Evaluation of a novel PCR-based assay for the detection of Candida auris colonization
Jesse Leonard, Alicia Amamoto, Monica Bates, Anh T. Tran, Pooja Ghatbale, Ahnika Kline, David T. Pride

TL;DR
This study evaluates a new PCR test for detecting Candida auris colonization, showing it performs well compared to traditional methods and lab-developed tests.
Contribution
This is the first evaluation of the FDA-approved Diasorin Simplexa C. auris assay outside of the FDA submission process.
Findings
The assay demonstrated 100% sensitivity and 90% specificity compared to culture.
It showed 100% agreement with two existing lab-developed tests.
The assay had 100% analytical specificity and no cross-reactivity.
Abstract
Candida auris is an emerging fungal pathogen linked to healthcare-associated infections, necessitating rapid and accurate detection for effective infection control. This study evaluated the analytical and clinical performance of the Diasorin Simplexa C. auris Direct IVD assay compared to traditional culture as the reference standard and also to two lab-developed tests (LDTs) already validated in our laboratory: one using DSQ Alert primers/probes on the Roche Cobas 5800 and another on the DiaSorin LIAISON MDX platform. Clinical accuracy was assessed using deidentified residual axillary/groin surveillance specimens from 20 culture-positive and 20 culture-negative patients. Analytical specificity was tested against 14 microbial species commonly found in the axilla/groin. Analytical sensitivity was determined using ZeptoMetrix C. auris strain Z485. Specimen stability was examined at various…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
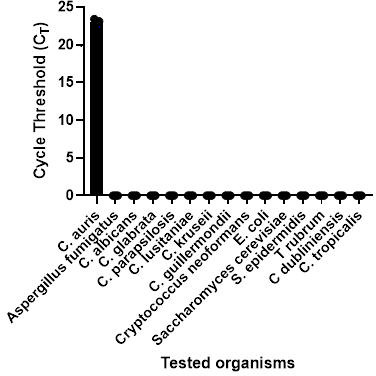 Fig 1
Fig 1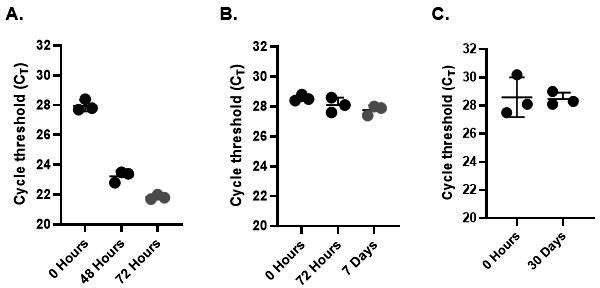 Fig 2
Fig 2| Storage condition | Test time points |
|---|---|
| Room temperature (22– 25°C) | 0 h, 48 h, 72 h |
| Refrigerated (2–8°C) | 0 h, 72 h, 7 days |
| Frozen (<−70°C) | 0 h, 30 days |
| Diasorin | Reference method (culture + MALDI) | ± 95% CI | |||||
|---|---|---|---|---|---|---|---|
| Positive | Negative | Total | Sensitivity | Specificity | Accuracy | Kappa ( | |
| Positive | 18 | 2 | 20 | 100%(0.82–1) | 90% (0.72–0.98) | 95% | 0.9 |
| Negative | 0 | 20 | 20 | ||||
| Total | 18 | 22 | 40 | ||||
| Concentration (CFU/mL) | CFU/reaction | Number tested | Number detected | Minimum CT | Maximum CT | % Detected |
|---|---|---|---|---|---|---|
| 1,510 | 75.5 | 20 | 20 | 27.7 | 32.0 | 100% |
| 702 | 35.1 | 20 | 20 | 29.3 | 32.8 | 100% |
| 233 | 11.7 | 14 | 12 | 30.0 | 37.9 | 85% |
| Environmental location | Swabs tested | Direct IVD result | Mean IC CT |
|---|---|---|---|
| Interior (before testing) | 5 | Undetected (100%) | 27.3 |
| Interior (after testing) | 5 | Undetected (100%) | 27.3 |
| Exterior (before testing) | 5 | Undetected (100%) | 27.3 |
| Exterior (after testing) | 5 | Undetected (100%) | 27.3 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Fungal Infections and Studies · Bacterial Identification and Susceptibility Testing
INTRODUCTION
Candida auris is an emerging fungal pathogen first described in 2009 after being isolated from a patient’s ear canal in Japan (1). The first case of C. auris in the United States occurred in 2013, and since then, the number of annual cases has risen dramatically (2). Between 2019 and 2022, the number of clinical C. auris and colonization cases increased by 214% and 339%, respectively (3). In 2020, at the onset of the COVID-19 pandemic, the Centers for Disease Control and Prevention (CDC) reported a concerning spread of C. auris across healthcare facilities in the United States. By 2021, the number of isolates exhibiting resistance to echinocandins, the standard treatment for C. auris infections, had tripled (4).
