Screening for Psychological Distress, Disaster-Related Experiences, and Newly Developed Mental Disorders among Residents Affected by the Great East Japan Earthquake: Implications for Suicide Prevention
Masatsugu Orui, Mana Kogure, Yuka Kotozaki, Taku Obara, Mami Ishikuro, Aoi Noda, Genki Shinoda, Keiko Murakami, Hirohito Metoki, Masahiro Kikuya, Yoshitake Takebayashi, Masaharu Maeda, Naoki Nakaya, Kozo Tanno, Atsushi Hozawa, Shinichi Kuriyama

TL;DR
This study shows that combining the K6 psychological distress scale with factors like PTSD and income loss improves suicide risk prediction after disasters.
Contribution
The study identifies specific factors that enhance the K6 scale's accuracy in predicting suicide after disasters.
Findings
Combining K6 with PTSD and income loss improved suicide prediction accuracy.
Disaster-related stress symptoms increased the predictive power of the K6 scale.
The K6 alone had lower accuracy compared to combinations with other factors.
Abstract
This study aimed to evaluate the accuracy of screening using the six-item Kessler Psychological Distress Scale (K6) for suicide death after the Great East Japan Earthquake (GEJE) in combination with binge drinking, diagnosed history of mental disorders, disaster-related experiences, disaster stress symptoms, sleep status, and social network, which were used in the practical settings of disaster-related mental health services. This prospective cohort study spanned the period from 2013 to 2021. Among the Tohoku Medical Megabank Project sample, 27,335 affected residents and 61,157 residents living within the disaster-stricken area (i.e., those who experienced partial or no house damage and did not evacuate even if they lived in the disaster-stricken area) of the GEJE were analyzed using receiver operating characteristic curve (ROC) analyses of the K6 score in combination with the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1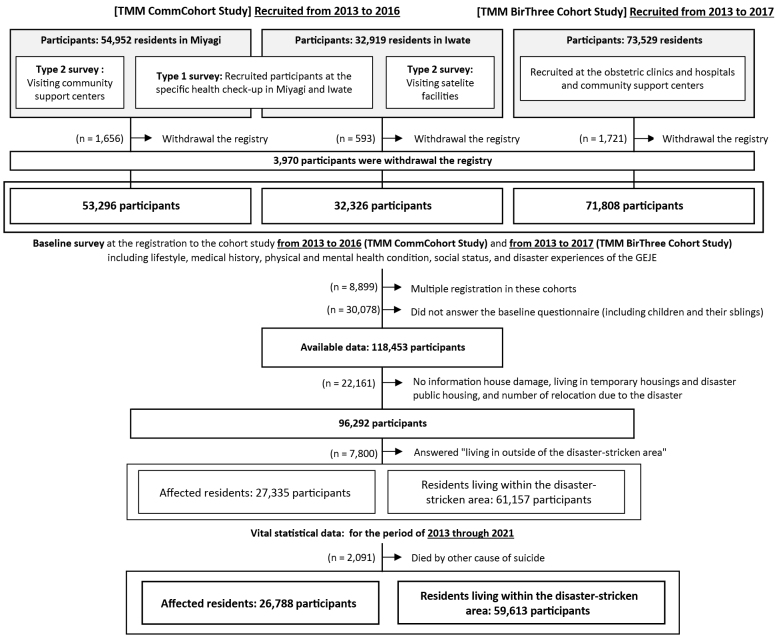 Figure 2
Figure 2| Affected residents | Residents living within the disaster-stricken area | ||||
|---|---|---|---|---|---|
| (n=27,335) | (%) | (n=61,157) | (%) | ||
| Sex | men | 11,932 | (43.7) | 23,962 | (39.2) |
| women | 15,403 | (56.3) | 37,195 | (60.8) | |
| Age group | 18-39 | 6,998 | (25.6) | 6,232 | (10.2) |
| 40-64 | 11,943 | (43.7) | 30,392 | (49.7) | |
| ≥65 years | 8,394 | (30.7) | 24,533 | (40.1) | |
| Educational attainment | junior/high school | 16,245 | (60.1) | 39,838 | (66.0) |
| vocational school/junior college | 6,563 | (24.3) | 13,878 | (23.0) | |
| university/graduate school | 4,243 | (15.7) | 6,622 | (11.0) | |
| Marital status | married | 21,365 | (79.0) | 49,101 | (81.2) |
| unmarried/divorced/bereaved | 5,691 | (21.0) | 11,366 | (18.8) | |
| Psychological distress (K6 score) | 0-4 points | 14,429 | (53.0) | 37,157 | (61.1) |
| 5-12 points | 10,602 | (38.9) | 20,328 | (33.4) | |
| ≥13 points | 2,189 | (8.0) | 3,348 | (5.5) | |
| Binge drinking | more than 6 drinks/day and every day | 1,115 | (4.1) | 2,294 | (3.8) |
| Social networks (LSNS-6) | ≤11 points | 6,799 | (25.8) | 14,553 | (24.8) |
| Sleep problems (AIS) | ≥6 points | 7,035 | (25.8) | 13,138 | (21.5) |
| History of diagnosed mental disorders | depression developed pre-disaster | 645 | (2.4) | 1,330 | (2.2) |
| depression newly developed after the GEJE | 310 | (1.1) | 312 | (0.5) | |
| PTSD developed pre-disaster | 49 | (0.2) | 81 | (0.1) | |
| PTSD newly developed after the GEJE | 224 | (0.8) | 125 | (0.2) | |
| Disaster experiences | loss of a family member | 1,525 | (5.8) | 916 | (1.6) |
| loss of relatives | 7,580 | (28.8) | 10,231 | (17.5) | |
| loss of friends | 5,830 | (22.1) | 7,219 | (12.3) | |
| Changes in income after the GEJE | increased in income/no change | 11,190 | (67.0) | 23,997 | (72.4) |
| decreased income | 5,504 | (33.0) | 9,141 | (27.6) | |
