Eosinophilic Granulomatosis with Polyangiitis Presenting with Intermittent Claudication
Koichi Bamba, Daisuke Fujishiro, Tomoki Kawahata, Yuki Kamikokura, Tsubasa Ono, Yuta Ikechi, Kitaru Tanaka, Kensaku Okamoto, Yuichi Makino, Hiroshi Nomoto

TL;DR
An 80-year-old woman with EGPA presented with intermittent claudication, highlighting the rare connection between this vasculitis and muscle symptoms.
Contribution
This case report presents a rare manifestation of EGPA as intermittent claudication and emphasizes the role of MRI in diagnosis.
Findings
EGPA can present with intermittent claudication, a symptom typically linked to other conditions.
MRI was effective in identifying muscle inflammation and guiding biopsy in this case.
Treatment with glucocorticoids led to significant clinical improvement in the patient.
Abstract
Intermittent claudication (IC), characterized by lower limb weakness and pain during walking that resolves with rest, is most commonly caused by lumbar spinal canal stenosis or peripheral arterial disease. We report a unique case of eosinophilic granulomatosis with polyangiitis (EGPA) presenting with IC. An 80-year-old woman presented with fever, muscle pain, muscle weakness, and IC. She had a history of bronchial asthma and allergic rhinitis. Laboratory tests revealed eosinophilia (4,212 /μL) and elevated creatine kinase levels (505 U/L). Magnetic resonance imaging (MRI) with short tau inversion recovery sequences demonstrated diffuse high-signal intensity across multiple skeletal muscles. A biopsy specimen of the right biceps brachii, taken from a high-signal area identified on MRI, showed inflammatory cell infiltration, primarily composed of eosinophils and lymphocytes in the blood…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
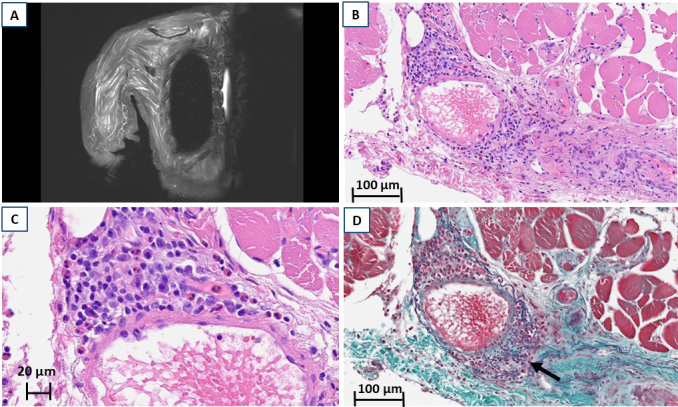 Figure 1
Figure 1| Variable | Reference range | Patient’s value | Measurement unit |
|---|---|---|---|
| Ig G | 861.0 - 1747.0 | 1268.0 | mg/dL |
| Ig A | 93.00 - 393.0 | 291.6 | mg/dL |
| Ig M | 50.00 - 269.0 | 58.4 | mg/dL |
| Ig E | ≤ 232 | 5024 | IU/mL |
| CH50 | 30.00 - 45.0 | 52.3 | U/mL |
| C3 | 73.00 - 138.0 | 104.3 | mg/dL |
| C4 | 11.00 - 31.0 | 25.2 | mg/dL |
| RF-IgM | < 15.0 | 160.9 | IU/mL |
| Anti-CCP Ab | < 4.5 | < 0.5 | U/mL |
| Antinuclear Antibody | < 40 | 40 | Times |
| SPECKLED | < 40 | 40 | Times |
| Anti-ds-DNA Ab | < 10.0 | 2.5 | IU/mL |
| Anti-Sm Ab | < 7.0 | < 7.0 | U/mL |
| Anti-RNP Ab | < 3.5 | < 0.7 | U/mL |
| Anti-SS-A Ab | < 7.0 | 0.7 | U/mL |
| Anti-SS-B Ab | < 7.0 | 0.4 | U/mL |
| Anti-topoisomerase I Ab | < 10.0 | 5.9 | U/mL |
| PR3-ANCA | < 2.0 | < 1.0 | U/mL |
| MPO-ANCA | < 3.5 | < 1.0 | U/mL |
| Anti-ARS Ab | < 25.0 | < 5.0 | Index |
| Anti-TIF1-γAb | < 32 | < 5 | index |
| Anti-Mi-2 Ab | < 53 | < 5 | index |
| Anti-MDA-5 Ab | < 32 | < 4 | index |
| AMA-M2 | < 7.0 | 1.8 | index |
| Case | Age (years) | Sex | Clinical symptoms | MPO-ANCA | PR3-ANCA | Diagnosis | Authors | Year | Publisher |
|---|---|---|---|---|---|---|---|---|---|
| Present case | 80 | F | Bronchial asthma, allergic rhinitis, muscle pain and weakness in the limbs, IC | Negative | Negative | EGPA | ー | ー | ー |
| 1 | 69 | M | Bronchial asthma, fever, IC, toe ulcers | Negative | Negative | EGPA | Inui S, Itami S, Iwai C, Yoshikawa K | 2001 |
|
| 2 | 75 | M | Muscle pain in both lower legs, IC, fever, dyspnea, renal impairment | 761.0 AAU | Negative | GPA | Kim MY, Bae SY, Lee M, et al | 2012 |
|
| 3 | 65 | F | Fever, difficulty breathing, blood in the sputum, pain in both lower legs, IC | 122.04 U/ml | Negative | MPA | Liao Z-H, Feng JT, Tang J-L, et al | 2021 |