Since then, C. auris has become a global concern, with cases in at least 50 countries on six continents (5, 6). In response to this threat, the World Health Organization recently classified C. auris as a critical fungal pathogen on its Fungal Priority Pathogens List. Additionally, the CDC has acknowledged C. auris as a public health threat, requiring urgent and aggressive intervention. This classification is due to the organism’s ability to cause invasive infections with high mortality rates, its potential for widespread outbreaks in healthcare settings, its capacity to asymptomatically colonize human skin, its intrinsic resistance to most available antifungal treatments and common disinfectants, and the challenges it presents in accurate identification and characterization using traditional laboratory methods (7, 8).
Not only is it difficult to distinguish C. auris from other Candida species using conventional laboratory methods, but many studies have also reported that biochemical-based tests misidentify C. auris as other Candida species or even genera (9–11). This misidentification can lead to misdiagnosis, inappropriate management, and missed opportunities for infection control. Currently, the CDC recommends screening patients at risk for C. auris colonization, including those with an epidemiological link to a colonized patient or facility, and healthcare facilities both within and outside the United States located in high-prevalence areas. Patients with risk factors for acquiring C. auris, such as mechanical ventilation, in-dwelling medical devices, receipt of high acuity medical care, frequent or long healthcare stays, infection, or colonization with other multidrug-resistant organisms (12). Current guidance suggests swabbing the axilla and groin though recent data suggest improved detection with the inclusion of anterior nares and hands (13, 14).
The aforementioned reasons are justification for why rapid and accurate detection of C. auris colonization is critical for the initiation of proper infection prevention measures and contact precautions to limit the spread of this fungal pathogen in healthcare settings. Recognizing the urgency of early detection, this study aims to assess a diagnostic tool that may improve the detection and management of C. auris. This study was designed to assess the performance of the Simplexa C. auris Direct Assay, a real-time polymerase chain reaction (RT-PCR) assay intended for use on the LIAISON MDX (15), by examining clinical accuracy, analytical sensitivity, and cross-reactivity during implementation in a clinical laboratory. This study also examined the potential impact of proper handling on environmental contamination with C. auris.
MATERIALS AND METHODS
Diasorin C. auris IVD
The Simplexa C. auris Direct is an FDA-approved real-time PCR assay designed for the direct amplification and qualitative detection of Candida auris DNA from composite axilla/groin swabs. This system utilizes the LIAISON MDX platform (integrated with LIAISON MDX Studio Software), the Direct Amplification Disc, the Simplexa C. auris Direct Assay, the Simplexa C. auris Sample Prep Solution, and essential laboratory consumables. The assay employs specific primers and FAM-labeled fluorescent probes to amplify both C. auris DNA and the assay internal control, ensuring reliability of its results. The assay targets the C. auris ITS 2 rRNA gene. A C. auris DNA positive control is included to aid in the detection of potential PCR failures or inhibition. A “No Template Control” (NTC) consisting of fresh Liquid Amies media and a positive C. auris DNA control were both run each day before testing to verify assay performance in the selected specimen media (13). The Simplexa C. auris Direct assay was performed according to the manufacturer’s instructions for use. Briefly, 50 µL of reaction mix was loaded onto the Direct Amplification Disc. Next, 50 µL of the patient sample was transferred to the Sample Prep Solution vial and mixed thoroughly by pipetting up and down, then 50 µL of the mixed sample was loaded onto the Direct Amplification Disc. The reaction wedge was sealed using the disc’s adhesive foil prior to being run on the LIAISON MDX. Results were produced approximately 105 min later.
