Lactate Dehydrogenase-Derived Indices and Prognosis in Patients with Resectable Gastric Cancer
Masayuki Urabe, Mami Suzuki, Takahiro Fukai, Yui Hasegawa, Emi Terai, Yoshitaka Kiya, Goki Morizono, Masaya Hiyoshi, Toshiyuki Watanabe, Yojiro Hashiguchi

TL;DR
This study shows that two blood-based indices derived from lactate dehydrogenase can predict survival outcomes in patients with resectable gastric cancer.
Contribution
The study introduces LDH-based indices (LLR and LAR) as novel independent prognostic markers for gastric cancer patients.
Findings
LLR and LAR outperformed LDH alone in predicting overall and relapse-free survival.
High LLR and LAR were independently associated with worse survival outcomes in multivariate analysis.
These indices could help identify high-risk gastric cancer patients preoperatively.
Abstract
Robust methodologies for risk stratification remain necessary for gastric cancer (GC). We investigated the prognostic significance of preoperative lactate dehydrogenase (LDH) and two LDH-based indices, the LDH-to-lymphocyte ratio (LLR) and LDH-to-albumin ratio (LAR), in patients undergoing curative resection for GC. We retrospectively reviewed the medical records of 225 consecutive patients with GC who underwent R0 surgical resection. The prognostic value of preoperative LDH, LLR, and LAR was assessed using time-dependent receiver operating characteristic curves and Cox proportional hazards regression. Optimal cut-off values were determined with X-tile software. The median follow-up period was 61 months. The areas under the curves for predicting overall survival (OS) and relapse-free survival (RFS) were notably higher for LLR and LAR as compared to LDH alone. In univariate Cox…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
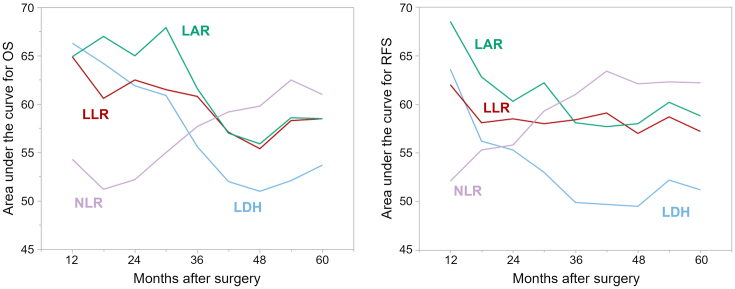 Figure 1
Figure 1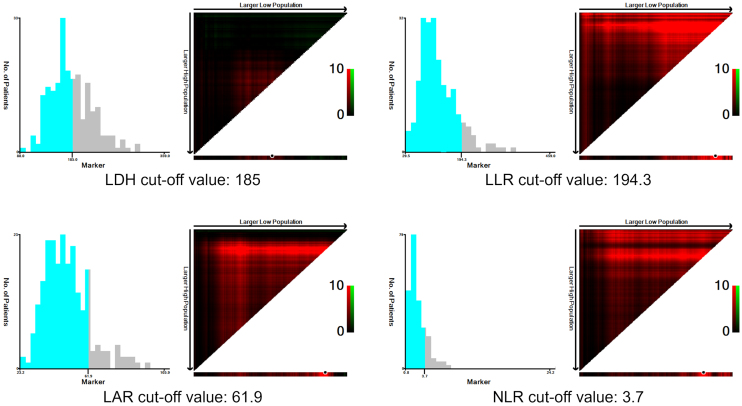 Figure 2
Figure 2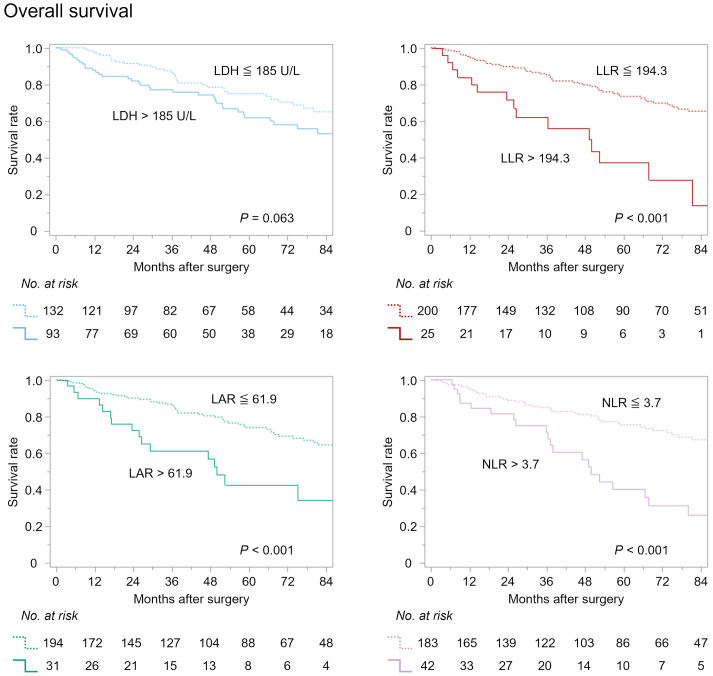 Figure 3
Figure 3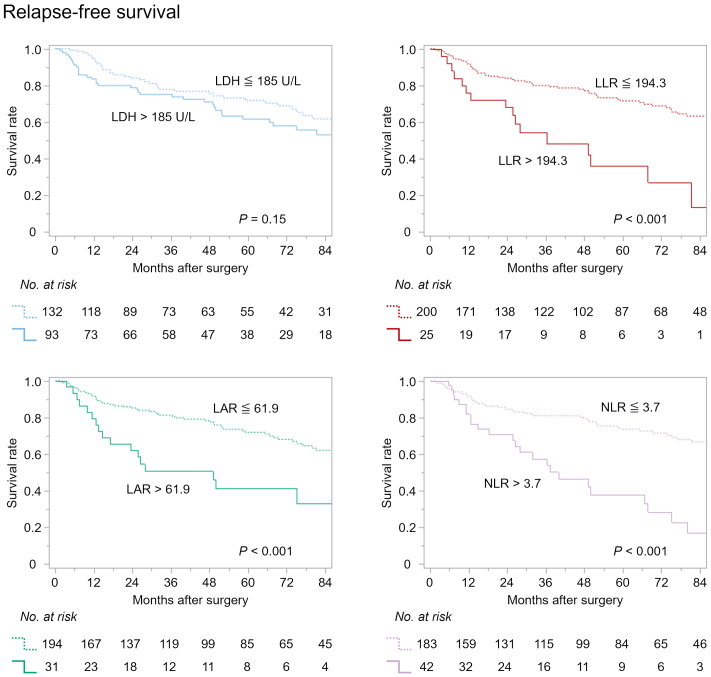 Figure 4
Figure 4| Characteristics | # | LDH, U/L | p Value | LLR | p Value | LAR | p Value |
|---|---|---|---|---|---|---|---|
| Total | 225 | 178 (155-211) | 114.2 (86.1-155.9) | 47.9 (40.1-57.1) | |||
|
| |||||||
| ≤69 | 71 | 169 (148-196) | 0.042* | 99.7 (72.5-123.4) | <0.001* | 42.8 (36.5-52.1) | <0.001* |
| ≥70 | 154 | 181 (157-213) | 120.0 (93.1-170.5) | 50.3 (42.3-58.0) | |||
|
| |||||||
| Male | 154 | 173 (154-200) | 0.10 | 114.5 (82.1-156.0) | 0.61 | 45.9 (39.5-55.5) | 0.023* |
| Female | 71 | 194 (157-213) | 113.9 (92.6-156.1) | 51.9 (44.7-57.6) | |||
|
| |||||||
| Absent | 214 | 177 (154-210) | 0.017* | 113.9 (86.2-153.3) | 0.34 | 47.9 (39.8-56.6) | 0.094 |
