A Tough Pill to Swallow: Demonstration of Esophageal Physiologic Events Explaining Severe Dysphagia Captured on EndoFLIP After LINX Procedure
Shay S. Bidani, Alexandria Iakovidis, Lindsey Creech, Manuel Amaris, David Estores

TL;DR
A patient experienced severe difficulty swallowing after a LINX procedure, and EndoFLIP imaging helped identify the cause and suggest a new treatment approach.
Contribution
The paper demonstrates a novel physiologic approach to treating post-LINX dysphagia by using EndoFLIP to guide dietary changes.
Findings
EndoFLIP showed narrowing and stiffness at lower volumes but improved distensibility at larger volumes.
Ingesting larger solid boluses was suggested as a treatment to improve swallowing.
The approach avoided additional invasive procedures.
Abstract
Dysphagia is a common symptom after magnetic sphincter augmentation, a minimally invasive antireflux alternative to laparoscopic Nissen fundoplication. A 69-year-old woman underwent LINX procedure in 2017 for GERD symptoms, after which she had the onset of dysphagia. EndoFLIP demonstrated narrowing and stiffness at lower volumes but acceptable distensibility at the largest balloon volume. The treatment plan aimed to improve swallowing by ingesting larger solid boluses and avoiding additional invasive procedures. This visualization of the obstruction on EndoFLIP presented a more physiologic approach to treatment with ingesting larger, rather than smaller, solid food boluses.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
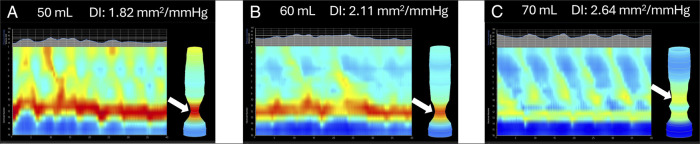 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastroesophageal reflux and treatments · Dysphagia Assessment and Management · Esophageal and GI Pathology
INTRODUCTION
Dysphagia is a common symptom after magnetic sphincter augmentation (MSA), a minimally invasive antireflux alternative to laparoscopic Nissen fundoplication.^1,2^ MSA involves the implantation of a ring-shaped device of titanium beads known as a LINX device around the lower esophageal sphincter to prevent stomach contents from refluxing into the esophagus.^2^ EndoFLIP is an impedance planimetry test done during endoscopy that measures the dimensions of the esophagus, esophageal contractility, and distensibility index (DI) of the esophagogastric junction (EGJ). EndoFLIP after MSA enables calculation of EGJ-DI, which can help determine whether dysphagia results from a restrictive or fibrotic process related to the LINX device versus the expected distensibility of native tissue.^3^ The expected EGJ-DI cutoff is 2 mm^2^/mm Hg at distention volumes of 50 and 60 mL.^4^ Although prior EndoFLIP studies have reported reduced EGJ distensibility using single-volume measurements, we describe, to our knowledge, the first reported instance of EndoFLIP demonstrating a volume-dependent pattern that correlates with the patient's bolus size–dependent symptoms from LINX-related EGJ restriction.^4,5^
CASE REPORT
A 69-year-old woman with a history of gastroesophageal reflux disease (GERD), irritable bowel syndrome with diarrhea, and interstitial cystitis presented with severe dysphagia localized to the bottom quarter of her sternum that occurred at least once daily, as well as regurgitation twice weekly. She self-treated her symptoms with aluminum hydroxide and magnesium carbonate with evening meals. She underwent LINX procedure 7 years prior for GERD symptoms and developed new-onset dysphagia within the following year. She underwent esophagogastroduodenoscopy (EGD) with dilation 1 year after LINX placement, as well as cognitive behavioral therapy with speech-language pathology, which improved her symptoms and allowed her to swallow solid foods again. After her initial dilation, she required 2–3 additional dilations, with her most recent 1–3 years before this visit. Per the patient, her symptoms improved for 1 year after each dilation, but she was lost to follow-up until this presentation.