Diasorin C. auris LDT
The C. auris Primer Pair LDT utilizes Diasorin Molecular’s C. auris Primer Pair, Fungal Lysis Solution and Simplexa Extraction and Amplification primers and control, with fluorescent probe technology and real-time PCR amplification and detection on the LIAISON MDX system. Each probe molecule is affixed with a fluorophore and a quencher. The C. auris primer pair is an analyte specific reagent (ASR) introduced in 2019 for amplifying a well-conserved region of the ITS2 region in the rRNA gene for Candida auris with a FAM labeled probe, forward primer, and reverse primer in Tris-EDTA buffer. First, 5 µL of Fungal Lysis Buffer is added to 50 µL of patient sample, and then the mix is incubated at 60°C for 30 min. During the incubation period, a master mix is made using C. auris Primer Pair solution, SEAC (IC) Primer Pair control, SEAC Control DNA (IC), and Nuclease-free water. After the incubation period, exactly 8 µL of master mix is then added to a reaction well on a 96-well disc, followed by 2 µL of fungal lysate. Each reaction wedge is then covered with Universal Disc Cover Tape prior to being run on the LIAISON MDX for 45 cycles. Results were produced approximately 73 min later.
DSQ C. auris LDT
The DSQ Alert Candida auris Assay is a real-time PCR LDT performed on the Cobas 5800 System. Specimens were processed using the Cobas omni Utility Channel Reagent Kit, which includes lysis, magnetic particle-based purification, and the elution of nucleic acids. The assay targets a 124-bp region of the ITS2 rRNA gene using specific primers and FAM-labeled probes provided in the DSQ Alert Primer and Probe Mixes kit purchased from ELITechGroup. Myriad consumables were replaced prior to each run, including tip racks, analyte-specific reagents, negative control racks, processing, liquid waste, and amplification plates, alongside wash, lysis, and diluent reagents. An internal control was co-extracted and co-amplified to monitor assay performance. Amplification and detection occurred in a closed system, using fluorescent signals generated during probe cleavage. The master mix includes dUTP and AmpErase enzymes to prevent carryover contamination. The cycling parameters of the assay include 45 cycles of denaturation and annealing steps, lasting 5 and 25 s, respectively, at temperatures of 91°C and 58°C. The system automated all sample preparation, PCR amplification, detection, and data analysis, with each 24-well plate accommodating 350 µL from up to 22 samples alongside an external control and an NTC. Results were produced approximately 2.5 h after fully loading the instrument.
Clinical accuracy
To evaluate the clinical accuracy of the Diasorin C. auris IVD assay, a total of 40 previously characterized composite axilla/groin swab specimens were tested, including 20 positive and 20 negative specimens. Swabs were collected using either BD ESwab or Copan ESwab in 1 mL liquid amies. Each positive sample was retrospectively obtained from frozen specimens. All clinical specimens were collected from patients with risk factors for C. auris colonization. Specimens were de-identified and assigned unique identification numbers to ensure the operator was blinded to both the subject identity and comparator results before testing. Culture served as the primary reference method for the primary analysis. A secondary analysis was also performed comparing different PCR methods to each other.
Culture comparator
Retrospective specimens were utilized in this study that had been stored at −70°C. The retrospective specimens were thawed and plated onto chromogenic agar that allows for the growth and differentiation of C. auris as well as other Candida species (Hardy Chromagar, Cat# G343) using 10 µL of the specimen and streaked for isolation and incubated at 37°C. Candidate colonies exhibiting color changes characteristic of C. auris were confirmed by mass spectrometry using the Bruker MALDI-ToF (Library version IVD MBT Compass 4.1.100). All Diasorin C. auris IVD assay specimens with an invalid result or error were re-tested once to obtain a valid result. For specimens that were Diasorin C. auris IVD PCR-positive but culture-negative, culture plates were incubated for 2 additional days to ensure the lack of detectable growth.