|
| 4 | 61 | M | IC, right leg drop, muscle weakness in both legs, sensory disturbance in both legs, cerebral infarction | 140 U/mL | N/A | MPA | Ando T, Watanabe H, Riku Y, et al | 2023 |
|
| 5 | 70 | M | IC, fever, purpura | 32.9 U/mL | N/A | MPA | Ishizuka K, Ohira Y | 2023 |
|
| Case | Age (years) | Sex | Clinical symptoms | CK (U/L) | MPO-ANCA (U/mL) | PR3-ANCA (U/mL) | MRI | Authors | Year | Publisher |
|---|---|---|---|---|---|---|---|---|---|---|
| Present case | 80 | F | Muscle pain and weakness in the limbs, intermittent claudication, BA, allergic rhinitis, | 505 | Negative | Negative | Diffuse high signal intensity in the muscles of both upper limbs, shoulders, and lower limbs on STIR sequences | ー | ー | ー |
| 1 | 50 | F | Muscle pain and weakness in both lower limbs, BA, numbness in the soles of both feet | 930 | N/A | N/A | N/A | Kawaguchi R, Okayama K, Handa Y, et al | 1989 |
|
| 2 | 81 | M | Muscle pain and weakness in both upper and lower limbs, BA, nasal polyps | 538 | 42.1 | Negative | N/A | Suresh E, Dhillon VB, Smith C, Ironside JW | 2004 |
|
| 3 | 57 | M | Generalized muscle pain, abnormal sensation in the arm, sinusitis, chronic bronchitis | 4,454 | 57.6 | Negative | N/A | Lazzarin P, Presotto F, Polo A | 2009 |
|
| 4 | 68 | F | Muscle pain and weakness in both lower limbs, fever, BA, sinusitis, hemorrhagic blisters | 1,076 | 640 | Negative | N/A | Uehara M, Hashimoto T, Sasahara E, et al | 2009 |
|
| 5 | 71 | M | Muscle pain and weakness in the lower limbs, edema, BA, nasal polyps | 2,245 | 132 | Negative | No abnormal findings | Tutor-Ureta P, Martín Jiménez ML, Bellas C, et al | 2011 |
|
| 6 | 74 | M | Generalized muscle pain, forehead claudication, fever, BA | 3,708 | Negative | Negative | Diffuse high signal intensity in the muscles of both lower limbs and mild muscle atrophy on STIR sequences | Parent M-E, Larue S, Ellezam B | 2014 |
|
| 7 | 64 | M | Muscle weakness in both lower legs, BA, sinusitis, purpura in both lower legs | 2,204 | 168 | Negative | N/A | Lim G, Lim S, Tee S-I, Ling CY | 2019 |
|
| 8 | 78 | M | Muscle pain and weakness in both lower limbs, fever, BA | 559 | Positive | N/A | Diffuse high signal intensity in the muscles of both lower limbs on T2WI | Woo K, Park YE, Jeon D, Shin JH | 2020 |
|
| 9 | 82 | F | Muscle weakness in both upper and lower limbs, dysphagia, dyspnea | 2,627 | >200 | N/A | Diffuse high signal intensity in the muscles of both lower limbs and mild muscle atrophy on T2WI | Koppikar S, Al-Dabie G, Jerome D, Vinik O | 2020 |
|
| 10 | 75 | M | Muscle pain and weakness in the lower limbs, fever | 632 | Negative | Negative | Diffuse high signal intensity in both thigh muscles on STIR sequences | Ueta Y, Akiba Y, Yamazaki J, et al | 2020 |
|
| 11 | 57 | M | Muscle pain and weakness in the upper and lower limbs, sensory disturbance in both hands | 1,040 | > 200 | Negative | N/A | Aykac S, Yuceyar AN, Akalın T, Colakoglu Z | 2023 |
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Eosinophilic Disorders and Syndromes · Peripheral Artery Disease Management
Introduction
Eosinophilic granulomatosis with polyangiitis (EGPA) is a type of anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis characterized by systemic necrotizing vasculitis and eosinophilic infiltration in patients with asthma or allergic rhinitis ^(1), (2)^. EGPA frequently causes muscle pain and weakness; however, intermittent claudication (IC) is rare. Here, we describe a case of EGPA presenting with IC and skeletal muscle damage, in which magnetic resonance imaging (MRI) helped identify the biopsy site for diagnosis.
