Transient Dip in Head Circumference Growth Trajectories Associated With Continuous Positive Airway Pressure Administration in Very Preterm Infants
Elena‐Laura Dumitrescu, Christoph Bührer

TL;DR
Using CPAP in very preterm infants temporarily lowers head circumference growth, but it recovers after stopping the treatment.
Contribution
Shows that CPAP causes a temporary drop in head growth in preterm infants, which recovers after discontinuation.
Findings
CPAP initiation caused a significant drop in head circumference percentiles.
Percentiles gradually recovered after CPAP was discontinued.
Head circumference continued to improve until hospital discharge.
Abstract
In preterm infants, decreasing head circumference (HC) percentiles have been linked to neurodevelopmental impairment. Devices for administering continuous positive airway pressure (CPAP) may alter skull morphology. We investigated the impact of sequentially administered CPAP and high‐flow nasal cannula on HC percentiles. In this retrospective single‐institution study of infants < 1500 g birthweight and < 30 weeks gestational age born 2019–2020 (syndromes and intraventricular haemorrhage ≥ grade 2 excluded), routine HC measurements were translated into HC percentiles. We compared data at birth, after CPAP initiation, after partial and complete discontinuation of CPAP, and at discharge. The study included 137 infants (median [interquartile range] gestational age 27+3 [25+5–28+6] weeks, birthweight 890 [715–1120] g). After initiation of CPAP, HC percentiles dropped from 57 [18–77] to 16…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
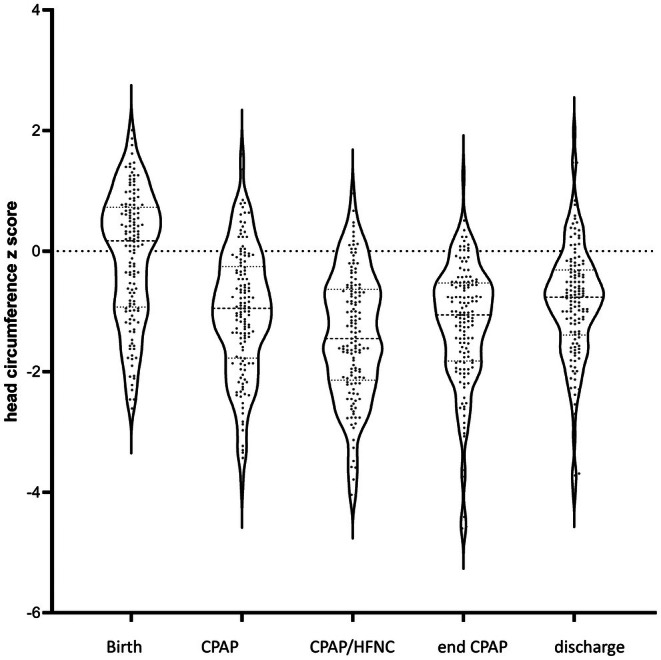 FIGURE 1
FIGURE 1| Birth | CPAP | CPAP/HFNC | End CPAP | Discharge | |
|---|---|---|---|---|---|
| Postmenstrual age (weeks+days) |
27+3 25+5–28+6 |
29+2 28+0–29+2 |
31+6 31+0–31+6 |
33+5 32+2–35+0 |
37+0 36+0–39+1 |
| Chronological age (days) |
0 0–0 |
9 6–13 |
27 17–49 |
46 26–65 |
70 53–90 |
| Birth |
| CPAP |
| CPAP/HFNC |
| End CPAP |
| Discharge |
|---|---|---|---|---|---|---|---|---|
| 57 | < 0.001 | 16 | < 0.001 | 7 | < 0.001 | 14 | < 0.001 | 22 |
| 18–77 | 4–38 | 2–26 | 3–30 | 8–37 |
| Birth |
| CPAP |
| CPAP/HFNC |
| End CPAP |
| Discharge |
|---|---|---|---|---|---|---|---|---|
| 1.15 | < 0.001 | 0.81 | < 0.001 | 0.61 | < 0.001 | 1.00 | < 0.001 | 1.87 |
| 0.80–1.69 | 0.36–1.29 | 0.23–1.17 | 0.61–1.81 | 1.06–4.00 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal Respiratory Health Research · Tracheal and airway disorders · Obstructive Sleep Apnea Research
Background
1
Two cohort studies reported an inverse relationship between the average rate of weekly in‐hospital head circumference (HC) growth and neurodevelopmental scores at 18–22 months [1, 2]. However, little is known about how clinical practice might shape head growth. Infants randomised to receive more amino acids and calories during the first weeks of life were found to have higher HC z scores as opposed to those in the standard group [3]. This did not translate into better motor, language, or combined neurodevelopmental scores at 2–3.5 years of age [4]. Subsequent attempts to promote head growth in hospitalised preterm infants by a variety of nutritional interventions have largely failed. This includes intensified nutrition with parenteral amino acids [5], enteral protein [6], polyunsaturated fatty acids [7], or iron [8]. In Germany, the relative loss of HC for postmenstrual age percentiles between admission and discharge has been viewed as an indicator of quality of care for preterm infants [IQTIG 2023].
