (11.4% vs. 4.0% and 13.6% vs. 5.8%, respectively; p = 0.007). Additionally, a higher proportion of patients in the hemorrhage group required parenteral nutritional support due to malnutrition compared to the non‐hemorrhage group (9.8% vs. 2.8%; p = 0.002). The overall improvement rates were 90.2% (55/61) in the hemorrhage group and 97.1% (1071/1103) in the non‐hemorrhage group (p = 0.001).
There was no statistically significant difference between the CTIT bleeding and non‐bleeding groups in terms of tumor stage, antitumor efficacy, hepatic and renal insufficiency, anemia, or leukopenia.
A comparison of the clinical characteristics of the specific 61 patients with CTIT with organ hemorrhage is shown in Table 1.
Risk Factors Predicting Organ Hemorrhage in CTIT
3.5
An ovarian tumor was identified as an independent protective factor against organ hemorrhage in patients with CTIT (odds ratio [OR] = 0.081, 95% confidence interval [CI]: 0.009–0.696, p = 0.022). Febrile symptoms were found to be an independent risk factor for organ hemorrhage in CTIT (odds ratio [OR] = 4.886, 95% confidence interval [CI]: 1.692–14.114, p = 0.003). Pleural effusion was determined to be an independent risk factor for the development of organ hemorrhage on CTIT (odds ratio [OR] = 4.812, 95% confidence interval [CI]: 1.546–14.975, p = 0.007).
Specific risk factors predicting organ hemorrhage in CTIT patients are presented in Table 4 and Figure 2.
Specific risk factors predicting organ hemorrhage in CTIT patients.
Discussion
4
Lack scale cohort data on oncological emergency cases treated with CTIT remain limited. In a retrospective analysis of patients with solid tumors receiving first‐ or second‐line treatment, the incidence of chemotherapy‐induced severe thrombocytopenia (CIT) (platelet count < 75 G/L) was 10.1%, with lung and bladder cancers exhibiting the highest rates of CIT [7]. In this study, nearly one in seven oncology emergency cases involved antitumor therapy‐related thrombocytopenia, with lung cancer being the most frequently associated malignancy, consistent with previous findings. This may be attributed to the high prevalence of lung cancer in China and the common use of chemotherapy regimens containing carboplatin, gemcitabine, and other thrombocytopenia‐inducing agents [8]. Due to the variety of tumor types and the complexity of antitumor regimens in the emergency cases analyzed, specific chemotherapy drugs were not included in the assessment of CTIT cases. Future research will focus on analyzing single‐tumor types and incorporating additional antitumor factors, such as specific chemotherapy regimens.
The incidence of CTIT‐related organ bleeding in this study was 5.24%, while the platelet transfusion rate was 2.5%. A retrospective cross‐sectional study evaluating the efficacy of various platelet‐raising therapies for CTIT [4] reported that among 1437 patients, 49.3% received rhTPO alone, with a platelet transfusion rate of 8.1%. In contrast, this study included all emergency visits for CTIT demonstrated a higher rate of improvement following pharmacological treatment and a lower platelet transfusion rate than the previous study. Another retrospective study investigating CTIT used compared the efficacy and cost‐effectiveness of rhTPO and interleukin‐11, concluding that while both treatments had similar efficacy, interleukin‐11 was more cost‐effective [6]. Additionally, a study of 112 patients with immune thrombocytopenia (ITP) with severe bleeding [9] reported a mortality rate of 30.6% and identified a lack of consensus regarding the prognostic impact of individualized treatments. That the study highlighted the need for a standardized approach to managing ITP with severe bleeding. Notably, no patients in this study died from CTIT‐related bleeding, and long‐term follow‐up will be conducted to clarify differences in long‐term prognosis. A multicenter prospective cohort study on thrombocytopenia in patients in the intensive care unit (ICU) [10] reported that 23.4% of patients had thrombocytopenia at ICU admission and identified hemorrhage as risk a factor for its progression. Similarly, the present study analyzed oncologic emergency oncology cases of CTIT and found that concurrent bleeding was a risk factor for disease. These findings indicate that in critically ill patients, thrombocytopenia accompanied by bleeding is a sign of a severe condition requiring proactive prevention and clinical management.
