Concurrent Diabetic Ketoacidosis and Non-ST-Elevation Myocardial Infarction: A Complex Cardiometabolic Emergency
Kinza Moin, Zahra Amini, Ridha Umar

TL;DR
A rare case of diabetic ketoacidosis caused by a heart attack highlights the challenges of managing overlapping metabolic and cardiac emergencies.
Contribution
This case report highlights the rare but clinically significant occurrence of NSTEMI-induced DKA and emphasizes the need for coordinated care.
Findings
A 51-year-old man with type 2 diabetes developed DKA due to a non-ST-elevation myocardial infarction.
The patient required ICU care and coronary artery bypass grafting after showing multi-vessel coronary artery disease.
The case emphasizes the importance of early recognition and multidisciplinary management in complex cardiometabolic emergencies.
Abstract
Diabetic ketoacidosis (DKA) is a severe diabetic emergency usually triggered by an infection or missed insulin doses. Concurrent myocardial infarction, though an uncommon precipitating factor, complicates diagnosis and management due to overlapping clinical features and contradictory management challenges. We report the case of a 51-year-old male patient with type 2 diabetes mellitus, hypertension, and dyslipidemia, who presented with a two-day history of central chest pain radiating to the left arm, associated with nausea, vomiting, exertional dyspnea, and orthopnea. On examination, he was hypotensive, tachycardic, and clinically dehydrated. Initial investigations revealed sinus tachycardia with ST-segment depression in leads V4, V5 and V6 on ECG, severe hyperglycemia (glucose 20.1 mmol/L), ketonemia (>7 mmol/L), and high anion gap metabolic acidosis (pH 7.06, bicarbonate 9 mmol/L),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
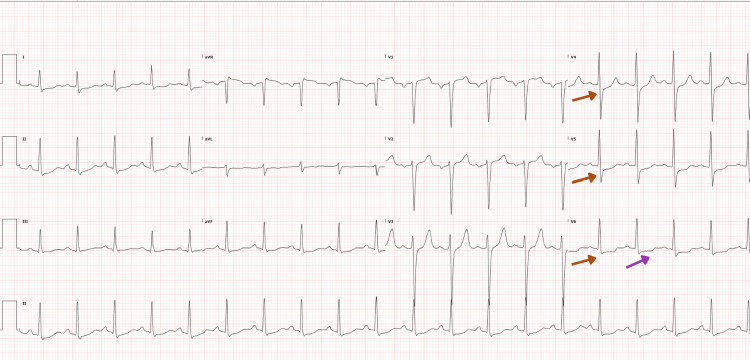 Figure 1
Figure 1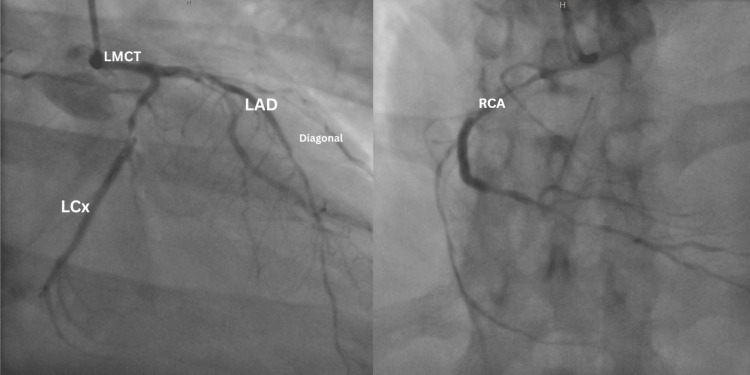 Figure 2
Figure 2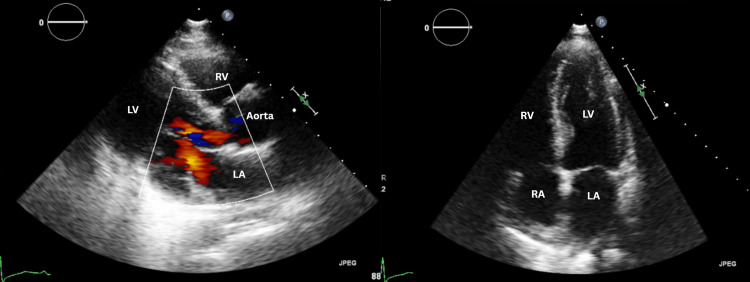 Figure 3
Figure 3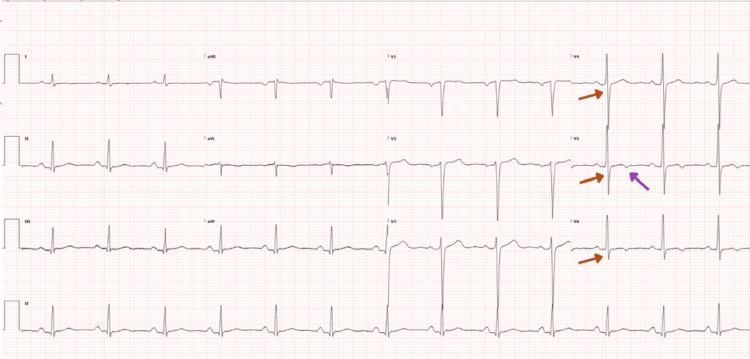 Figure 4
Figure 4| Variable | Result | Reference range |
| pH (Venous) | 7.05 | 7.35–7.45 |
| pCO2 (partial pressure carbon dioxide) | 33.2 mmHg | 35–45 mmHg |
| pO2 (partial pressure oxygen) | 33.8 mmHg | 80–100 mmHg |
| Bicarbonate (HCO3) | 9 mmol/L | 22–26 mmol/L |
| Base excess (BE) | -20.7 mmol/L | -2.0–2.0 mmol/L |