Analytical sensitivity/limit of detection
To evaluate the analytical sensitivity of the Diasorin C. auris IVD assay, experiments were performed to identify the assay’s limit of detection (LoD) in a negative bilateral axilla/groin swab matrix. Analytical sensitivity was determined by creating a series of serial dilutions using a commercial C. auris stock (Zeptometrix Cat# 0804386) that was quantified to contain 10^9^ CFU/mL by viable plate count. This stock was diluted from 10^9^ to 10^2^ CFU/mL, and each dilution magnitude was tested in triplicate. Then, 20 replicates were performed at the lowest concentration detected to determine whether that concentration represented the LoD.
Analytical specificity/cross-reactivity
The analytical specificity, or cross-reactivity, of the Diasorin C. auris IVD assay was evaluated using a panel of 14 organisms that are either closely related to C. auris or anticipated to be present in the axilla or groin regions. The organisms representing bacteria and fungi are A. fumigatus, C. albicans, C. glabrata, C. parapsilosis, C. dubliniensis, C. lusitaniae, C. kruseii, C. guillermondii, C. tropicalis, C. neoformans, E. coli, S. cerevisiae, S. epidermidis, and T. rubrum. Quantified Zeptometrix stocks were diluted to clinically relevant concentrations (10^5^–10^6^ CFU/mL) in Liquid Amies medium and then tested in triplicate.
Stability
The stability of bilateral axilla/groin swabs in Liquid Amies media (BD ESwab) and its potential impact on the performance of the Diasorin C. auris IVD Assay was also evaluated. In order to examine specimen stability, a C. auris standard contrived to 5× LoD was prepared in triplicate and aliquoted for various time points. The aliquots were stored at room temperature (22–25°C), refrigerated (2–8 °C), and frozen (<−70°C) and then tested in triplicate at the time points outlined (Table 1).
Environmental swab testing
The sites designated for swab testing were the inside of the instrument and the outside of the instrument. The areas swabbed outside of the instrument include the instrument’s lid, open button, logos, mouse keys and body, laptop keys, body, and trackpad, bench space, pipettes, pipette boxes, and the surface of the biosafety cabinet. The inside of the instrument was also swabbed in areas like the central testing platform, under the removable magnetic ring, the ring itself, as well as all openings, holes, and crevices within. Swabs were collected using either BD ESwab or Copan ESwab in 1 mL Liquid Amies. Swab specimens were then tested on the Direct Amplification Disc as per the Simplexa C. auris Direct Assay’s instructions for use.
Statistical analysis
Positive Percent Agreement (PPA), Negative Percent Agreement (NPA), Probit, Cohen’s kappa, diagnostic accuracy, and two-sided (upper/lower) 95% confidence intervals (CI) were calculated using Microsoft Office Excel 365 MSO software (Microsoft, Redmond, WA) and Prism GraphPad software (GraphPad Software Inc., San Diego, CA, USA). The PPA was calculated as TP/(TP + FN) × 100, the NPA was calculated as TN/(TN + FP) × 100, where TP is true-positive results, FN is false-negative results, TN is true-negative results, and FP is false-positive results. Probit analysis was used for the CFU/mL determination of the analytical sensitivity study. Diagnostic accuracy was calculated as [(TP + TN)/(TN + FP + FN + TP)]. Cohen’s kappa values (κ) were calculated as a measure of the overall agreement, categorized as almost perfect (>0.90), strong (0.8 to 0.9), moderate (0.6 to 0.79), weak (0.4 to 0.59), minimal (0.21 to 0.39), or none (0–0.20).
RESULTS
Comparison of assay accuracy
Specimens selected for testing using the Diasorin C. auris IVD assay on the LIAISON MDX and for comparator C. auris culture were 40 previously characterized C. auris specimens. Specimens were previously determined positive or negative using the Diasorin C. auris LDT on the LIAISON MDX and/or the DSQ C. auris LDT on the Cobas 5800 with testing platforms evenly distributed across 20 previously positive C. auris specimens and 20 previously negative C. auris specimens. The sensitivity of the Diasorin C. auris IVD Assay compared to the gold-standard reference method of culture followed by MALDI identification was 100% (95% CI 0.82–1), and the specificity was 90% (95% CI 0.72–0.98) (Table 2). There were two retrospective specimens that were detected by the Simplexa C. auris Direct IVD assay but exhibited no growth in culture. Both of these specimens were also detected by both PCR-based LDT methods. The diagnostic accuracy of the Simplexa C. auris Direct Assay compared to the culture comparator was 95% (95% CI 0.83–0.99), showing a high rate of accuracy. The Cohen’s kappa value was 0.9 (95% CI 0.76–1), demonstrating strong agreement.