At birth, skull sutures are partly open to allow for adaptation of the infant's head to external forces. Administration of continuous positive airway pressure (CPAP) requires devices attached to the infant's head. Inadvertently, these devices exert some pressure. A pilot study has shown that various CPAP devices may gear the head shape towards a turricephalic deformation [9]. Cumulative exposure time to caps for CPAP administration has been reported to be negatively associated with HC and ear‐to‐ear distance z scores [10]. We hypothesized that HC growth trajectories are influenced by the type of noninvasive respiratory support administered. The present study investigates the impact of CPAP, followed by high‐flow nasal cannula (HFNC), on routinely obtained occipitofrontal HC measurements in very preterm infants between birth and discharge.
Methods
2
In this single‐institution retrospective analysis, anonymized routine weight and HC measurements of preterm infants below 1500 g birth weight and less than 30 weeks gestational age born 2019–2020 and admitted within 24 h after birth were retrieved from electronic charts. Infants with recognised syndromes, intraventricular haemorrhage ≥ grade 2, or incomplete data were excluded.
CPAP was administered interchangeably via the Fisher‐Paykel flexitrunk interface (Fisher & Paykel Healthcare Limited, Auckland, New Zealand) or the EasyFlow nCPAP accessory (Fritz Stephan GmbH, Gackenbach, Germany). Both devices consist of nasal prongs or a nasal mask, bonnet, and headgear secured to the infant's head with straps and clips.
Weight and head circumference were considered at 5 time points: first measurement after birth, after definitive start of binasal CPAP with prongs or mask, after start alternation between CPAP and HFNC, after definitive end of CPAP, and the last measurement prior to discharge.
Raw data were transposed into gestational age‐specific and sex‐specific z‐scores and percentiles based on the Fenton growth charts [11] via the Kinderarztrechner online calculator [12]. For infants below 23 weeks gestational age, data from the German perinatal survey were used [13]. SPSS 30.0 (IBM, Armonk, N.Y., USA) was used for the statistical analysis. Data were compared using the related‐samples Friedman analysis of variance followed by paired Wilcoxon tests for adjacent time points, with 2‐tailed p values < 0.05 considered to indicate statistical significance.
All procedures were performed in compliance with relevant laws, institutional guidelines, and the Declaration of Helsinki, as revised in 2024. The study received approval from the local institutional review board (Ethikkommission Charité—Universitätsmedizin Berlin, number EA2/199/22) which waived the need for informed parental consent.
Results
3
Between 1 January 2019 and 31 December 2020, a total of 224 infants below 1500 g birth weight and a gestational age below 30 weeks were admitted. Of these, 33 had intraventricular haemorrhage grade 2 or more, 43 died, and 10 had incomplete data for other reasons. The final study cohort comprised 137 infants (64 girls, 73 boys) with a median gestational age of 27^+3^ weeks^+days^ [interquartile range (IQR) 25^+5^–28^+6^] and a birth weight of 890 [715–1120] g.
Table 1 presents the chronological and postmenstrual age at which measurements were taken after birth, after definitive start of binasal CPAP, after start alternation between CPAP and HFNC, after definitive end of CPAP, and the last measurement prior to discharge.
Head circumference percentiles continuously declined from birth during the administration of CPAP, then rose steadily after partial and definitive withdrawal of CPAP until discharge (Table 2).
A similar picture emerged when head circumferences were expressed in z‐scores (Figure 1).
Violin plots of head circumference z scores at birth, after the start of CPAP, start of alternation between CPAP and HFNC, definitive end of CPAP, and prior to discharge.
The ratios of head circumference percentile to body weight percentile also declined during CPAP and recovered until discharge (Table 3).
Discussion
4
In this cohort of very preterm infants, occipitofrontal HC deviated downwards from intrauterine trajectories while infants were treated with CPAP. This was followed by a catch‐up increase upon CPAP discontinuation. This was not mediated by postnatal growth failure, as the ratios of head percentile to body weight percentile declined during CPAP but fully recovered by discharge, exceeding values at birth.
While previous studies have looked at HC at birth and at discharge, this is the first study examining HC during the entire course of the hospital stay in relation to the type of respiratory support administered. This strength is offset by three limitations. First, the study relied on routine measurements which included occipitofrontal HC but not ear‐to‐ear distances or other measurements. Therefore, we were unable to decide whether the reduced HC in the wake of CPAP represented smaller head volumes or was compensated for by eccentric head growth. Second, the two CPAP devices had been used interchangeably during the study period. Therefore, we could not determine any difference between the two of them. Third, CPAP having become standard of care for preterm infants < 30 weeks gestational age, there was no control group without CPAP.