| Total hemoglobin (THB) | 146 g/L | 120–170 g/L |
| O2 saturation | 53.4% | 95–99% |
| Oxyhemoglobin (O2Hb) | 52% | ≥95% |
| Carboxyhemoglobin (COHb) | 0.8% | <2% |
| Deoxyhemoglobin (HHb) | 45.5% | — |
| Methemoglobin (MetHb) | 1.6% | <2% |
| Potassium (K) | 4.7 mmol/L | 3.4–5.1 mmol/L |
| Chloride (Cl) | 102 mmol/L | 98–107 mmol/L |
| Sodium (Na) | 135 mmol/L | 136–145 mmol/L |
| Glucose | 19.6 mmol/L | 3.9–6 mmol/L |
| Lactate | 2.8 mmol/L | 0.5-2.2 mmol/L |
| Variable | Result | Reference range |
| pH (Venous) | 7.48 | 7.35–7.45 |
| pCO2 (partial pressure of carbon dioxide) | 32.7 mmHg | 35–45 mmHg |
| pO2 (partial pressure of oxygen) | 106 mmHg | 80–100 mmHg |
| Bicarbonate (HCO3) | 24 mmol/L | 22–26 mmol/L |
| Base excess (BE) | 1.4 mmol/L | -2 – 2 mmol/L |
| Total hemoglobin (THB) | 130 g/L | 120–170 g/L |
| O2 saturation | 97.4% | 95–99% |
| Oxyhemoglobin (O2Hb) | 95.7% | ≥95% |
| Carboxyhemoglobin (COHb) | 0.5% | <2% |
| Methemoglobin (MetHb) | 1.20% | <2% |
| Potassium (K) | 3.5 mmol/L | 3.4–5.1 mmol/L |
| Chloride (Cl) | 111 mmol/L | 98–107 mmol/L |
| Sodium (Na) | 149 mmol/L | 136–145 mmol/L |
| Glucose | 9.6 mmol/L | 3.9–6 mmol/L |
| Lactate | 1.2 mmol/L | 0.5–2.2 mmol/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes and associated disorders · Neurological and metabolic disorders · Cardiovascular Function and Risk Factors
Introduction
Diabetic ketoacidosis (DKA) is a critical metabolic emergency commonly triggered by infection, missed insulin, or physiological stress [1,2]. Although uncommon, acute myocardial infarction (MI) can precipitate DKA and occurs in about 4% of cases, with mortality approaching 85% [3]. One important subtype is non-ST-elevation myocardial infarction (NSTEMI), a form of heart attack caused by reduced blood flow to the heart muscle that does not produce the classic ST-segment elevation on electrocardiography and may therefore be less immediately recognizable. Because DKA and MI share symptoms such as epigastric pain and sudden shortness of breath, their coexistence often creates diagnostic uncertainty. Management is further complicated because DKA necessitates substantial fluid resuscitation, yet in patients with MI and concurrent acute heart failure, rapid volume expansion can be hazardous and creates a major therapeutic challenge.