| Disaster-related stress symptoms | recollection of disaster experiences | 3,721 | (14.0) | 3,963 | (6.7) |
| physical reactions due to recalling the disaster | 1,659 | (6.2) | 1,842 | (3.1) | |
| Number of suicide cases | Total number (2013 through 2021) | 26 | 41 | ||
| /100,000 participants (annualized) | 10.8 | 7.6 | |||
| Affected residents | Residents living within the disaster-stricken area | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Suicide death (+) | Suicide death (-) | Suicide death (+) | Suicide death (-) | ||||||
| (n=26) | (%) | (n=26,762) | (%) | (n=41) | (%) | (n=59,572) | (%) | ||
| Sex | men | 19 | (0.16) | 11,577 | (99.84) | 25 | (0.11) | 22,925 | (99.89) |
| women | 7 | (0.05) | 15,185 | (99.95) | 16 | (0.04) | 36,647 | (99.96) | |
| Age group | 18-39 | 5 | (0.07) | 6,985 | (99.93) | 7 | (0.11) | 6,213 | (99.89) |
| 40-64 | 13 | (0.11) | 11,782 | (99.89) | 22 | (0.07) | 29,938 | (99.93) | |
| ≥65 years | 8 | (0.10) | 7,995 | (99.90) | 12 | (0.05) | 23,421 | (99.95) | |
| Educational attainment | junior/high school | 12 | (0.08) | 15,835 | (99.92) | 27 | (0.07) | 38,667 | (99.93) |
| vocational school/junior college | 5 | (0.08) | 6,473 | (99.92) | 6 | (0.04) | 13,661 | (99.96) | |
| university/graduate school | 9 | (0.21) | 4,180 | (99.79) | 8 | (0.12) | 6,456 | (99.88) | |
| Marital status | married | 19 | (0.09) | 20,951 | (99.91) | 29 | (0.06) | 47,869 | (99.94) |
| unmarried/divorced/bereaved | 6 | (0.11) | 5,544 | (99.89) | 12 | (0.11) | 11,045 | (99.89) | |
| Psychological distress (K6) | 0-4 points | 7 | (0.05) | 14,129 | (99.95) | 15 | (0.04) | 36,156 | (99.96) |
| 5-12 points | 13 | (0.13) | 10,380 | (99.87) | 16 | (0.08) | 19,828 | (99.92) | |
| ≥13 points | 6 | (0.28) | 2,144 | (99.72) | 10 | (0.30) | 3,275 | (99.70) | |
| Binge drinking | more than 6 drinks/day and every day | 1 | (0.09) | 1,080 | (99.91) | 4 | (0.18) | 2,209 | (99.82) |
| Social networks (LSNS-6) | ≤11 points | 11 | (0.17) | 6,643 | (99.83) | 17 | (0.12) | 14,139 | (99.88) |
| Sleep problems (AIS) | ≥6 points | 13 | (0.19) | 6,880 | (99.81) | 17 | (0.13) | 12,802 | (99.87) |
| History of diagnosed mental disorders | depression developed pre-disaster | 5 | (0.80) | 622 | (99.20) | 8 | (0.62) | 1,286 | (99.38) |
| depression newly developed after the GEJE | 2 | (0.66) | 301 | (99.34) | 1 | (0.33) | 306 | (99.67) | |
| PTSD developed pre-disaster | 1 | (2.08) | 47 | (97.92) | 0 | (0.0) | 80 | (100.0) | |
| PTSD newly developed after the GEJE | 3 | (1.40) | 211 | (98.60) | 0 | (0.0) | 119 | (100.0) | |
| Disaster experiences | loss of a family member | 1 | (0.07) | 1,493 | (99.93) | 1 | (0.11) | 886 | (99.89) |
| loss of relatives | 8 | (0.11) | 7,380 | (99.89) | 10 | (0.10) | 9,939 | (99.90) | |
| loss of friends | 8 | (0.14) | 5,655 | (99.86) | 5 | (0.07) | 6,997 | (99.93) | |
| Changes in income after the GEJE | decreased income | 7 | (0.13) | 5,398 | (99.87) | 9 | (0.10) | 8,926 | (99.90) |
| Disaster-related stress symptoms | recollection of disaster experiences | 5 | (0.14) | 3,611 | (99.86) | 5 | (0.13) | 3,827 | (99.87) |
| physical reactions due to recalling the disaster | 5 | (0.31) | 1,609 | (99.69) | 2 | (0.11) | 1,802 | (99.89) | |
| Affected residents (n=26,788) | Residents living within the disaster-stricken area (n=59,613) | ||||||
|---|---|---|---|---|---|---|---|
| OR* | (95% CI) | p-value | OR* | (95% CI) | p-Value | ||
| Psychological distress (K6) | 5-12 points | 2.688 | (1.051-6.877) | 0.039 | 2.042 | (1.002-4.160) | 0.049 |
| ≥13 points | 7.718 | (2.226-23.59) | <0.001 | 7.552 | (3.268-17.45) | <0.001 | |
| Binge drinking | more than 6 drinks/day and every day | 0.680 | (0.090-5.139) | 0.709 | 1.912 | (0.663-5.514) | 0.231 |
| Social networks (LSNS-6) | ≤11 points | 2.144 | (0.945-4.867) | 0.068 | 2.086 | (1.096-3.969) | 0.025 |