| Present | 11 | 197 (187-259) | 149.1 (85.4-190.8) | 55.4 (44.9-67.9) | |||
|
| |||||||
| Intestinal | 149 | 177 (156-210) | 0.79 | 113.9 (87.3-156.4) | 0.84 | 47.9 (39.9-57.1) | 0.78 |
| Diffuse | 76 | 179 (153-213) | 114.2 (83.1-155.1) | 47.6 (40.3-57.1) | |||
|
| |||||||
| Partial | 168 | 181 (159-212) | 0.096 | 113.5 (88.4-152.9) | 0.83 | 47.0 (40.3-56.6) | 0.43 |
| Total | 57 | 171 (147-203) | 115.8 (83.6-167.0) | 50.0 (39.9-58.6) | |||
|
| |||||||
| Open | 186 | 180 (156-212) | 0.19 | 116.0 (88.8-157.1) | 0.11 | 49.4 (41.2-58.0) | <0.001* |
| Laparoscopic/robotic | 39 | 169 (155-200) | 107.0 (76.2-137.7) | 40.9 (26.0-45.6) | |||
|
| |||||||
| T1 | 96 | 176 (154-208) | 0.46 | 108.5 (79.2-143.1) | 0.015* | 44.8 (38.5-53.3) | 0.001* |
| T2-4 | 129 | 180 (156-213) | 119.3 (92.0-167.5) | 50.7 (42.0-58.7) | |||
|
| |||||||
| N0 | 148 | 178 (156-212) | 0.47 | 113.0 (85.5-150.1) | 0.32 | 46.7 (39.6-57.2) | 0.27 |
| N1-3 | 77 | 179 (152-205) | 116.7 (88.3-169.2) | 49.4 (42.5-56.9) | |||
|
| |||||||
| Absent | 99 | 175 (156-210) | 0.68 | 113.9 (88.3-152.4) | 0.69 | 44.9 (39.3-54.3) | 0.005* |
| Present | 126 | 180 (155-211) | 115.0 (86.0-162.5) | 50.8 (42.0-58.4) | |||
|
| |||||||
| Absent | 200 | 180 (156-212) | 0.14 | 115.1 (89.2-156.0) | 0.095 | 48.8 (41.2-57.6) | 0.004* |
| Present | 25 | 166 (150-191) | 86.2 (68.1-167.9) | 39.8 (36.7-47.9) | |||
|
| |||||||
| Absent | 189 | 177 (154-210) | 0.55 | 114.3 (88.2-158.4) | 0.35 | 47.3 (40.1-55.9) | 0.29 |
| Present | 36 | 181 (161-216) | 107.2 (82.1-141.6) | 50.7 (40.0-60.9) | |||
|
| |||||||
| Absent | 201 | 178 (156-212) | 0.68 | 111.5 (82.4-149.8) | <0.001* | 47.9 (39.8-56.9) | 0.23 |
| Present | 24 | 178 (153-197) | 150.8 (114.6-209.1) | 47.8 (43.1-67.4) |
| Characteristics | Overall survival | Relapse-free survival | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age at surgery (≥70 years) | 2.39 (1.32-4.31) | 0.004* | 1.95 (1.13-3.36) | 0.016* |
| Gender (male) | 1.89 (1.07-3.33) | 0.029* | 1.95 (1.12-3.38) | 0.018* |
| Hepatitis (present) | 3.34 (1.53-7.31) | 0.003* | 2.84 (1.31-6.20) | 0.009* |
| Main histology (intestinal) | 1.35 (0.81-2.25) | 0.25 | 1.35 (0.83-2.20) | 0.23 |
| Type of gastrectomy (total) | 2.17 (1.34-3.50) | 0.002* | 2.13 (1.34-3.37 | 0.001* |
| Surgical approach (open) | 1.90 (0.82-4.39) | 0.13 | 1.84 (0.84-4.00) | 0.13 |
| pT classification (T2-4) | 3.01 (1.72-5.26) | <0.001* | 3.23 (1.88-5.54) | <0.001* |
| pN classification (N1-3) | 2.28 (1.43-3.63) | <0.001* | 2.56 (1.63-4.01) | <0.001* |
| Lymphovascular involvement (present) | 2.30 (1.37-3.87) | 0.002* | 2.70 (1.62-4.51) | <0.001* |