This study identified combined organ bleeding as an independent risk factor influencing the short‐term outcomes of patients undergoing CTIT. A previous study examining bleeding due to CIT in solid tumors [5] found that bleeding was associated with worse overall survival (OS). The study also concluded that although the overall incidence of bleeding in CIT was low, it exceeded 20% in specific subgroups with relevant clinical characteristics. However, the study did not establish clinical prediction rules for CIT‐related hemorrhages. In our study, the incidence of organ hemorrhage in CTIT was 5.24%. Fever was identified as an independent risk factor for both the clinical outcomes of CTIT and the prediction of organ hemorrhage. Among the patients in our study, 58.8% of CTIT cases were accompanied by leukopenia. Additionally, 94.9% (35/39) of CTIT cases with fever were diagnosed with microbial infections. It is possible that these infections exacerbated bone marrow suppression, accelerated platelet clearance, and shortened platelet lifespan [11, 12], thereby increasing the risk of hemorrhage. A separate study [13] identified age > 65 years, hepatic or renal insufficiency, malnutrition, and co‐infections as risk factors for severe and persistent chemotherapy‐induced myelosuppression. The findings of our study align with those results, as multiple studies have demonstrated that malnutrition exacerbates myelosuppressive toxicity related to antitumor therapy [14, 15]. Additionally, our study found that patients with renal insufficiency had a lower CTIT improvement rate than those with normal renal function. Renal insufficiency negatively affected short‐term CTIT outcomes, and the incidence of bleeding was higher in malnourished patients with CTIT who required parenteral nutritional support. However, neither renal insufficiency nor malnutrition was identified as an independent predictor of CTIT outcomes or bleeding. A possible explanation is that concurrent renal and hepatic impairment affects the clearance and metabolism of chemotherapeutic agents, prolonging their presence in the body and increasing myelosuppressive toxicity [13].
We identified clinical risk factors associated with bleeding in CTIT; however, no definitive drugs have been established for its prevention. A UK‐based, randomized, double‐blind, phase 3 trial [16] comparing tranexamic acid to placebo for the prevention of severe thrombocytopenic bleeding in hematological malignancies found insufficient evidence to support that the routine use of tranexamic acid in reducing bleeding incidence in those receiving high‐dose chemotherapy. In China, Yunnan Baiyao is empirically recommended for hemostasis in patients with organ hemorrhage. Yunnan Baiyao is a traditional Chinese medicine [17, 18], and its potential role in preventing CTIT‐related hemorrhage warrants further investigation.
This study had some limitations. First, certain medicines promoting platelet production in this study are only available within the Chinese context (rhTPO and IL‐11), thereby limiting the possibility of extrapolating the findings to other settings. Secondly, this study did not classify or analyze the antitumor regimens, specific drugs, or the number of treatment cycles administered prior to CTIT. This omission was due to the complexity and diversity of tumor sites and pathological types in emergency cancer patients, as well as the wide variety of treatment regimens available. Consequently, an analysis of specific therapeutic drugs was not conducted at this stage. However, future research will focus on evaluating different treatment regimens for specific tumor types to assess their impact on bleeding in CTIT and to determine the effect of delayed antitumor therapy. Additionally, as a retrospective cohort study, this research primarily examines the current status and recent outcomes of CTIT and bleeding in Chinese patients with oncological emergencies. However, long‐term survival data for all patients have not yet been collected; future investigations will further explore the impact of CTIT and bleeding on the long‐term prognosis of patients with different tumor types.
Finally, emergency oncology is an emerging interdisciplinary field in China, and our center is the first in the country to establish an emergency oncology department. Additionally, it has been designated as a National Clinical Key Specialty in Emergencies. Although this study is a single‐center retrospective cohort study, emergency oncology cohort data in China remain scarce. Therefore, this study analyzed the emergency oncology data of CTIT to contribute to advancing the oncology emergency medicine field and to guide future prospective cohort studies on emergency CTIT.
Conclusion
5
CTIT cases constitute approximately one in seven oncologic emergencies in China. Poor physical condition, fever, organ hemorrhage, and anemia are identified as risk factors for short‐term CTIT regression. Malignancy cases with thrombocytopenia and additional risk factors necessitate heightened clinical vigilance for hemorrhage development.