The patient underwent a timed barium esophagram, revealing a dilated esophagus with residual barium at 1 minute, clearing of barium at the 5-minute mark, and normal passage of a 13-mm barium tablet through the esophagus. Her subsequent EGD showed normal mucosa of the esophagus. High-resolution manometry was not obtained because postoperative changes after MSA can make measurements of lower esophageal sphincter integrated relaxation pressures (LES IRP) and intrabolus pressures (IBP) difficult to interpret. EndoFLIP was instead used to assess EGJ opening and distensibility under graded distention. EndoFLIP demonstrated stiffness at lower volumes, reflected by DI of 1.82 and 2.11 mm^2^/mm Hg at 50 and 60 mL, respectively, but acceptable distensibility at the maximum balloon volume of 70 mL (DI 2.64 mm^2^/mm Hg), indicating adequate opening (Figure 1). Normal contractility was demonstrated by the repetitive antegrade contractions at the highest volume, indicating an acceptable gastroesophageal junction distensibility and opening despite the observed restriction at lower volumes. These findings demonstrate that adequate EGJ opening requires higher distending forces. Therefore, the treatment plan aimed to alleviate symptoms and improve swallowing by ingesting larger solid boluses and allowing a 10-second interval after each swallow. A larger bolus was recommended to increase intraluminal pressure and overcome mechanical restriction from the LINX, thereby mitigating dysphagia symptoms. Avoidance of additional invasive procedures was also recommended. With these recommendations, the patient had improvement in her symptoms.
EndoFLIP demonstrating volume-dependent EGJ narrowing and opening after magnetic sphincter augmentation. Arrows indicate the site of EGJ narrowing. (A) Restricted EGJ opening at 50 mL of saline with a low DI (1.82 mm2/mm Hg), intrabag pressure of 31.1 mm Hg, and a maximum EGJ diameter of 8.50 mm. (B) Partial improvement in EGJ opening at 60 mL of saline (DI 2.11 mm2/mm Hg, 37.9 mm Hg of pressure, and diameter of 10.10 mm). (C) Adequate EGJ opening at 70 mL of saline with preserved repetitive antegrade contractions (DI 2.64 mm2/mm Hg, 67.0 mm Hg of pressure, and diameter of 15.00 mm). These findings illustrate a volume-dependent physiologic response that correlated with the patient's bolus size–dependent dysphagia and guided conservative treatment with larger bolus swallows. DI, distensibility index; EGJ, esophagogastric junction.
DISCUSSION
Up to 67.8% of patients report dysphagia after MSA with a LINX device, with 15.5% reporting long-term symptoms.^3,6^ For patients with persistent dysphagia after MSA, up to 31% undergo endoscopic dilations with an initial success rate of 67%; however, this success rate decreases with repeated procedures.^3^ Roughly 2%–3% of patients with refractory symptoms require device removal with resolution of symptoms ranging from 75% to 100%.^5,7,8^ These invasive postoperative treatments highlight the need for diagnostic tools that can precisely identify the cause of dysphagia and inform targeted treatment strategies that may include avoiding unnecessary operations and complications.
Diagnostic approaches for such cases include the use of EGD, high-resolution manometry, and pH monitoring.^2,3^ Although these tools may provide insight into the pressure dynamics and peristaltic patterns in the esophagus and EGJ, they lack any information on the compliance or distensibility that would help differentiate if the dysphagia is due to mechanical obstruction from the LINX device itself or if it is due to a physiologic abnormality within the patient's EGJ. EndoFLIP offers real-time measurements of the cross-sectional area and pressure in the esophagus thereby allowing calculation of the distensibility index that quantifies EGJ wall compliance. Several studies have explored this in the context of post-MSA dysphagia and demonstrated that a lower DI is associated with dysphagia.^5,9^ Another study used EndoFLIP to optimize the tightness of the device intraoperatively to reduce postoperative dysphagia.^10^ However, these studies focused only on the static measurements by only measuring the DI without correlating the differences in DI at higher FLIP balloon volumes.