| Preoperative ER (present) | 0.46 (0.15-1.47) | 0.19 | 0.38 (0.12-1.22) | 0.10 |
| Adjuvant chemotherapy (present) | 1.70 (0.98-2.94) | 0.057 | 1.90 (1.11-3.22) | 0.018* |
| Postoperative complications (present) | 2.18 (1.17-4.06) | 0.014* | 1.87 (1.01-3.47) | 0.046* |
| Preoperative LDH (>185 U/L) | 1.55 (0.97-2.47) | 0.065 | 1.38 (0.88-2.17) | 0.15 |
| Preoperative LLR (>194.3) | 3.30 (1.85-5.88) | <0.001* | 2.97 (1.70-5.19) | <0.001* |
| Preoperative LAR (>61.9) | 2.68 (1.55-4.63) | <0.001* | 2.61 (1.53-4.43) | <0.001* |
| Preoperative NLR (>3.7) | 2.92 (1.76-4.86) | <0.001* | 3.31 (2.03-5.38) | <0.001* |
| Model for LDH | ||
|---|---|---|
| Characteristics | Overall survival | |
| Adjusted HR (95% CI) | p Value | |
| Age at surgery (≥70 years) | 2.83 (1.51-5.30) | 0.001* |
| Gender (male) | 2.59 (1.40-4.80) | 0.003* |
| Type of gastrectomy (total) | 1.40 (0.82-2.41) | 0.22 |
| pT classification (T2-4) | 2.16 (1.13-4.12) | 0.020* |
| pN classification (N1-3) | 1.54 (0.79-3.00) | 0.21 |
| Preoperative ER (present) | 0.58 (0.18-1.93) | 0.38 |
| Adjuvant chemotherapy (present) | 0.87 (0.43-1.76) | 0.70 |
| Preoperative NLR (>3.7) | 1.84 (1.07-3.16) | 0.027* |
| Preoperative LDH (>185 U/L) | 1.53 (0.94-2.48) | 0.084 |
|
| ||
|
|
| |
|
|
| |
| Age at surgery (≥70 years) | 2.82 (1.51-5.24) | 0.001* |
| Gender (male) | 2.58 (1.39-4.77) | 0.003* |
| Type of gastrectomy (total) | 1.53 (0.89-2.61) | 0.12 |
| pT classification (T2-4) | 2.18 (1.13-4.21) | 0.020* |
| pN classification (N1-3) | 1.47 (0.76-2.86) | 0.25 |
| Preoperative ER (present) | 0.43 (0.12-1.47) | 0.18 |
| Adjuvant chemotherapy (present) | 0.94 (0.47-1.88) | 0.86 |
| Preoperative NLR (>3.7) | 1.34 (0.73-2.43) | 0.34 |
| Preoperative LLR (>194.3) | 2.66 (1.34-5.28) | 0.005* |
|
| ||
|
|
| |
|
|
| |
| Age at surgery (≥70 years) | 2.95 (1.58-5.48) | < 0.001* |
| Gender (male) | 2.63 (1.42-4.89) | 0.002* |
| Type of gastrectomy (total) | 1.29 (0.75-2.22) | 0.37 |
| pT classification (T2-4) | 2.13 (1.10-4.12) | 0.025* |
| pN classification (N1-3) | 2.05 (1.02-4.10) | 0.044* |
| Preoperative ER (present) | 0.61 (0.18-2.03) | 0.42 |
| Adjuvant chemotherapy (present) | 0.76 (0.38-1.55) | 0.45 |
| Preoperative NLR (>3.7) | 1.68 (0.98-2.88) | 0.060 |
| Preoperative LAR (>61.9) | 2.61 (1.45-4.71) | 0.001* |
| Model for LDH | ||
|---|---|---|
| Characteristics | Relapse-free survival | |
| Adjusted HR (95% CI) | p Value | |
| Age at surgery (≥70 years) | 2.17 (1.22-3.84) | 0.008* |
| Gender (male) | 2.58 (1.43-4.68) | 0.002* |
| Type of gastrectomy (total) | 1.26 (0.75-2.12) | 0.38 |
| pT classification (T2-4) | 2.13 (1.14-3.99) | 0.018* |
| pN classification (N1-3) | 1.69 (0.90-3.18) | 0.11 |