| Sleep problems (AIS) | ≥6 points | 3.630 | (1.643-8.020) | 0.001 | 3.030 | (1.597-5.750) | 0.001 |
| History of diagnosed mental disorders | depression developed pre-disaster | 7.986 | (2.667-23.92) | <0.001 | 10.38 | (4.710-22.86) | <0.001 |
| depression newly developed after the GEJE | 9.906 | (2.272-43.19) | 0.002 | 5.036 | (0.683-37.15) | 0.113 | |
| PTSD developed pre-disaster | 28.50 | (3.557-228.4) | 0.002 | - | - | - | |
| PTSD newly developed after the GEJE | 20.96 | (6.050-72.62) | <0.001 | - | - | - | |
| Disaster experiences | loss of a family member | 0.736 | (0.097-5.581) | 0.767 | 1.781 | (0.243-13.03) | 0.570 |
| loss of relatives | 1.640 | (0.665-4.042) | 0.283 | 1.963 | (0.947-4.068) | 0.070 | |
| loss of friends | 1.700 | (0.678-4.262) | 0.258 | 1.131 | (0.440-2.907) | 0.798 | |
| Changes in income after the GEJE | decreased income | 1.277 | (0.431-3.781) | 0.659 | 2.191 | (0.906-5.301) | 0.082 |
| Disaster-related stress symptoms | recollection of disaster experiences | 2.178 | (0.789-6.012) | 0.133 | 2.364 | (0.917-6.091) | 0.075 |
| physical reactions due to recalling the disaster | 6.043 | (2.217-16.86) | 0.001 | 1.937 | (0.462-8.113) | 0.366 | |
| Affected residents (n = 26,788) | Residents living within the disaster-stricken area (n = 59,613) | ||||||
|---|---|---|---|---|---|---|---|
| AUC | (95% CI) | p-Value | AUC | (95% CI) | p-Value | ||
| K6 score alone | 0.681 | (0.567-0.794) | - | 0.699 | (0.602-0.882) | - | |
| K6 with binge drinking | more than 6 drinks/day and every day | - | - | - | 0.728 | (0.394-1.000) | 0.833 |
| K6 with social networks | LSNS-6 ≤11 points | 0.627 | (0.447-0.805) | 0.457 | 0.613 | (0.168-0.7308) | 0.107 |
| K6 with sleep problems | AIS ≥6 points | 0.702 | (0.555-0.849) | 0.319 | 0.758 | (0.644-0.873) | 0.117 |
| K6 with diagnosed mental disorders | depression developed pre-disaster | 0.720 | (0.474-0.966) | 0.566 | 0.695 | (0.517-0.874) | 0.696 |
| depression newly developed after the GEJE | 0.773 | (0.377-1.000) | 0.509 | - | - | - | |
| PTSD developed pre-disaster | - | - | - | - | - | - | |
| PTSD newly developed after the GEJE | 0.878 | (0.773-0.982) | 0.004 | - | - | - | |
| K6 with disaster experiences | loss of a family member | - | - | - | - | - | - |
| loss of relatives | 0.746 | (0.601-0.890) | 0.245 | 0.692 | (0.506-0.877) | 0.997 | |
| loss of friends | 0.721 | (0.519-0.922) | 0.468 | 0.836 | (0.675-0.997) | 0.078 | |
| K6 with changes in income after the GEJE | decreased income | 0.835 | (0.726-0.945) | 0.014 | 0.699 | (0.504-0.894) | 0.729 |
| K6 with disaster-related stress symptoms | recollection of disaster experiences | 0.849 | (0.714-0.985) | 0.020 | 0.866 | (0.779-0.952) | 0.005 |
| physical reactions due to recalling the disaster | 0.780 | (0.589-0.970) | 0.165 | 0.969 | (0.958-0.981) | <0.001 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPosttraumatic Stress Disorder Research · Suicide and Self-Harm Studies · Disaster Response and Management
Introduction
Devastating natural disasters and their aftermaths are known to cause psychological distress in the individuals affected, which can lead to suicidality ^(1), (2)^. The 2011 Great East Japan Earthquake (GEJE) undoubtedly had a severe impact on mental health among those affected ^(3), (4), (5), (6), (7), (8), (9)^. Against this backdrop, our earlier research revealed that the GEJE was followed by an increase in suicide rates in the disaster-stricken area ^(10), (11), (12)^. After the GEJE, disaster-related mental health services, such as psychological first aid, screening for individuals requiring observation or support, and counseling services, were offered early in the post-disaster period to address the broad mental health impacts among affected residents, thereby helping to prevent suicide ^(13), (14), (15), (16), (17)^.