Case presentation
A 51-year-old male patient presented to the emergency department with a two-day history of central chest pain radiating to the left arm. The pain was described as burning in nature, severe in intensity, and progressively worsening over the preceding 24 hours. Associated symptoms included nausea, vomiting, exertional dyspnea, and orthopnea. He denied palpitations, dizziness, or syncope. Based on his severe symptoms, concerning chest pain characteristics, and the need for prompt diagnostic evaluation and interventions, the patient was assigned an Emergency Severity Index (ESI) Category two [4] and transferred to the resuscitation bay immediately.
On examination, the patient appeared clinically unwell and dehydrated, though alert and oriented. His vital signs were notable for hypotension (BP 92/68 mmHg; normal systolic ≥90 mmHg), tachycardia (heart rate 118 beats/minute; normal 60-100 beats/minute), and tachypnea (respiratory rate 22 breaths/minute; normal 12-20 breaths/minute). Chest auscultation revealed clear breath sounds bilaterally, and abdominal examination was unremarkable.
His medical history was significant for type 2 diabetes mellitus managed with subcutaneous tirzepatide 15 mg, hypertension, and dyslipidemia, for which he was on amlodipine 10 mg and atorvastatin 10 mg, respectively. He also reported having angina symptoms previously and was suspected to have acute coronary syndrome (ACS) 15 years prior, managed conservatively with aspirin and clopidogrel, although no definitive diagnostic workup was performed at that time.
An initial electrocardiogram (ECG) demonstrated sinus tachycardia with ST-segment depression in leads V4, V5 and V6 without additional ischemic changes (Figure 1).
Electrocardiogram showing ST segment depression in leads V4, V5, V6 (red arrows) and T wave inversion in V6 (purple arrow)
Point-of-care venous blood gas (VBG) analysis revealed severe high-anion gap metabolic acidosis. The patient was markedly hyperglycemic (glucose 19.6 mmol/L) with profound ketonemia (>7 mmol/L). Bicarbonate was low at 9 mmol/L, with an elevated anion gap of 24, and the pH was 7.05. These laboratory findings, particularly the combination of low bicarbonate and high anion gap, were consistent with metabolic acidosis typical of diabetic ketoacidosis (Table 1).
Management was promptly initiated with intravenous fluid resuscitation using balanced crystalloids and a continuous intravenous insulin infusion at 0.1 units/kg/hour. Electrolyte replacement was carefully titrated based on serial laboratory assessments. During the management of DKA, the patient’s initial high-sensitivity cardiac troponin T level was elevated at 56.2 ng/L (reference ≤14 ng/L), raising concern for a NSTEMI. The constellation of severe central chest pain, high-anion gap metabolic acidosis with marked hyperglycemia and ketonemia, and elevated cardiac troponin levels represented key diagnostic red flags. These findings prompted clinicians to consider the coexistence of DKA and ACS early in the evaluation and guided urgent investigations and management.