| Preoperative ER (present) | 0.52 (0.16-1.72) | 0.29 |
| Adjuvant chemotherapy (present) | 0.91 (0.46-1.78) | 0.78 |
| Preoperative NLR (>3.7) | 2.02 (1.20-3.40) | 0.009* |
| Preoperative LDH (>185 U/L) | 1.40 (0.88-2.23) | 0.15 |
|
| ||
|
|
| |
|
|
| |
| Age at surgery (≥70 years) | 2.15 (1.22-3.79) | 0.008* |
| Gender (male) | 2.55 (1.41-4.61) | 0.002* |
| Type of gastrectomy (total) | 1.36 (0.81-2.28) | 0.25 |
| pT classification (T2-4) | 2.13 (1.13-4.02) | 0.020* |
| pN classification (N1-3) | 1.62 (0.86-3.02) | 0.13 |
| Preoperative ER (present) | 0.41 (0.12-1.38) | 0.15 |
| Adjuvant chemotherapy (present) | 0.96 (0.50-1.87) | 0.92 |
| Preoperative NLR (>3.7) | 1.53 (0.86-2.74) | 0.15 |
| Preoperative LLR (>194.3) | 2.22 (1.14-4.31) | 0.019* |
|
| ||
|
|
| |
|
|
| |
| Age at surgery (≥70 years) | 2.10 (1.18-3.72) | 0.011* |
| Gender (male) | 2.59 (1.43-4.69) | 0.002* |
| Type of gastrectomy (total) | 1.13 (0.67-1.91) | 0.65 |
| pT classification (T2-4) | 2.11 (1.11-3.99) | 0.022* |
| pN classification (N1-3) | 2.25 (1.16-4.34) | 0.016* |
| Preoperative ER (present) | 0.55 (0.17-1.83) | 0.33 |
| Adjuvant chemotherapy (present) | 0.79 (0.40-1.55) | 0.50 |
| Preoperative NLR (>3.7) | 1.86 (1.10-3.12) | 0.020* |
| Preoperative LAR (>61.9) | 2.65 (1.49-4.72) | <0.001* |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Inflammatory Biomarkers in Disease Prognosis · Esophageal Cancer Research and Treatment
Introduction
Gastric cancer (GC) remains one of the most lethal malignancies, currently ranking fifth among causes of cancer-related mortality worldwide ^(1)^. Despite advances in therapeutic strategies, improvements in prognosis have been modest, and GC continues to pose a major public health challenge ^(2)^. In the current era of multimodal treatment strategies anchored in surgical resection, pretreatment risk stratification is essential, and there is a pressing need for reliable, readily accessible tools to inform therapeutic decision-making. However, effective modalities to optimize treatment selection remain limited.
Lactate dehydrogenase (LDH) is a ubiquitous cytoplasmic enzyme that catalyzes the conversion of pyruvate to lactate during anaerobic glycolysis and is widely used in clinical practice as a marker of tissue injury. Owing to its integral role in cancer metabolism, LDH has been classically proposed as a potential prognostic biomarker in various solid tumors and hematologic malignancies ^(3), (4)^. Nevertheless, its prognostic significance in GC remains controversial ^(5), (6)^. Moreover, LDH-derived indices, such as the LDH-to-lymphocyte ratio (LLR) and LDH-to-albumin ratio (LAR) ^(7), (8), (9), (10), (11)^, have not been comprehensively evaluated in the context of GC.