In disaster mental health activities after the GEJE, the six-item Kessler Psychological Distress Scale (K6) ^(18), (19)^―a widely used screening checklist for identifying individuals at high risk―was used extensively in practical settings (e.g., K6 score ≥13 is defined as an individual at high risk) ^(20), (21)^. Mental health screening has been conducted using K6 in accordance with Japan’s disaster-related mental health guidelines ^(22), (23)^, which is also used to screen for suicidality ^(24)^.
A previous study found both severe and moderate psychological distress to be associated with an increased risk of suicide death among the Japanese general population during a non-disaster phase ^(25)^. This finding indicates that a certain number of suicide cases occur even among those whose K6 scores are lower than 13 points ^(25)^; therefore, relying solely on K6 screening may not be ideal for suicide prevention after disasters. Thus, other checklists that evaluate related factors, such as binge drinking, disaster-related experiences, traumatic stress, and history of mental disorders, are also used as important screening tools in disaster-related mental health services in Japan ^(20), (21)^.
However, simply evaluating K6 scores including other related factors―binge drinking, disaster-related experiences, traumatic stress, and history of mental disorders―is not sufficient among residents affected by disasters to determine whether these screening efforts can prevent suicide death after disasters. To our knowledge, no studies have yet been reported that examine the accuracy of suicide death screening using the K6 score among residents affected by disasters. Therefore, to generate solid evidence for suicide prevention after disasters, we aimed to evaluate the accuracy of screening for suicide death after the GEJE using the K6―alongside assessing for binge drinking, disaster-related experiences, traumatic stress, and newly developed mental disorders―in a large-scale cohort study established after the GEJE. We hypothesized that (1) screening for suicide prevention through K6 alone would not be sufficiently accurate and that (2) screening using K6 in conjunction with assessments of binge drinking, disaster experiences, disaster-related stress symptoms, and newly developed mental disorders would be more accurate than using K6 alone.
Methods
Disaster-related mental health services after the GEJE
According to the Japanese Fire and Disaster Management Agency, the GEJE disaster led to 15,844 deaths, with more than 90% of the deaths attributed to drowning due to a massive tsunami ^(26)^.
After the GEJE, disaster-related mental health services were conducted from an early stage across multiple settings―such as shelters, temporary housing, and post-disaster public housing―in the disaster-stricken area, which have been primarily organized by the prefectural government. These services aimed to support affected residents, alleviate psychological distress, and prevent suicide. Screening to identify individuals at high risk of mental health problems plays a crucial role in these disaster-related services. When residents are recognized as being in a high-risk mental health state, public health nurses or other health professionals reach out to provide counseling and other forms of psychological support; if necessary, the residents are referred to specialized institutions. These disaster-related mental health services are modeled on suicide prevention activities that have been performed in the non-disaster phase for communities in Niigata and Akita prefectures, which have been evaluated for the effectiveness of suicide prevention ^(27), (28)^.
Study design and linkage of death data of vital statistics
This is a prospective cohort study. The Tohoku Medical Megabank Project (TMM) began in 2013 with the aim of assisting medical and health services in overcoming the damage from the GEJE by supporting survivors and implementing personalized health care. The TMM encompasses two prospective cohort studies in Miyagi and Iwate prefectures. One is a population-based adult cohort study―the TMM Community-Based Cohort Study (TMM CommCohort Study)―in which more than 80,000 residents aged 20 to 74 years were recruited from 2013 to 2016. The other cohort study is a birth and three-generation cohort study―the TMM Birth and Three-Generation Cohort Study (TMM BirThree Cohort Study)―which recruited more than 70,000 residents from 2013 to 2017 by first enrolling pregnant women at obstetric clinics or hospitals, along with their children, partners, parents, and extended family members.