Case Report
An 80-year-old woman with a history of bronchial asthma and allergic rhinitis experienced muscle pain in both thighs three months before admission, which later spread to her shoulders and upper arms. She developed a fever of 38°C and IC. A few days later, she presented to our emergency department with muscle weakness, primarily affecting both lower legs, and was admitted.
On physical examination, she had spontaneous pain and tenderness in the biceps, triceps, and quadriceps bilaterally. Manual muscle testing yielded a score of four in both the upper and lower limbs. She had no abdominal pain or rash, and the bilateral dorsalis pedis arteries were palpable. Her IC was unaffected by postural changes, and she could walk only approximately 6 m because of leg pain.
Laboratory tests revealed eosinophilia (4,212 /μL), elevated creatine kinase levels (CK, 505 U/L), C-reactive protein (2.25 mg/dL), and immunoglobulin E (5,024 IU/mL). CK-myoglobin, electrolytes, and thyroid function were normal. As summarized in Table 1, immunological tests showed weakly positive antinuclear antibodies (speckled pattern, 1:40), while all disease-specific autoantibodies were negative. Rheumatoid factor was positive (160.9 IU/mL); however, the absence of joint symptoms and the lack of inflammatory findings on joint ultrasonography made rheumatoid arthritis unlikely.
MRI with short tau inversion recovery sequences demonstrated diffuse high-signal intensity in the muscles of both upper limbs, shoulders, and lower limbs (Figure 1A). A biopsy specimen from the right biceps brachii, identified as a high-signal area on MRI, showed inflammatory cell infiltration, predominantly eosinophils and lymphocytes, within the arterial walls (Figure 1B and 1C). Elastica Masson staining revealed disruption of the external elastic lamina and perivascular collagen fiber proliferation (Figure 1D).
MRI and pathology.(A) MRI with short tau inversion recovery sequences of the right upper arm shows high signal intensity in the skeletal muscle. (B, C) H & E staining of the right biceps brachii reveals inflammatory cell infiltration, predominantly eosinophils and lymphocytes, within the walls of arteries. (D) Elastica Masson staining of the right biceps brachii; the arrow indicates a disruption of the external elastic lamina, with proliferation of collagen fibers surrounding the blood vessels.H & E: hematoxylin-eosin; MRI: magnetic resonance imaging.
She had no history of lifestyle-related disease or smoking. Based on her clinical history, fever, muscle pain, eosinophilia, MRI findings, and histology, she was diagnosed with EGPA and associated skeletal muscle involvement. To evaluate possible comorbidities, we performed a non-contrast computed tomography (CT) scan, which showed no comorbidities, including calcification in the aorta or lower-limb arteries.
Treatment with prednisolone 20 mg/day (0.5 mg/kg/day) led to rapid improvement. By day six, she was able to walk 12 m; by day 10, 30 m; and by day 12, she could ascend and descend stairs without difficulty.
Discussion
This is the second reported case of EGPA with IC. Among the five reported cases of ANCA-associated vasculitis presenting with IC (Table 2), only one was diagnosed as EGPA ^(3)^. In the present case, histology revealed inflammatory cell infiltration in the vascular walls surrounding the skeletal muscle, suggesting ischemia due to necrotizing vasculitis.
IC is typically caused by peripheral arterial disease ^(4)^ or spinal canal stenosis ^(5)^ and is rarely attributed to vasculitis. In elderly patients, distinguishing EGPA-related IC from atherosclerosis is crucial. In this patient, the absence of atherosclerotic risk factors, the presence of palpable peripheral pulses, no vascular calcification on CT, and rapid and dramatic improvement with corticosteroid therapy suggested that atherosclerosis was unlikely. While non-contrast CT is not standard for evaluating peripheral vascular disease, it was used here to screen for comorbidities. We acknowledge the lack of angiography as a limitation, as small-vessel peripheral vascular disease cannot be completely ruled out. However, the rapid therapeutic response strongly supports vasculitis as the cause of IC.