We hypothesized that LDH and LDH-related indices may serve as valuable biomarkers for stratifying survival outcomes in GC. To test this hypothesis, we performed a retrospective analysis to assess their prognostic significance in patients who underwent curative resection for GC.
Materials and Methods
Study population
From a prospectively maintained institutional database, we identified 293 consecutive patients who underwent oncological gastrectomy with lymphadenectomy for GC between August 2010 and December 2024. Sixty-eight patients were excluded for the following reasons: R1 or R2 resection margins (n = 27), cancer of the remnant stomach (n = 9), synchronous malignancies (n = 16), receipt of neoadjuvant chemotherapy (n = 2), emergency surgery (n = 1), follow-up of less than 1 month (n = 1), or incomplete perioperative data (n = 12). No cases with cholangitis, acute infectious diseases, or connective tissue diseases were included. The medical records of the remaining 225 patients were retrospectively reviewed. This study was approved by the Institutional Review Board (number 24-33).
Clinicopathological data
Tumor stage was assigned according to the eighth edition of the Union for International Cancer Control Tumor-Node-Metastasis classification ^(12)^. Histological subtype was categorized as intestinal or diffuse, based on Lauren’s criteria ^(13)^. Postoperative complications were defined as events occurring within 30 days of surgery and graded as Clavien-Dindo grade ≥III ^(14)^.
Postoperative surveillance was conducted in accordance with the Japanese Gastric Cancer Association guidelines, with follow-up scheduled for at least 5 years or until death ^(15)^. For patients diagnosed with pathological stage II/III disease (excluding T3N0), the introduction of adjuvant chemotherapy based on S-1 (an oral fluoropyrimidine derivative) was considered. Postoperative follow-up routinely included physical examination, esophagogastroduodenoscopy, computed tomography, abdominal ultrasonography, and blood tests. When recurrence was detected, systemic chemotherapy was initiated when clinically appropriate, based on the patient’s general condition, organ function, and extent of disease. For patients who missed scheduled visits, survival and recurrence status were confirmed by telephone interview. Surveillance for all patients was completed in July 2025. During the study period, 71 deaths occurred, comprising 28 cancer-specific and 43 non-GC-related deaths. As of the last follow-up, the median follow-up duration among survivors was 61 months.