The regions targeted by these two cohorts are shown in Figure 1. They include all 35 municipalities in Miyagi Prefecture and 20 municipalities (Miyako City, Ofunato City, Kuji City, Tono City, Ichinoseki City, Rikuzen-Takata City, Kamaishi City, Ninohe City, Yahaba town, Sumita town, Otsuchi town, Yamada town, Iwaizumi town, Tanohata village, Fudai village, Karumai town, Noda village, Kunohe village, Hirono town, and Ichinohe town) in Iwate Prefecture ^(29)^.
Municipalities in Iwate Prefecture and Miyagi Prefecture.
To link death data from Japan’s Ministry of Health, Labour, and Welfare, we gathered extensive vital statistical data for the period of 2013 through 2021, which encompassed data regarding age, sex, address, dates of birth and death, and cause of death. Subsequently, we matched cohort participants on the basis of these variables to determine causes of death.
Outcome
In this study, the outcome set suicide death. We defined suicide death among the cohort participants using the International Classification of Diseases, 10th Revision, codes X60-84.
Study period
This study period was set from 2013 to 2021. Given participants in these cohort studies were registered in 2013 or later, this study targeted the mid- to long-term and recovery phases after the GEJE. It should be noted that the participants’ lifestyles, social networks, socioeconomic statuses, and mental health statuses did not reflect the immediate aftermath of the GEJE.
Participants
The participants in the two cohort studies are presented in Figure 2. The TMM CommCohort Study enrolled 54,952 participants in Miyagi, and 32,326 participants in Iwate. The TMM BirThree Cohort Study enrolled 73,529 participants. Among participants in the TMM CommCohort study and the TMM BirThree Cohort study, 3,970 withdrew their registration as of December 2023. A total of 8,899 participants were enrolled in both cohorts, and 30,078 participants did not complete the baseline questionnaire. As a result, 118,453 participants had baseline questionnaire data available for analysis. We excluded 22,161 participants owing to missing information on (1) house damage caused by the GEJE, (2) whether they lived in temporary or post-disaster public housing, and (3) the number of evacuations they experienced owing to the GEJE, and excluded those who answered, “living outside of the disaster-stricken area.”
Participants in the TMM CommCohort Study and BirThree Cohort Study and subjects analyzed.TMM: Tohoku Medical Megabank Project.
In this study, we defined “affected residents” as participants who had experienced house damage (totally destroyed, mostly destroyed, or half destroyed), lived in temporary or post-disaster public housing, and evacuated to shelters at least once (n = 27,335). Those who experienced partial or no house damage and no evacuations, even if they lived in the disaster-stricken area, were classified as “residents living within the disaster-stricken area” (n = 61,157).
Measurements
At the baseline survey, we collected the following demographic and disaster-related variables: sex (men, women), age group (18-39, 40-64, and ≥65 years), educational attainment (junior/high school, vocational school/junior college, and university/graduate school), marital status (married or unmarried/divorced/bereaved), housing damage due to the GEJE (totally destroyed, mostly destroyed, half destroyed, partially destroyed, not destroyed, or did not live in the disaster-stricken area), living conditions (whether residing in temporary or post-disaster public housing), and the number of evacuations to shelters or temporary housing.
Besides, the following variables collected at the baseline survey―psychological distress, binge drinking, disaster experiences, disaster-related stress symptoms, diagnosed mental history of disorders, sleep status, and social network―were selected as related variables because they were used commonly in practical settings in disaster-related mental health activities ^(16), (20)^. Furthermore, these variables have been identified as risk factors for suicide ideation in previous studies on disaster-related mental health ^(30), (31), (32), (33), (34), (35)^.
Psychological distress (K6)
We used the K6 scale to assess current psychological distress. The K6 scale screens for non-specific serious mental illnesses, including Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition mood and anxiety disorders, indicating psychological distress within the past 30 days. Scores on the K6 range from 0 to 24 points. A score of 0-4 points indicates probable absence of psychological distress; 5-12 points indicates probable mild-to-moderate distress, and 13 points or more indicates serious psychological distress ^(18)^. This study used the Japanese version of the K6 scale, which has been empirically validated as an independent screening tool for mental distress ^(19)^.
Binge drinking
Participants were asked the following questions about their drinking habits: “Do you drink alcohol more than once a month?” and “If you are a drinker, what kind of alcohol and how much do you drink on a typical drinking day?” We then defined “binge drinkers” based on the frequency of drinking and the amount of alcohol consumed on a typical drinking day. “Binge drinking” was defined as drinking alcohol every day and consuming more than six drinks per day (≥66 g of ethanol per day). “Six drinks” was defined as 180 mL of spirits (e.g., whiskey or brandy), 600 mL of wine, 1,500 mL of beer, or 540 mL of Japanese sake ^(36), (37)^.
Disaster experiences and disaster-related stress symptoms
We assessed participants’ disaster experiences by asking whether any family, relatives, or friends died or went missing because of the GEJE. To evaluate changes in income after the GEJE, we asked participants whether they had changed their income, offering three response options: “increased income,” “decreased income,” or “no change.”