The clinical accuracy of the Diasorin C. auris IVD Assay was also compared to the two in-house C. auris LDT methods (Table 3). The Diasorin C. auris IVD assay demonstrated perfect agreement with the DSQ Alert LDT assay across both positive and negative samples with a PPA of 100% (20/20, 95% CI 0.83–1) and NPA of 100% (20/20, 95% CI 0.83–1). The corresponding Cohen’s kappa value for this assay comparison was 1.00, indicating perfect overall agreement. For the comparison between the Diasorin C. auris IVD and the Diasorin C. auris LDT, only positive samples were available. The PPA between these two assays was 100% (13/13, 95% CI 0.77–1). Both NPA and Cohen’s kappa values could not be calculated for this comparison because the negative retrospective specimens used in this study were not run on the Diasorin C. auris LDT, making chance-corrected agreement between these two assays uninterpretable. However, the consistent positive agreement observed across all assay comparisons provides strong initial evidence of consistent performance across assay platforms for C. auris positive samples and the Direct IVD assay’s diagnostic concordance.
TABLE 3: Diasorin C. auris IVD vs LDTa
Limit of detection analysis
We next determined the limit of detection for the Diasorin C. auris IVD assay. We had previously determined that the LoD for the DSQ C. auris LDT was 100 cp/mL when run on the Cobas 5800 and that the limit was 1,000 cp/mL for the Diasorin C. auris LDT run on the LIAISON MDX (data not shown). In contrast to the previous LoD experiments done for our LDT assay validations, which utilized inactivated C. auris stock solutions quantified in copies/mL, our experiments were conducted using a live C. auris stock solution quantified in CFU/mL by plating and counting prior to testing in order to account for the viability of our control organism. We diluted our C. auris stock solution from 10^9^ CFU/mL to a clinically relevant concentration of 10^5^ CFU/mL and then tested each 10-fold dilution in triplicate until we achieved our first dropout value at 10^2^ CFU/mL. We then tested 20 separate replicates at the lowest concentration where amplification was detected in all three dilution replicates. The detection of C. auris in 19/20 (95%) replicates detected was considered acceptable for the limit of detection of the assay. We performed serial dilutions and testing of 20 replicates until less than 95% detection occurred. We, thus, determined the LoD of the assay to be 702 CFU/mL (Table 4). As an additional investigation, we also conducted a probit analysis using data from three independent iterations of the Diasorin C. auris IVD assay’s sensitivity analysis, which would refine the LoD to 317 ± 56 CFU/mL based on the detection rates across varying concentrations (data not shown).
Analytical specificity
We characterized the specificity of the assay by performing the Diasorin C. auris IVD assay against a panel of known positive specimens containing various yeasts, molds, and bacteria. These organisms included multiple species of Candida, as well as Cryptococcus, Saccharomyces, Aspergillus, Trichophyton, Escherichia, and Staphylococcus. Aside from Candida auris, none of these organisms produced positive results on the Direct assay. These findings indicate that no cross-reactivity was observed for any of these targets, yielding an analytical specificity of 100% (Fig. 1).
A total of 14 contrived standard solutions of clinically relevant fungi and bacteria were tested using the Simplexa C. auris direct assay. Zero is depicted as no amplification on this chart.
Specimen stability
We evaluated the potential impact of stability of specimens stored at room temperature, refrigerated, or frozen at ≤−70°C on the performance of the Diasorin C. auris IVD assay. Notably, the room temperature experiments expand upon the timeframe that is currently allowed in the assay instructions for use (1). To perform this analysis, we contrived a set of specimens that were spiked with a live C. auris standard at 5× the LoD in a C. auris negative axilla/groin matrix in Liquid Amies and stored under various clinically relevant conditions for different time periods. The specimens were tested on the Simplexa C. auris Direct assay at the relative timepoints for each temperature condition, and the resulting CT values were recorded. We found that for all conditions over the course of the 30-day study, all expected positive results remained positive, with a trend in lower CT values over time (Fig. 2).