LDH and LDH-based indices
Preoperative blood test data were basically obtained within 7 days before surgery. The LLR was calculated as serum LDH (U/L) divided by total lymphocyte count (×10^3^/μL), and the LAR as serum LDH (U/L) divided by serum albumin (g/dL).
In addition to LDH and LDH-derived indices, the preoperative neutrophil-to-lymphocyte ratio (NLR) was evaluated as a representative prognostic marker in GC ^(16)^. NLR was calculated as the neutrophil count divided by the total lymphocyte count.
Statistical analysis
Statistical analyses were performed using JMP Student Edition version 18.2.1 (SAS Institute, Cary, NC, USA), X-tile version 3.6.1 (Yale University, New Haven, CT, USA), and R version 4.5.1 (R Foundation for Statistical Computing, Vienna, Austria). All tests were two-tailed, and a P value <0.05 was considered statistically significant.
Continuous variables were compared using the Wilcoxon rank-sum test. Overall survival (OS) was defined as the interval from surgery to death from any cause, and relapse-free survival (RFS) as the interval from surgery to recurrence or death from any cause. Optimal cut-off values for LDH, LLR, LAR, and NLR were determined using X-tile plots based on survival outcomes ^(17)^. Survival curves were generated with the Kaplan-Meier method and compared using the log-rank test. Factors associated with OS and RFS were first evaluated by univariate Cox proportional hazards regression, followed by multivariate models adjusting for known prognostic variables: age at surgery, sex, type of gastrectomy, tumor depth, nodal metastasis, preoperative endoscopic resection, adjuvant chemotherapy, and preoperative NLR ^(16), (18)^. The number of variables included in the model was restricted according to the number of events to ensure stability and prevent overfitting. To mitigate potential collinearity, each index was analyzed using separate models. Time-dependent receiver operating characteristic (ROC) curves for survival prediction based on preoperative LDH, LLR, LAR, and NLR were generated using the “timeROC” function in R.
Results
Associations of preoperative LDH, LLR, and LAR with clinicopathological characteristics
The associations between preoperative indices and baseline clinicopathological characteristics are presented in Table 1. Preoperative LDH was significantly associated with age, dichotomized at 70 years. The LLR was significantly associated with age, tumor depth, and the occurrence of postoperative complications. The LAR demonstrated significant associations with age, gender, surgical approach, tumor depth, lymphovascular invasion, and prior endoscopic resection.
Linear regression analyses were conducted to evaluate the associations of preoperative LDH, LLR, and LAR with NLR. No significant correlation was observed between LDH and NLR (p = 0.41, R^2^ = 0.0030). Although both LLR and LAR exhibited significant associations with NLR (LLR: p < 0.001, R^2^ = 0.31; LAR: p = 0.021, R^2^ = 0.024), the strength of these correlations was weak, as indicated by low R^2^ values.
Time-dependent ROC analyses
Time-dependent ROC analyses were performed, and the area under the curve values for each index were plotted over time to compare their prognostic performance (Figure 1). The preoperative LLR and LAR demonstrated superior predictive accuracy for both OS and RFS compared to LDH. Furthermore, the prognostic performance of LLR and LAR was largely comparable to that of the preoperative NLR. The prognostic accuracy of preoperative LLR and LAR was particularly high during the relatively early postoperative period, within 3 years after surgery.
Time-dependent ROC analyses for overall and relapse-free survival estimations.ROC: receiver operating characteristic.
Determination of cut-off points and survival curve analyses
Optimal cut-off values for each index were determined using X-tile software, based on 5-year survival data from the entire patient cohort. The resulting cut-off values were 185 U/L for LDH, 194.3 for LLR, 61.9 for LAR, and 3.7 for NLR (Figure 2).
Determination of cut-off values using X-tile software.
Patients were stratified into high and low groups according to these thresholds, and Kaplan-Meier survival analyses were conducted for both OS (Figure 3) and RFS (Figure 4). While the preoperative LDH level did not significantly stratify OS (p = 0.063), LLR, LAR, and NLR all demonstrated significant prognostic discrimination for OS (all p < 0.001). Similarly, RFS was significantly stratified by preoperative LLR, LAR, and NLR (all p < 0.001), whereas LDH failed to show a statistically significant association (p = 0.15).