We also assessed disaster-related stress symptoms using investigator-designed queries: “Do you recall or dream about the disaster, even if you would prefer not to?” (recollection of disaster experiences) and “Do you have any physical reactions when you think about the disasters (e.g., heart palpitations, shortness of breath, sweating, dizziness)?” (physical reactions due to recalling the disaster).
History of diagnosed mental disorders
Besides the question about disaster-related stress symptoms, the history of diagnosed mental disorders was collected through self-reported answers. Respondents were asked: “Have medical doctors diagnosed you with any of the following diseases before/after the GEJE?” We classified any diagnosed cases into “developed pre-disaster” and “newly developed after the GEJE.” We focused on depression and post-traumatic stress disorder (PTSD), given previous studies have reported that these disorders are more likely to develop after devastating natural disasters ^(38), (39)^.
Sleep status
Sleep status was measured using the Athens Insomnia Scale (AIS), a validated screening tool for sleep status ^(40)^. This study used the Japanese version of the AIS, which includes the following items: sleep induction, awakenings during the night, final awakening earlier than desired, total sleep duration, overall quality of sleep, sense of well-being during the day, daytime physical and mental functioning, and daytime sleepiness. Participants who scored 6 or higher were classified as having sleep problems ^(41)^.
Social networks
Social networks were evaluated using the Lubben Social Network Scale-6 (LSNS-6), Japanese version ^(42)^. The scale comprises six questions: (1) “How many relatives do you see or hear from at least once a month?”; (2) “How many relatives do you feel comfortable talking with about private matters?”; (3) “How many relatives do you feel close to such that you could call on them for help?”; (4) “How many of your friends do you see or hear from at least once a month?”; (5) “How many friends do you feel comfortable talking with about private matters?”; and (6) “How many friends do you feel close to such that you could call on them for help?” Participants responded on a five-point scale (0 = none, 1 = one, 2 = two, 3 = three or four, 4 = five to eight, 5 = nine or more). Respondents with 11 points or fewer were classified as socially isolated ^(43)^.
Data analysis
We excluded 2,091 participants who had died from causes other than suicide death. First, we performed a simple tabulation, then conducted univariate logistic regression analysis to evaluate the association with suicide death after the GEJE, adjusted for cohort group, sex, age group, educational attainment, and marital status.
Furthermore, receiver operating characteristic (ROC) curve analyses were performed to assess the predictive ability of the K6 score in combination with single variables in discriminating suicide death, as follows: (1) K6 score alone, and K6 score with (2) binge drinking, (3) social network, (4) sleep problems, (5) diagnosed mental disorders after the GEJE, (6) disaster-related experiences, and (7) disaster stress symptoms. We then compared the area under the ROC curve (AUC) for the K6 score combined with each variable and without each variable. AUC values higher than 0.80 are generally considered clinically useful, whereas values lower than 0.80 are considered of limited clinical utility ^(44)^.
Statistical significance was evaluated using two-sided, design-based tests at a 5% significance level, with analyses conducted using Stata 18 (StataCorp, College Station, TX, USA).
Ethical considerations
Our study protocol for the TMM CommCohort Study and the TMM BirThree Cohort Study was approved by Ethical Research Committee at Tohoku University Graduate School of Medicine (2013-4-103, approval date: May 10, 2013; latest revised 2023-4-040, approval date: June 21, 2023). Moreover, this study protocol has conformed to the provisions of the Declaration of Helsinki. Informed consent has been obtained from all participants of TMM CommCohort Study and TMM BirThree Cohort Study.
Results
Basic participant characteristics
The participants’ basic characteristics are listed in Table 1. Among the affected residents, the proportions of individuals with newly developed depression and PTSD, disaster-related experiences, and disaster-related stress symptoms were higher. Moreover, the proportions of moderate (K6 score: 5-12) and severe (K6 score: 13 or more) psychological distress were high. Sleep disturbances were also slightly more prevalent among the affected residents. Incidentally, the crude suicide mortality rate per 100,000 participants in each group―affected residents and residents within the disaster-stricken area―were 10.8 and 7.6, respectively.
Association with suicide death
Among the affected residents, depression newly developed after the GEJE, PTSD developed pre-disaster, and PTSD newly developed after the GEJE were a higher proportion in suicide cases than those who lived within the disaster-stricken area (Table 2).
In univariate logistic regression analysis, individuals with reduced social networks (LSNS-6 ≤11), moderate and severe psychological distress (K6 5-12 and K6 ≥13), sleep problems (AIS ≥6), or a diagnosis of depression or PTSD (pre-disaster or newly developed) were significantly associated with suicide death among affected residents. In addition, disaster-related stress symptoms, such as physical reactions when recalling the disaster, were specific risk factors (Table 3). Incidentally, we found little evidence of a notable inverse relationship between men and women, and each age group (Supplementary Table 1 and 2).