CPAP‐related transient decline in head circumference for postmenstrual age percentiles may underlie the apparent nadir reported for head circumference between birth and follow‐up measurements at 3–12 months of age [14, 15]. Infants with poor head growth between birth and discharge followed by catch‐up post discharge were found to have a reduced odds ratio of significant neurodevelopmental impairment [16].
In more recent cohorts of preterm infants, the association between changes in HC z scores between birth and discharge and neurodevelopment outcome has faded. In extremely preterm infants below 29 weeks gestational age cared for in hospitals of the Canadian Neonatal Network, changes in HC between birth and discharge were neither related to Bayley‐III scores at 18–24 months corrected age nor to neurodevelopmental impairment [17]. In contrast, there were some small associations between head growth post‐discharge and neuromotor development. In a single‐institution study in Leipzig, Germany, no correlations emerged between cognitive abilities at 2 years and the slopes of HC between birth and discharge [10]. A population‐based cohort study including all live‐born infants below 28 weeks gestational age in 2006–2012 in Switzerland also found no association between declining head circumference z‐scores between birth and discharge and neurodevelopmental impairment at 2 years of age [18].
Conclusion
5
Data of this study suggests that the HC trajectories in the hospitalised very preterm infants studied were influenced by devices to deliver non‐invasive respiratory support. Apparent loss of HC percentiles during CPAP was reversed upon discontinuation of CPAP. These observations may explain the poor predictive power of HC at discharge for future neurodevelopment.
Author Contributions
Elena‐Laura Dumitrescu: project administration, investigation, data curation, writing – review and editing, validation. Christoph Bührer: conceptualization, methodology, formal analysis, supervision, writing – original draft.
Funding
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1R. A. Ehrenkranz , A. M. Dusick , B. R. Vohr , L. L. Wright , L. A. Wrage , and W. K. Poole , “Growth in the Neonatal Intensive Care Unit Influences Neurodevelopmental and Growth Outcomes of Extremely Low Birth Weight Infants,” Pediatrics 117, no. 4 (2006): 1253–1261, 10.1542/peds.2005-1368.16585322 · doi ↗ · pubmed ↗
- 2M. B. Belfort , S. L. Rifas‐Shiman , T. Sullivan , et al., “Infant Growth Before and After Term: Effects on Neurodevelopment in Preterm Infants,” Pediatrics 128, no. 4 (2011): e 899–e 906, 10.1542/peds.2011-0282.21949135 PMC 3182845 · doi ↗ · pubmed ↗
- 3C. Morgan , P. Mc Gowan , S. Herwitker , A. E. Hart , and M. A. Turner , “Postnatal Head Growth in Preterm Infants: A Randomized Controlled Parenteral Nutrition Study,” Pediatrics 133, no. 1 (2014): e 120–e 128, 10.1542/peds.2013-2207.24379229 · doi ↗ · pubmed ↗
- 4C. Morgan , S. Parry , J. Park , and M. Tan , “Neurodevelopmental Outcome in Very Preterm Infants Randomised to Receive Two Different Standardised, Concentrated Parenteral Nutrition Regimens,” Nutrients 15, no. 22 (2023): 4741, 10.3390/nu 15224741.38004135 PMC 10674254 · doi ↗ · pubmed ↗
- 5A. Trivedi , V. Jatana , and J. K. Sinn , “Early Versus Late Administration of Amino Acids in Preterm Infants Receiving Parenteral Nutrition,” Cochrane Database of Systematic Reviews 1, no. 1 (2024): CD 008771, 10.1002/14651858.CD 008771.pub 3.38275196 PMC 10811752 · doi ↗ · pubmed ↗
- 6M. Sanchez‐Holgado , M. J. Johnson , A. Witte Castro , et al., “Systematic Review and Meta‐Analysis of Enteral Protein Intake Effects on Growth in Preterm Infants,” Pediatric Research 98 (2025): 1696–1710, 10.1038/s 41390-025-04115-9.40473805 PMC 12602309 · doi ↗ · pubmed ↗
- 7C. T. Collins , M. Makrides , R. A. Gibson , et al., “Pre‐ and Post‐Term Growth in Pre‐Term Infants Supplemented With Higher‐Dose DHA: A Randomised Controlled Trial,” British Journal of Nutrition 105, no. 11 (2011): 1635–1643, 10.1017/S 000711451000509 X.21443815 · doi ↗ · pubmed ↗
- 8R. M. Manapurath , B. Gadapani Pathak , B. Sinha , et al., “Enteral Iron Supplementation in Preterm or Low Birth Weight Infants: A Systematic Review and Meta‐Analysis,” Pediatrics 50, no. Suppl 1 (2022): e 2022057092 I, 10.1542/peds.2022-057092 I.35921671 · doi ↗ · pubmed ↗