Author Contributions
Le Tian: conceptualization (equal), funding acquisition (equal), methodology (equal), resources (equal), software (lead), visualization (lead), writing – original draft (lead), writing – review and editing (lead). Jia‐Xin Huang: formal analysis (equal), validation (equal). Xi Zhang: data curation (equal), supervision (supporting). Ning Li: investigation (equal), resources (supporting). Zhi‐Min Bian: software (supporting). Na Li: project administration (supporting). Shao‐Ming Wang: funding acquisition (supporting). Xin‐Qi Liu: supervision (supporting). Zhi‐Yong Li: data curation (supporting), resources (supporting). Qing‐Long Jiang: conceptualization (supporting), investigation (equal), methodology (equal), project administration (equal). Chao Wang: resources (equal), software (equal). Cong Zhao: software (supporting), supervision (supporting). Wei Wei: methodology (supporting), resources (supporting). Ming‐Hua Cong: conceptualization (equal), data curation (supporting), supervision (equal), writing – review and editing (lead).
Funding
This study was supported by the National High Level Hospital Clinical Research Funding (80102022524).
Ethics Statement
This study was in accordance with the principles of the Declaration of Helsinki and was approved by the Medical Ethics Committee of the Cancer Hospital, Chinese Academy of Medical Science (reference number: 24–208/4488). All participants were informed of the purpose of the study and provided signed informed consent. All methods were performed in accordance with the relevant guidelines and regulations.
Consent
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J. Mei , F. Jiao , Y. Li , J. Cui , H. Yang , and L. Wang , “Application of Thrombopoietic Agents in Cancer Therapy‐Induced Thrombocytopenia: A Comprehensive Review,” Blood Reviews 70 (2025): 101257, 10.1016/j.blre.2025.101257.39809679 · doi ↗ · pubmed ↗
- 2N. Denduluri , G. H. Lyman , Y. Wang , et al., “Chemotherapy Dose Intensity and Overall Survival Among Patients With Advanced Breast or Ovarian Cancer,” Clinical Breast Cancer 18, no. 5 (2018): 380–386, 10.1016/j.clbc.2018.02.003.29622384 · doi ↗ · pubmed ↗
- 3A. Gao , L. Zhang , and D. Zhong , “Chemotherapy‐Induced Thrombocytopenia: Literature Review,” Discover Oncology 14, no. 1 (2023): 10, 10.1007/s 12672-023-00616-3.36695938 PMC 9877263 · doi ↗ · pubmed ↗
- 4M. Chen , L. Li , Q. Xia , et al., “A Real‐World Observation on Thrombopoietic Agents for Patients With Cancer Treatment‐Induced Thrombocytopenia in China: A Multicenter, Cross‐Sectional Study,” Cancer 130, no. S 8 (2024): 1524–1538, 10.1002/cncr.35292.38515388 · doi ↗ · pubmed ↗
- 5L. S. Elting , E. B. Rubenstein , C. G. Martin , et al., “Incidence, Cost, and Outcomes of Bleeding and Chemotherapy Dose Modification Among Solid Tumor Patients With Chemotherapy‐Induced Thrombocytopenia,” Journal of Clinical Oncology 19, no. 4 (2001): 1137–1146, 10.1200/JCO.2001.19.4.1137.11181679 · doi ↗ · pubmed ↗
- 6F. M. Gong , F. Y. Liu , X. Ma , et al., “Effectiveness and Economic Evaluation of rh TPO and rh IL‐11 in the Treatment of Cancer Therapy Induced Thrombocytopenia Based on Real‐World Research,” Frontiers in Pharmacology 15 (2024): 1288964, 10.3389/fphar.2024.1288964.38327986 PMC 10848320 · doi ↗ · pubmed ↗
- 7A. Hitron , D. Steinke , S. Sutphin , A. Lawson , J. Talbert , and V. Adams , “Incidence and Risk Factors of Clinically Significant Chemotherapy‐Induced Thrombocytopenia in Patients With Solid Tumors,” Journal of Oncology Pharmacy Practice 17, no. 4 (2011): 312–319, 10.1177/1078155210380293.20823048 · doi ↗ · pubmed ↗
- 8F. Griesinger , E. E. Korol , S. Kayaniyil , N. Varol , T. Ebner , and S. M. Goring , “Efficacy and Safety of First‐Line Carboplatin‐Versus Cisplatin‐Based Chemotherapy for Non‐Small Cell Lung Cancer: A Meta‐Analysis,” Lung Cancer 135 (2019): 196–204, 10.1016/j.lungcan.2019.07.010.31446995 · doi ↗ · pubmed ↗