Predicting suicide death in ROC analyses
The AUC of the K6 score alone was 0.681 (95% confidence interval [CI]: 0.567-0.794) for affected residents. When the K6 score was combined with additional variables, newly developed PTSD after the GEJE (AUC: 0.878 [95% CI: 0.773-0.982]), the disaster stress symptom of recollection of disaster experiences (AUC: 0.849 [95% CI: 0.714-0.985]), and decreased income (AUC: 0.835 [95% CI: 0.726-0.945] were significantly higher than that of the AUC without each variable, which yielded much higher AUC values combined with these variables than did K6 alone (Table 4).
Discussion
We identified in ROC curve analysis combining the K6 score with newly developed PTSD after the GEJE or with the disaster stress symptom of recollection of disaster experiences improved the accuracy of suicide prediction compared with using K6 alone. We consider the utility of K6, a commonly used measure in Japanese disaster settings, for suicide prevention screening. According to our ROC analysis, the AUC for K6 alone was 0.681 (95% CI: 0.567-0.794), suggesting that K6 alone is not sufficiently accurate for predicting suicide death. In contrast, combining the K6 score with newly developed PTSD, with disaster stress symptoms (e.g., physical reactions to recalling the disaster), and with decreased income significantly increased predictive accuracy.
It goes without saying that PTSD and traumatic stress are well-established risk factors for suicide ^(45), (46)^. Even with a self-reported measure of diagnosed PTSD, the K6-plus-newly developed PTSD approach still yielded better predictive accuracy than did K6 alone. Moreover, in comparing disaster experiences and associated symptoms, the latter (e.g., physical reactions to disaster recollections) showed greater predictive power for suicide death than did the experience of losing family or friends. Although losing a loved one is undoubtedly stressful, our findings emphasize the importance of screening for stress responses rather than simply cataloging disaster-related events. Residents with disaster-related stress symptoms were supported by disaster-related mental health services, which have provided continuous counseling through outreach to help reduce these residents’ psychological burden. In fact, frequent outreach efforts may have contributed to relief in traumatic stress symptoms, leading to the successful conclusion of the support activities ^(16)^. For this backdrop, it would be essential to screen for K6 in addition to disaster-related stress symptoms in the setting of disaster-related mental health services, and to provide continuous support to those affected residents.
We also found that combining the K6 score with decreased income due to the GEJE improved suicide prediction accuracy among affected residents, consistent with previous studies linking income reduction after a devastating disaster to severe psychological distress or post-traumatic stress ^(47), (48)^.
Overall, these findings indicate that relying solely on the K6 score is insufficient for suicide prevention in post-disaster contexts. Instead, screening protocols should incorporate additional factors―especially disaster-related stress symptoms, newly developed PTSD, and changes in income―to more effectively identify individuals at high risk. Incidentally, the positive predictive value of K6 ≥13 points with newly developed PTSD was 3.85% among the affected residents, which was greater than that of K6 ≥5 points with newly developed PTSD (1.65%). Thus, in the context of disaster-related mental health activities, a K6 score of greater than 13 points would be appropriate (Supplementary Table 3).
Regarding differences between affected residents and residents living within the disaster-stricken area, this study found that there was a difference in binge drinking and disaster experiences of loss of family members; binge drinking and experiencing the loss of a family member presented a lower risk of suicide death among affected residents, whereas both factors posed a higher risk among those living within the disaster-stricken area. The disparity in the level of disaster-related mental health services after the GEJE may have an impact on these results. Affected individuals with binge drinking behaviors and the experience of loss of a family member were primarily targeted for counseling in the disaster-related mental health services ^(20), (21)^, whereas residents living within the disaster-stricken area had limited access to disaster-related mental health interventions.
Several limitations merit consideration. First, the cause of suicide death was unclear; moreover, this study did not ascertain whether the participants actually received disaster-related mental health services. Second, our classification―affected residents and residents living within the disaster-stricken area―was based on self-reported data. Third, there are inherent representativeness issues, given cohort participants tend to be more interested in healthy behaviors ^(49)^, and our study sample may not fully reflect all affected residents in the disaster-stricken region. Fourth, all variables―including diagnosed mental disorders―were self-reported, raising the possibility of response bias. Fifth, because the TMM CommCohort and BirThree Cohort Studies began in 2013, our findings may not apply to the immediate post-disaster period because risk factors for suicide death could differ shortly after such an event. Fifth, the number of suicide cases was small, limiting the statistical power to detect certain risk factors or fully evaluate predictive accuracy. Furthermore, the relative variables among suicide cases were exceedingly low (e.g, binge drinking and loss of family were just two cases, respectively). As a result, combining K6 exposure with multiple factors was challenging to evaluate. Finally, this study area is limited to specific region in Japan.
Despite these limitations, this large-scale cohort study uniquely integrates several disaster-specific questionnaire items with official cause-of-death data. To our knowledge, this was the first study to investigate suicide risk and predictive accuracy for suicide death in a cohort established after the GEJE, offering valuable insights into post-disaster suicide prevention measures.