The cardiology team was consulted. As the patient’s chest pain subsided with analgesia and no immediate indication for invasive intervention was identified, a conservative medical management strategy was adopted, which included a loading dose of aspirin 300 mg followed by 100 mg daily, ticagrelor 180 mg loading dose followed by 90 mg twice daily, atorvastatin 80 mg once daily, enoxaparin 1 mg/kg subcutaneously twice daily, bisoprolol 2.5 mg once daily, and ramipril 2.5 mg once daily-initiated after achieving hemodynamic stabilization.
After four hours of emergency department resuscitation, the patient was transferred to the intensive care unit (ICU) for ongoing care. He subsequently developed oxygen desaturation to 94% on 4 L/min oxygen via nasal cannula. Examination revealed bilateral basal crackles. Non-invasive ventilation with bilevel positive airway pressure (BiPAP) was initiated, leading to rapid clinical and oxygenation improvement.
Fluid replacement was titrated by serial assessments of cardiovascular function and overall volume status using bedside echocardiogram (to visualize cardiac contractility and inferior vena cava) and measuring urine output. His management followed standard DKA protocols, with very cautious fluid resuscitation using 4-5 liters of balanced crystalloids over 24 hours, continuous IV insulin infusion at 0.1 units/kg/hour, and guided potassium replacement. VBG was repeated every two hours in the emergency department and every three hours in the ICU until resolution of DKA. The resolution of DKA was evidenced by normalization of pH, closure of the anion gap, and clinical stabilization. Repeat VBG after 12 hours showed normalization of acid-base parameters (pH 7.48, bicarbonate 24 mmol/L, closed anion gap), confirming the resolution (Table 2).
Serial high-sensitivity cardiac troponin T levels demonstrated a progressive rise, peaking at 429 ng/L. This dynamic troponin elevation, in conjunction with ischemic electrocardiographic changes including ST-segment depression in the lateral leads, was indicative of active myocardial ischemia. The presence of evolving biomarker and ECG abnormalities prompted escalation of care and supported an early invasive strategy. Consequently, coronary angiography was performed on day two of the hospitalization, revealing severe multivessel coronary artery disease. Findings included 40-50% eccentric stenosis of the left main coronary artery, 80% discrete proximal stenosis of the left anterior descending (LAD) artery, 80% diffuse stenosis in the first diagonal branch, 80% diffuse stenosis in the ramus intermedius, 90% proximal diffuse stenosis of the left circumflex artery (LCX), and 95% proximal stenosis along with 70-80% stenosis in the posterior descending artery (PDA) of the right coronary artery (RCA) (Figure 2).
Coronary angiography demonstrating severe multi-vessel coronary artery diseaseThe coronary angiogram (image on the left) shows the left main coronary artery (LMCT) with eccentric luminal narrowing, giving rise to the left anterior descending (LAD) artery, which demonstrates severe proximal stenosis with additional diffuse disease involving the first diagonal branch. The left circumflex artery (LCx) shows severe proximal diffuse narrowing. The right coronary angiogram (image on the right) demonstrates significant proximal right coronary artery (RCA) stenosis with reduced distal opacification, consistent with advanced obstructive disease.
Trans-thoracic echocardiography (TTE) demonstrated normal chamber dimensions with mildly reduced ejection function (EF 40-45%) and regional wall motion abnormalities involving the mid-inferior, apical anterior, apical septal segments, and the apex. No pericardial effusion or signs of pulmonary hypertension were identified (Figure 3).
Color doppler imagesParasternal long-axis view with color doppler (image on the left) showing normal flow across the left ventricular outflow tract extending into the ascending aorta. Apical four-chamber view (image on the right) demonstrating normal chamber orientation with preserved left ventricular cavity size. The right atrium (RA), right ventricle (RV), left atrium (LA), and left ventricle (LV) are labeled. No pericardial effusion can be seen. Regional wall motion abnormalities involving the mid-inferior, apical anterior, apical septal segments, and the apex were identified on dynamic echocardiographic assessment and are not fully appreciable on representative static images.