To assess specimen stability, triplicates of contrived C. auris samples were prepared in a negative bilateral axilla/groin swab matrix with liquid amies at 5× LOD and stored at (A) room temperature (22–25°C), (B) refrigerated (2–8°C), and (C) frozen at ≥ 70°C. The assay successfully identified C. auris under all three environmental conditions.
Environmental colonization
Standard lab quality monitoring practices to monitor for false positivity include performance of wipe testing to monitor for environmental colonization (16). Over a 14-day period, we swabbed the interior of the LIAISON MDX instrument, the exterior of the instrument, the surfaces of the biosafety cabinet, and all tools used where the experiments were being conducted to determine whether any of those surfaces may be exposed to C. auris that could contaminate the experiments. The swabs were collected in a C. auris negative axilla/groin matrix in Liquid Amies medium and tested using the Simplexa C. auris Direct assay on the LIAISON MDX. Each of the tests produced negative results (Table 5), indicating the absence of detectable contaminating nucleic acids on the instrument and in the working area despite the high numbers of C. auris amplification experiments taking place on a regular basis. These data suggest that as long as standard operating procedures and proper decontamination protocols are followed, the risk of environmental contamination with C. auris is minimal.
DISCUSSION
This study is the first to assess the performance of the Diasorin Simplexa C. auris Direct assay (Diasorin C. auris IVD assay) in comparison to the current gold-standard method of culture followed by MALDI-TOF identification for the detection of C. auris colonization in clinical specimens. The Diasorin C. auris IVD assay demonstrated good agreement with a culture-based method. While there were two culture-negative specimens, it is notable that these specimens were both positive on each of the PCR-based methods examined in this study. The PCR-concordance but culture negativity could be explained by a higher sensitivity of PCR compared to culture in specimens with low numbers of organisms. Additionally, this study utilized retrospective frozen specimens, and freezing may have had a negative effect on the viability of the organisms. Lastly, our protocol for culture omitted the up to 5 day broth enrichment step outlined in the CDC procedure for isolation which may have reduced our culture sensitivity (17). Overall, the agreement between culture and the Diasorin C. auris IVD assay was high, suggesting this is a sensitive and specific method for the detection of C. auris colonization.
Additionally, this is the first study to compare the diagnostic accuracy of the Diasorin C. auris IVD assay to two lab-developed PCR tests in our lab, the DSQ C. auris LDT, and the Diasorin C. auris LDT. The Diasorin C. auris IVD assay demonstrated 100% clinical agreement with all C. auris positive samples tested on both LDTs examined in this study, providing great confidence that the Diasorin Simplexa C. auris Direct assay will provide results that are at least equivalent to other tests we already have used clinically at our institution.
Our experiments found a LoD of 702 CFU/mL, which is within the logarithmic range of the LoD described in the package insert (127 CFU/mL for Clade I, 260 CFU/ml for Clade IV)^13^. Given we still observed 85% detection of replicates at 233 CFU/mL, it is not unreasonable to hypothesize that our observed LoD could be lower if we had elected to test concentrations lower than 702 CFU/mL, and indeed, a sensitivity analysis of all of our data suggests it may be closer to 317 CFU/mL. More importantly, our previous LDT validations were performed with inactivated stock solutions quantified in copies/mL, which do not provide an assessment of the detection of live viable organisms. While the detection of both viable and non-viable organisms may be valuable in a screening assay, it is ultimately only viable organism that can lead to C. auris infection.
One of the critical features of any PCR-based test to detect C. auris is specificity, because a plethora of different microbes are known to colonize the skin including various yeasts, which can be misidentified as a number of different organisms when using traditional phenotypic methods for yeast identification. Inaccurate detection due to cross-reactivity could lead to unnecessary patient isolation, treatment errors, or misclassification of colonization status (18). Given the high microbial diversity in commonly surveilled anatomical regions like the axilla and groin, a high caliber of assay specificity is critical in clinical practice. In support of this need, we observed no off-target amplification from other Candida species or any of the phylogenetically related fungi and bacteria included in our panel of potentially cross-reactive organisms, indicating that the assay is not easily affected by off-target amplification events or organisms.