Pain at rest raised the possibility of myositis; however, histopathology showed no inflammation within muscle fibers or the perimysium, ruling out true inflammatory myopathy. Muscle pain was likely due to ischemia and perivascular inflammation.
In this case, MRI played a pivotal role by identifying high-signal areas for biopsy. In a cohort study, muscle pain was reported in 40% of myeloperoxidase-ANCA-positive and 17.2% of myeloperoxidase-ANCA-negative EGPA cases ^(6)^. However, few reports have described skeletal muscle involvement in patients with elevated CK. Table 3 summarizes 11 EGPA cases with elevated CK, five of which used MRI; this is the first case in which biopsy of an MRI finding confirmed vasculitis.
While MRI is widely used in inflammatory myopathies ^(7), (8), (9)^, its role in EGPA-associated muscle damage remains to be established.
In conclusion, EGPA should be considered in the differential diagnosis of patients presenting with IC, particularly when systemic signs such as fever, eosinophilia, and asthma are present. MRI may help detect muscle involvement, guide biopsy site selection, and facilitate timely diagnosis and treatment of EGPA-associated muscle damage.
Article Information
Acknowledgements
We would like to thank Editage (www.editage.jp) for English language editing.
Authors Contributions
Conception, data acquisition, analysis, interpretation of data for the work, and drafting: Koichi Bamba. Pathology imaging, figure preparation, and interpretation of the pathology: Yuki Kamikokura. Provided substantial contribution to interpretation of data for the work and revised it critically: Daisuke Fujishiro, Tomoki Kawahata, Tsubasa Ono, Yuta Ikechi, Kitaru Tanaka, Kensaku Okamoto, Yuichi Makino, and Hiroshi Nomoto. All authors substantially contributed to the revision of the manuscript drafts. Manuscript revision and final approval: All authors.
Conflicts of Interest
None
IRB Approval Code and Name of the Institution
According to the guidelines of the Institutional Review Board of Asahikawa Medical University, formal ethical approval was not required for a single case report.
Informed Consent
Written informed consent for publication was obtained from the patient.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Emmi G, Bettiol A, Gelain E, et al. Evidence-based guideline for the diagnosis and management of eosinophilic granulomatosis with polyangiitis. Nat Rev Rheumatol. 2023;19(6):378-93.37161084 10.1038/s 41584-023-00958-w · doi ↗ · pubmed ↗
- 2White J, Dubey S. Eosinophilic granulomatosis with polyangiitis: a review. Autoimmun Rev. 2023;22(1):103219.36283646 10.1016/j.autrev.2022.103219 · doi ↗ · pubmed ↗
- 3Inui S, Itami S, Iwai C, et al. Churg-Strauss syndrome involving medium-sized arteries. J Dermatol. 2001;28(3):161-4.11349469 10.1111/j.1346-8138.2001.tb 00112.x · doi ↗ · pubmed ↗
- 4Moras E, Khan MI, Song DD, et al. Pharmacotherapy and revascularization strategies of peripheral artery disease. Curr Probl Cardiol. 2024;49(4):102430.38309544 10.1016/j.cpcardiol.2024.102430 · doi ↗ · pubmed ↗
- 5Genevay S, Atlas SJ. Lumbar spinal stenosis. Best Pract Res Clin Rheumatol. 2010;24(2):253-65.20227646 10.1016/j.berh.2009.11.001PMC 2841052 · doi ↗ · pubmed ↗
- 6Liu S, Han L, Liu Y, et al. Clinical significance of MPO-ANCA in eosinophilic granulomatosis with polyangiitis: experience from a longitudinal Chinese cohort. Front Immunol. 2022;13:885198.35833130 10.3389/fimmu.2022.885198 PMC 9271578 · doi ↗ · pubmed ↗
- 7Del Grande F, Carrino JA, Del Grande M, et al. Magnetic resonance imaging of inflammatory myopathies. Top Magn Reson Imaging. 2011;22(2):39-43.22648079 10.1097/RMR.0b 013e 31825 b 2c 35 · doi ↗ · pubmed ↗
- 8Schmidt J. Current classification and management of inflammatory myopathies. J Neuromuscul Dis. 2018;5(2):109-29.29865091 10.3233/JND-180308 PMC 6004913 · doi ↗ · pubmed ↗