Our case addresses this by using various balloon volumes to dynamically correlate EndoFLIP findings with the patient's symptoms, offering a direct physiologic explanation of the patient's symptoms: lower DI at smaller volumes that correlated with the patient's dysphagia with DI normalized at larger volumes. This demonstrates that her dysphagia is volume-dependent and may respond to different strategies for treatment of dysphagia. These findings give clinicians actionable insight, allowing a tailored treatment strategy, such as advising the patient to swallow larger volume solid boluses. In contrast to traditional tools, like EGD, high-resolution manometry, and pH monitoring, which might have prompted repeated dilations or device explanation, EndoFLIP provided a physiologic rationale for a conservative approach, ultimately sparing the patient from further invasive procedures.
Our case highlights the potential for EndoFLIP to refine the diagnostic and treatment approach to post-LINX dysphagia as it offers insights that are not attainable with the more commonly used modalities. EndoFLIP affords an insight into the mechanical and functional causes of dysphagia, which further allows patient-specific treatment strategies and a reduction of unnecessary interventions.
DISCLOSURES
Author contributions: SS Bidani: drafted the initial manuscript, performed primary literature review, contributed to interpretation of case findings, and prepared revisions. A. Iakovidis: drafted the initial manuscript, performed primary literature review, contributed to interpretation of case findings, and prepared revisions. L. Creech: provided manuscript revisions, refined structure, and ensured clarity of presentation. M. Amaris: contributed to case interpretation, reviewed and edited the manuscript for accuracy, and approved the final draft. D. Estores: supervised case interpretation, provided critical revisions, ensured integrity of clinical content, and approved the final manuscript for submission. David Estores is the article guarantor.
Previous presentation: This case report was presented as a poster presentation at the American Neurogastroenterology and Motility Society (ANMS) August 9, 2025 in Minneapolis, MN.
Informed consent was obtained for this case report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bologheanu M Matic A Feka J . Severe dysphagia is rare after magnetic sphincter augmentation. World J Surg. 2022;46(9):2243–50.35486162 10.1007/s 00268-022-06573-2PMC 9334408 · doi ↗ · pubmed ↗
- 2Yadlapati R Gyawali CP Pandolfino JE; CGIT GERD Consensus Conference Participants. AGA clinical practice update on the personalized approach to the evaluation and management of GERD: Expert review. Clin Gastroenterol Hepatol. 2022;20(5):984–94.e 1.35123084 10.1016/j.cgh.2022.01.025PMC 9838103 · doi ↗ · pubmed ↗
- 3Ayazi S Zheng P Zaidi AH . Magnetic sphincter augmentation and postoperative dysphagia: Characterization, clinical risk factors, and management. J Gastrointest Surg. 2020;24(1):39–49.31388888 10.1007/s 11605-019-04331-9PMC 6987054 · doi ↗ · pubmed ↗
- 4Bredenoord AJ Rancati F Lin H Schwartz N Argov M. Normative values for esophageal functional lumen imaging probe measurements: A meta-analysis. Neurogastroenterology Motil. 2022;34(11):e 14419.10.1111/nmo.14419 PMC 978627335665566 · doi ↗ · pubmed ↗
- 5Wu H Attaar M Wong HJ . Impedance planimetry (Endo FLIP™) after magnetic sphincter augmentation (LINX®) compared to fundoplication. Surg Endosc. 2022;36(10):7709–16.35169878 10.1007/s 00464-022-09128-7 · doi ↗ · pubmed ↗
- 6Tsai C Steffen R Kessler U Merki H Lipham J Zehetner J. Postoperative dysphagia following magnetic sphincter augmentation for gastroesophageal reflux disease. Surg Laparosc Endosc Percutan Tech. 2020;30(4):322–6.32282618 10.1097/SLE.0000000000000785 · doi ↗ · pubmed ↗
- 7Poola AS Gatta P. Reoperative surgery after magnetic sphincter augmentation. Dis Esophagus. 2023;36(Supplement_1):doad 024.37317932 10.1093/dote/doad 024 · doi ↗ · pubmed ↗
- 8Tatum JM Alicuben E Bildzukewicz N Samakar K Houghton CC Lipham JC. Removing the magnetic sphincter augmentation device: Operative management and outcomes. Surg Endosc. 2019;33(8):2663–9.30386987 10.1007/s 00464-018-6544-y · doi ↗ · pubmed ↗