Based on angiographic and echocardiographic findings, the patient was referred for coronary artery bypass grafting (CABG), which was successfully completed at an external center. Although detailed operative notes were unavailable, follow-up at our institution demonstrated favorable recovery. Transthoracic echocardiography performed three months postoperatively showed improved left ventricular systolic function with an EF of 50%.
Glycemic control was optimized, with fasting glucose consistently within 6-8 mmol/L and HbA1c improving to 7.1%. The patient reported significant improvement in exercise tolerance and functional capacity, able to perform daily activities without chest pain or dyspnea (New York Heart Association or NYHA Class I). In comparison with the initial ECG on arrival, ECG done after CABG showed a resolution of the ST depression in V4, V5, V6 and nonspecific T wave inversions in leads V5 and V6 (Figure 4).
Electrocardiogram showing resolution of ST depressions in leads V4,V5 and V6 (red arrows) and non specific T wave inversions in leads V5 and V6 (purple arrow)
Discussion
DKA is a life-threatening metabolic emergency characterized by profound hyperglycemia, ketosis, and high anion gap metabolic acidosis, resulting from either absolute or relative insulin deficiency. It is often triggered by infection, missed insulin doses, or acute physiological stress. In rare but clinically significant cases, MI can serve as the precipitating factor - particularly in individuals with long-standing diabetes and underlying coronary artery disease - with an estimated incidence of approximately 1% [5].
In this case, determining whether DKA precipitated NSTEMI or vice versa is challenging. A case report by Kaefer et al. explores the bidirectional relationship between ACS and DKA, highlighting how each condition can trigger or exacerbate the other [5]. DKA pathogenesis involves counter-regulatory hormone excess - glucagon, catecholamines, cortisol, and growth hormone - which promote lipolysis, hepatic gluconeogenesis, and ketogenesis, culminating in metabolic acidosis and dehydration [1,2]. Insulin deficiency raises free fatty acids and ketones, which disrupt myocyte membranes and limit glucose uptake [5]. In this patient, myocardial ischemia likely acted as the precipitating stressor, disrupting glycemic control and triggering DKA. Notably, DKA can mask or mimic ACS symptoms such as chest pain, nausea, and tachypnea, complicating the diagnostic process [2].
Additionally, NSTEMI in this context likely arose due to a combination of demand ischemia and underlying coronary artery disease. DKA creates a systemic pro-inflammatory state, increasing oxidative stress and impairing endothelial function, potentially precipitating Type 2 MI even in the absence of coronary occlusion [6]. However, angiography in this case revealed significant multivessel disease, including critical stenoses in the LAD, RCA, LCX, and ramus intermedius, indicating true ischemic injury.
One of the key challenges in the concurrent DKA and NSTEMI management lies in balancing aggressive fluid resuscitation, critical for correcting ketoacidosis, with the risk of fluid overload and cardiac decompensation. The management of DKA in patients with concurrent NSTEMI is particularly complex due to the need for fluid resuscitation in DKA, which may exacerbate cardiac dysfunction and pulmonary congestion especially in those with heart failure. In such cases, cautious fluid administration is essential, with studies suggesting initiation of isotonic saline at reduced rates. A case report by Zuhri et al. highlighted the challenge of managing DKA with acute MI and heart failure, successfully addressed by using echocardiography-guided fluid resuscitation and primary percutaneous coronary intervention (PCI), leading to discharge in 10 days [7].
Given the complexity of the clinical scenario, individualized treatment guided by continuous monitoring of cardiac function and volume status is critical to balance metabolic correction with cardiovascular stability [7]. Current American Diabetes Association (ADA) guidelines emphasize prompt fluid resuscitation, intravenous insulin therapy, electrolyte correction, and identification of precipitating factors as the cornerstones of DKA management. In patients with concurrent cardiac disease, the ADA recommends cautious fluid administration with close monitoring to avoid volume overload [8].