Overall survival curves according to preoperative LDH, LLR, LAR, and NLR.LAR: LDH-to-albumin ratio; LDH: lactate dehydrogenase; LLR: LDH-to-lymphocyte ratio; NLR: neutrophil-to-lymphocyte ratio.
Relapse-free survival curves according to preoperative LDH, LLR, LAR, and NLR.LAR: LDH-to-albumin ratio; LDH: lactate dehydrogenase; LLR: LDH-to-lymphocyte ratio; NLR: neutrophil-to-lymphocyte ratio.
Univariate and multivariate Cox regression analyses
Univariate Cox regression analyses showed that preoperative LLR, LAR, and NLR were significantly associated with both OS and RFS (all p < 0.001), whereas preoperative LDH was not (Table 2). In multivariate analysis, both LLR and LAR emerged as independent predictors of OS (high LLR: hazard ratio [HR] 2.66, 95% confidence interval [CI] 1.34-5.28, p = 0.005) (high LAR: HR 2.61, 95% CI 1.45-4.71, p = 0.001), while LDH remained non-significant (Table 3). For RFS, LLR, and LAR also retained independent prognostic value in the multivariate model (high LLR: HR 2.22, 95% CI 1.14-4.31, p = 0.019) (high LAR: HR 2.65, 95% CI 1.49-4.72, p < 0.001), whereas LDH again was not significant (Table 4).
Discussion
In this study, we retrospectively evaluated the association between preoperative LDH, LDH-derived indices, and survival outcomes in patients with resectable GC. LDH alone did not exhibit a significant association with long-term outcomes. However, two composite indices, which integrate LDH with total lymphocyte count and albumin level, respectively, demonstrated significant prognostic relevance. Notably, their predictive performance was comparable to that of the conventional NLR, and, in multivariate analysis, both LLR and LAR overperformed NLR in terms of independent prognostic power.
LAR has been widely recognized as a predictor of outcomes in cardiovascular, cerebrovascular, and respiratory diseases ^(7), (8), (9)^. In contrast, evidence linking LAR to cancer prognosis remains limited. For GC specifically, we identified only a single study, which included a highly limited sample size (n = 81) ^(19)^. Regarding LLR, it has been described as a prognostic marker in renal cell carcinoma and diffuse large B-cell lymphoma ^(10), (11)^, but no prior study has evaluated its relevance in GC. To our knowledge, this is the first study to demonstrate that preoperative LLR independently predicts prognosis in patients with resectable GC.
LDH is well recognized as an indicator of non-specific tissue injury, but it also plays a pivotal role in anaerobic metabolism, a hallmark of cancer cells driven by enhanced glycolytic activity. LDH has been reported as both a prognostic biomarker and a tool for monitoring therapeutic response in various malignancies ^(3), (4)^. Additionally, elevated LDH levels correlate with higher infiltration of immune cells, including macrophages, neutrophils, T helper cells, tumor-infiltrating lymphocytes, and regulatory T cells, suggesting a link with the immune-inflammatory microenvironment ^(3), (20)^. Despite this biological plausibility, the prognostic significance of LDH in GC remains controversial ^(5), (6)^. In our analysis, LDH alone exhibited only a modest, non-significant association with survival. By contrast, when integrated with lymphocyte count or albumin, LDH-based indices demonstrated substantially stronger prognostic performance. Intriguingly, when we assessed their association with cancer-specific survival versus non-GC-related mortality, neither LLR nor LAR showed strong correlations with cancer-specific outcomes; instead, both were significantly associated with non-GC-related deaths (Supplementary Figure S1). Our time-dependent ROC analyses demonstrated that LLR and LAR exhibited particularly high prognostic accuracy during the relatively early postoperative period (Figure 1). These observations suggest that LDH, as a surrogate for non-specific tissue damage, systemic inflammation, and immune dysregulation, in combination with nutritional status, may help identify patients at elevated risk of early-phase mortality from non-cancer-related causes.
Routine measurement of LDH and calculation of LDH-based indices could facilitate the identification of high-risk patients and enable more individualized treatment strategies. Notably, elderly patients with GC are highly susceptible to non-cancer-related mortality ^(21)^. In the current era, where the incidence of elderly GC cases is increasing at an alarming rate ^(22)^, identifying factors such as LLR and LAR that can predict such outcomes holds considerable clinical significance. Patients with elevated LLR or LAR may warrant special consideration for surgical safety rather than oncological radicality, such as minimizing the extent of lymphadenectomy or tailoring the resection range. Thus, LDH-based markers may serve as valuable tools to guide risk-adapted treatment planning.