In conclusion, our study identified, combining the K6 score with newly developed PTSD, the disaster stress symptom of recollection of disaster experiences, and changes in income improved suicide prediction accuracy compared with using K6 alone when the ROC curve analyses. We hope these findings will help minimize post-disaster suicide death by guiding practical disaster-related mental health services in the future. (3,417 words)
Data availability statement
According to regulations from the Ministry of Health, Labour and Welfare, permission is required to use vital statistical data; therefore, it must be requested in advance to the corresponding author. All data except vital statistical data used to support the findings may be released on application to the Tohoku Medical Megabank Organization.
Article Information
Acknowledgments
Our research members are as follows: https://www.megabank.tohoku.ac.jp/english/a240901/
This study was permitted officially for the use of data of vital statistics from the Ministry of Health, Labour on the basis of Article 33 of the Statistics Act.
Author Contributions
Masatsugu Orui conceptualized and designed this study, conducted the initial analyses, drafted the initial manuscript, and revised the manuscript.
Shinichi Kuriyama conceptualized, designed, and organized the TMM CommCohort Study and BirThree Cohort Study, and reviewed the manuscript.
Atsushi Hozawa, Kozo Tanno, Naoki Nakaya, Mana Kogure, and Yuka Kotozaki managed the implementation of the TMM CommCohort Study and reviewed the manuscript.
Masahiro Kikuya, Hirohito Metoki, Taku Obara, Mami Ishikuro, Aoi Noda, Genki Shinoda, and Keiko Murakami managed the implementation of the TMM BirThree Cohort Study and reviewed the manuscript.
Masatsugu Orui, Mana Kogure, and Yuka Kotozaki performed the linkage of vital statistical data and the information of baseline questionnaires.
Masaharu Maeda and Yoshitake Takebayashi conceptualized this study and critically reviewed the manuscript.
All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Conflicts of Interest
None
Approval code issued by the institutional review board and the name of the institution(s)
This study was approved by the Ethical Research Committee at Tohoku University Graduate School of Medicine (TMM CommCohort Study: 2012-4-617, approval date: March 21, 2013; TMM BirThree Cohort Study: 2013-4-103, approval date: May 10, 2013). Informed consent was obtained from all participants in the TMM CommCohort Study and TMM BirThree Cohort Study.
Supplement
Supplementary Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Murphy SA. Status of natural disaster victims’ health and recovery 1 and 3 years later. Res Nurs Health. 1986;9(4):331-40.3643610 10.1002/nur.4770090410 · doi ↗ · pubmed ↗
- 2Kiliç C, Ulusoy M. Psychological effects of the November 1999 earthquake in Turkey: an epidemiological study. Acta Psychiatr Scand. 2003;108(3):232-8.12890279 10.1034/j.1600-0447.2003.00119.x · doi ↗ · pubmed ↗
- 3Sone T, Nakaya N, Sugawara Y, et al. Longitudinal association between time-varying social isolation and psychological distress after the Great East Japan Earthquake. Soc Sci Med. 2016;152:96-101.26851408 10.1016/j.socscimed.2016.01.037 · doi ↗ · pubmed ↗
- 4Kunii Y, Suzuki Y, Shiga T, et al. Severe psychological distress of evacuees in evacuation zone caused by the Fukushima daiichi nuclear power plant accident: the Fukushima health management survey. P Lo S One. 2016;11(7):e 0158821.27391446 10.1371/journal.pone.0158821 PMC 4938533 · doi ↗ · pubmed ↗
- 5Oe M, Maeda M, Nagai M, et al. Predictors of severe psychological distress trajectory after nuclear disaster: evidence from the Fukushima Health Management Survey. BMJ Open. 2016;6(10):e 013400.10.1136/bmjopen-2016-013400 PMC 507355427798033 · doi ↗ · pubmed ↗
- 6Tanji F, Tomata Y, Sekiguchi T, et al. Period of residence in prefabricated temporary housing and psychological distress after the Great East Japan Earthquake: a longitudinal study. BMJ Open. 2018;8(5):e 018211.10.1136/bmjopen-2017-018211 PMC 594241929730612 · doi ↗ · pubmed ↗
- 7Orui M, Nakayama C, Moriyama N, et al. Those who have continuing radiation anxiety show high psychological distress in cases of high post-traumatic stress: the Fukushima nuclear disaster. Int J Environ Res Public Health. 2021;18(22):12048.34831804 10.3390/ijerph 182212048 PMC 8623122 · doi ↗ · pubmed ↗
- 8Kunii Y, Usukura H, Utsumi Y, et al. Review of mental health consequences of the great East Japan earthquake through long-term epidemiological studies: the Shichigahama health promotion project. Tohoku J Exp Med. 2022;257(2):85-95.35569933 10.1620/tjem.2022.J 039 · doi ↗ · pubmed ↗