This case exemplifies the complex interplay between diabetes, cardiovascular disease, and metabolic decompensation. Studies have shown that MI and congestive heart failure are major contributors to DKA-related mortality, accounting for up to 28% of deaths [5]. Furthermore, hyperglycemia itself is an independent predictor of adverse outcomes in ACS, regardless of diabetes status [9]. The management of this patient was consistent with the American College of Cardiology/American Heart Association (ACC/AHA) guidelines for NSTEMI, which emphasize early risk stratification, prompt electrocardiographic evaluation, serial cardiac biomarker assessment, and initiation of guideline-directed medical therapy, including dual antiplatelet therapy, anticoagulation, and high-intensity statin therapy [10]. An early invasive strategy with coronary angiography is recommended for high-risk patients, whereas a more selective approach may be appropriate for those at lower risk. Overall, management should be individualized, carefully balancing ischemic and bleeding risks, and ensuring implementation of appropriate secondary prevention strategies prior to discharge.
Prompt recognition of ACS in DKA patients is essential, given their elevated risk for arrhythmias, cardiogenic shock, and mortality. Early ECG and serial troponin measurements are critical diagnostic tools, even when initial ECGs are non-specific. Tailored management, integrating DKA correction with cardioprotective therapy and revascularization, is essential to improving outcomes in this high-risk population [9].
Conclusions
The coexistence of DKA and NSTEMI represents a critical intersection of metabolic and cardiovascular emergencies, where causality may be bidirectional and not immediately apparent. In this patient, continuous ECG monitoring, serial cardiac biomarkers, and close hemodynamic surveillance enabled early detection of myocardial ischemia. Coordinated multidisciplinary care, with careful balancing of fluid resuscitation and cardiac therapies, was crucial for achieving a favorable outcome. This case highlights the importance of vigilant cardiac assessment during DKA and illustrates how MI, even when not initially evident on ECG, can precipitate acute metabolic decompensation in patients with diabetes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hyperglycemic crises in adult patients with diabetes Diabetes Care Kitabchi AE Umpierrez GE Miles JM Fisher JN 133513433220091956447610.2337/dc 09-9032 PMC 2699725 · doi ↗ · pubmed ↗
- 2Adult diabetic ketoacidosis Stat Pearls [Internet] Lizzo JM Goyal A Kaur J Treasure Island (FL)Stat Pearls Publishing 2025 http://www.ncbi.nlm.nih.gov/books/NBK 560723/32809558 · pubmed ↗
- 3Diabetic ketoacidosis and myocardial infarction: a diagnostic and therapeutic challenge Int J Sci Res Kumbhar S Lohar R Haldhar A Kant R 89122025
- 4Emergency Severity Index (ESI): A Triage Tool for Emergency Department Care, Version 4. Implementation Handbook 2012 Edition Gilboy N Tanabe T Travers D Rosenau AM Rockville, MD Agency for Healthcare Research and Quality 2011 https://www.govinfo.gov/content/pkg/GOVPUB-HE 20_6500-PURL-gpo 23161/pdf/GOVPUB-HE 20_6500-PURL-gpo 23161.pdf
- 5Acute coronary syndrome and diabetic keto acidosis: the chicken or the egg?Ann Transl Med Kaefer K Botta I Mugisha A 397720193155571110.21037/atm.2019.07.38PMC 6736820 · doi ↗ · pubmed ↗
- 6Association between hyperglycaemic crisis and long-term major adverse cardiovascular events: a nationwide population-based, propensity score-matched, cohort study BMJ Open Chang LH Lin LY Tsai MT 06201610.1136/bmjopen-2016-012233 PMC 501348727554106 · doi ↗ · pubmed ↗
- 7Management of diabetic ketoacidosis concomitant with acute myocardial infarction with acute heart failure: a case report Cardiometab Syndr J Zuhri E Iryuza N 717622022
- 8Hyperglycemic crises in adults with diabetes: a consensus report Diabetes Care Umpierrez GE Davis GM El Sayed NA 125712754720243905290110.2337/dci 24-0032 PMC 11272983 · doi ↗ · pubmed ↗