This study has limitations. First, its retrospective, single-institution design could introduce the potential for selection bias. Second, the study period (2010-2024) encompassed substantial changes in clinical practice, including widespread adoption of minimally invasive approaches, implementation of enhanced recovery after surgery protocols, and significant advances in perioperative systemic therapy ^(2)^. Third, the competing risk of non-GC-related deaths may have led to an underestimation of disease-specific prognostic associations. Fourth, while dichotomization based on cut-off values is a common approach in clinical research, it can lead to loss of statistical power and insufficient control of confounding factors ^(23)^. These factors may have influenced outcomes. Validation in larger, prospective, multicenter cohorts is warranted.
In summary, preoperative LLR and LAR were identified as independent predictors of survival outcomes in patients undergoing radical surgery for GC. These parameters may facilitate early-phase risk stratification in resectable GC cases and contribute to the optimization of tailored treatment strategies.
Article Information
Author Contributions
Masayuki Urabe contributed to the conception and design of the study. All authors acquired data. Masayuki Urabe performed data interpretation and drafted the manuscript. Yoshitaka Kiya, Goki Morizono, Masaya Hiyoshi, Toshiyuki Watanabe, and Yojiro Hashiguchi critically revised the manuscript. All authors read and approved the final version prior to submission.
Conflicts of Interest
None
Approval by Institutional Review Board
This study was approved by the institutional ethics committee of the Japanese Red Cross Omori Hospital (Identification 24-33).
Informed Consent
Written informed consent was waived because of the retrospective design.
Supplement
Supplementary MaterialSupplementary Figure S1. Cancer-specific survival curves and non-GC-related death curves according to preoperative LDH, LLR, LAR, and NLR.LAR: LDH-to-albumin ratio; LDH: lactate dehydrogenase; LLR: LDH-to-lymphocyte ratio; NLR: neutrophil-to-lymphocyte ratio.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229-63.38572751 10.3322/caac.21834 · doi ↗ · pubmed ↗
- 2Smyth EC, Nilsson M, Grabsch HI, et al. Gastric cancer. Lancet. 2020;396(10251):635-48.32861308 10.1016/S 0140-6736(20)31288-5 · doi ↗ · pubmed ↗
- 3Zhang J, Yao YH, Li BG, et al. Prognostic value of pretreatment serum lactate dehydrogenase level in patients with solid tumors: a systematic review and meta-analysis. Sci Rep. 2015;5:9800.25902419 10.1038/srep 09800 PMC 5386114 · doi ↗ · pubmed ↗
- 4Schneider RJ, Seibert K, Passe S, et al. Prognostic significance of serum lactate dehydrogenase in malignant lymphoma. Cancer. 1980;46(1):139-43.6992974 10.1002/1097-0142(19800701)46:1<139::aid-cncr 2820460122>3.0.co;2-8 · doi ↗ · pubmed ↗
- 5Feng Y, Xiong Y, Qiao T, et al. Lactate dehydrogenase A: a key player in carcinogenesis and potential target in cancer therapy. Cancer Med. 2018;7(12):6124-36.30403008 10.1002/cam 4.1820 PMC 6308051 · doi ↗ · pubmed ↗
- 6Chen J, Zou X. Prognostic significance of lactate dehydrogenase and its impact on the outcomes of gastric cancer: a systematic review and meta-analysis. Front Oncol. 2023;13:1247444.37727205 10.3389/fonc.2023.1247444 PMC 10505930 · doi ↗ · pubmed ↗
- 7Zeng JL, Chen JH, Zhang LW, et al. Lactate dehydrogenase-to-albumin ratio: a superior inflammatory marker for predicting contrast-associated acute kidney injury after percutaneous coronary intervention. Clin Cardiol. 2024;47(2):e 24219.38402549 10.1002/clc.24219 PMC 10823551 · doi ↗ · pubmed ↗
- 8Chu M, Niu H, Yang N, et al. High serum lactate dehydrogenase to albumin ratio is associated with increased risk of poor prognosis after ischemic stroke. Clin Neurol Neurosurg. 2024;237:108120.38266329 10.1016/j.clineuro.2024.108120 · doi ↗ · pubmed ↗