Given the antifungal drug resistance of C. auris, and its ability to easily colonize patients and patient care areas, there may exist concern in a clinical lab about contamination of lab space with C. auris. Additionally, labs accredited by the College of American Pathologists are required to monitor existing molecular testing for false positive results, including with wipe testing if necessary. Our lab routinely handles and grows C. auris and works with positive patient specimens. Environmental testing of the areas where we handle specimens for testing both before and after testing showed no evidence of C. auris positivity by PCR on the Diasorin C. auris IVD assay, affirming our lab practices.
As diagnostics for C. auris colonization continue to evolve, infection prevention practices evolve along with them and may dictate an ever-increasing need for rapid diagnostics. At our institution, we have experienced that need firsthand and despite our efforts to respond to the growing need to provide rapid diagnostics dictated by inpatient cohorting (19), disposition (20), and an ongoing need for contact precautions (21) that may affect the patient’s stay from both a cost perspective (22, 23) and a mental health perspective (24), we continue to find ourselves in need of an additional solution to provide rapid solutions for C. auris colonization diagnostics. Patients are often unable to transfer to an inpatient room from the Emergency Department or to discharge to a facility until the results of C. auris screening are back. We had settled upon the DSQ C. auris LDT on the open channel on the Roche Cobas 5800 platform because it allowed us to perform the assay twice daily in large, batched runs. Unfortunately, we have found we need to run the assay even more frequently to prevent delays in transitions of care. The Diasorin Simplexa Direct IVD (Diasorin C. auris IVD) assay allows for smaller run sizes in batches of 1–8, with turn-around times around 105 min. The Diasorin C. auris IVD assay offers an additional advantage over our previous Diasorin C. auris LDT with the absence of a separate pre-analytical step, and because it is FDA-approved allows for a far simpler verification and validation to onboard the assay in a clinical lab, even if multiple instruments are necessary.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Satoh K, Makimura K, Hasumi Y, Nishiyama Y, Uchida K, Yamaguchi H. 2009. Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital. Microbiol Immunol 53:41–44. doi:10.1111/j.1348-0421.2008.00083.x 19161556 · doi ↗ · pubmed ↗
- 2Vallabhaneni S, Kallen A, Tsay S, Chow N, Welsh R, Kerins J, Kemble SK, Pacilli M, Black SR, Landon E, et al.. 2017. Investigation of the first seven reported cases of Candida auris, a globally emerging invasive, multidrug-resistant fungus-United States, May 2013-August 2016. Am J Transplant 17:296–299. doi:10.1111/ajt.1412128029734 · doi ↗ · pubmed ↗
- 3CDC. 2024. Tracking Candida auris. Available from: https://www.cdc.gov/fungal/candida-auris/tracking-c-auris.html
- 4CDC. 2023. Increasing Threat of Spread of Antimicrobial-resistant Fungus in Healthcare Facilities
- 5Ahmad S, Asadzadeh M. 2023. Strategies to prevent transmission of Candida auris in healthcare settings. Curr Fungal Infect Rep 17:36–48. doi:10.1007/s 12281-023-00451-736718372 PMC 9878498 · doi ↗ · pubmed ↗
- 6Vaseghi N, Sharifisooraki J, Khodadadi H, Nami S, Safari F, Ahangarkani F, Meis JF, Badali H, Morovati H. 2022. Global prevalence and subgroup analyses of coronavirus disease (COVID-19) associated Candida auris infections (CA Ca): a systematic review and meta-analysis. Mycoses 65:683–703. doi:10.1111/myc.1347135555921 PMC 9347948 · doi ↗ · pubmed ↗
- 7WHO. 2022. WHO fungal priority pathogens list to guide research, development and public health action, W.H. W.H. Organization, Editor
- 8Antibiotic Resistance Threats in the United States 2019. 2019. CDC: Atlanta, GA U.S. Department of Health and Human Services