Evaluation of the Bruker MALDI Biotyper (MBT) subtyping module for detection of Klebsiella pneumoniae carbapenemase (KPC) in Enterobacterales in a Canadian clinical microbiology laboratory
Emma Finlayson-Trick, Heather Glassman, Jasmine Ahmed-Bentley, Xinhe Liu, Linda Tsui, Lori Sung, Charlene Porter, Claudine Desruisseaux, Valery Lavergne, Suefay Liu, Jennifer Tat, Anthony Lieu, Aruna Uma Chandran, Marthe K. Charles

TL;DR
This study evaluates a MALDI-ToF tool's ability to detect KPC-producing Enterobacterales, finding it highly specific but with low sensitivity.
Contribution
The study expands the validation of MALDI-ToF for KPC detection in a Canadian clinical setting with a diverse isolate collection.
Findings
The MBT Module detected KPC with 100% specificity but only 15.5% sensitivity.
It detected 40% of KPC-2 isolates but none of the KPC-3 isolates.
A positive result reliably predicts KPC presence, but negative results are unreliable.
Abstract
Early detection of Klebsiella pneumoniae carbapenemase (KPC)-producing Enterobacterales enables prompt initiation of appropriate antimicrobial therapy and infection prevention and control measures. The matrix-assisted laser desorption/ionization time-of-flight (MALDI-ToF) Biotyper (MBT) Subtyping Module (Bruker Daltonics) uses a characteristic spectral peak at ~11,109 m/z to identify KPC-producing Enterobacterales. The aim of this study was to assess the ability of the MBT Module to detect KPC among a variety of clinical and reference (AR Bank) Enterobacterales isolates. Detection of KPC was compared between the MBT Module and a laboratory-developed real-time KPC PCR. Of the 93 isolates tested, 58 (62.4%) were positive for KPC by PCR (39 clinical and 19 AR bank isolates), and 35 were negative. Among the KPC-positive PCR isolates, nine (seven clinical and two AR bank) also tested…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
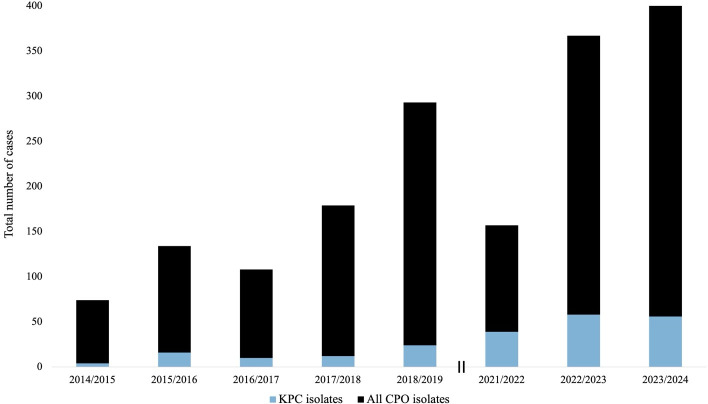 Fig 1
Fig 1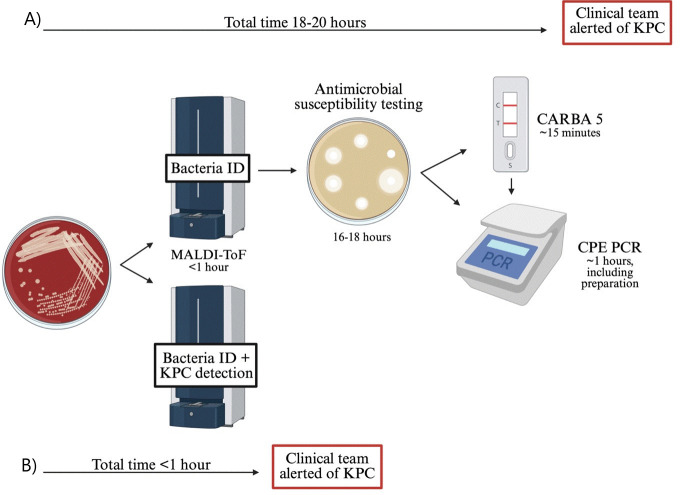 Fig 2
Fig 2| Species | Total isolates | KPC-producing isolates | Non-KPC producing isolates |
|---|---|---|---|
| Clinical samples | |||
| | 24 | 15 | 9 |
| | 17 | 12 | 5 |
| | 11 | 4 | 7 |
| | 7 | 6 | 1 |
| | 6 | 1 | 5 |
| | 2 | 0 | 2 |
| | 1 | 1 | 0 |
| | 1 | 0 | 1 |
| AR Bank samples | |||
| | 13 | 11 | 2 |
| | 5 | 2 | 3 |
| | 4 | 4 | 0 |
| | 1 | 1 | 0 |
| | 1 | 1 | 0 |
| Name | Sequence (5′ → 3′) | Reporter/quencher | [Final] (μM) |
|---|---|---|---|
| KPC Forward |
| 0.2 | |
| KPC Reverse |
| 0.2 | |
| KPC Probe |
| MAX/ZEN/IFBQ | 0.15 |
| KPC detected via PCR/total number of isolates | KPC detected via MBT module | Sensitivity (%) | |
|---|---|---|---|
| 26/37 | 2 | 7.7 | |
|
| 13/18 | 2 | 15.4 |
|
| 7/8 | 5 | 71.4 |
|
| 6/16 | 0 | 0 |
| 5/10 | 0 | 0 | |
|
| 1/1 | 0 | 0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Identification and Susceptibility Testing · Antibiotic Resistance in Bacteria · Neutropenia and Cancer Infections
INTRODUCTION
Carbapenemase-producing Enterobacterales (CPE) present a significant threat to global health (1). Located on mobile genetic elements, such as plasmids, carbapenemases are easily transferred among bacteria, facilitating the spread of multi-drug resistance (2). Historically in Canada, CPE infections were attributed to international travel, but in recent years, an increasing number of cases have been associated with domestic acquisition (3–5). Klebsiella pneumoniae carbapenemase (KPC), New Delhi metallo-β-lactamase (NDM), and oxacillinase 48 (OXA-48) account for 86–96% of carbapenemases in Canada (6). Nationally, KPC is implicated in more than half of all CPE infections (6). In British Columbia, while the total number of KPC cases is relatively low, the case count has been steadily increasing over the last decade (Fig. 1) (7, 8).
Annual number of cases due to KPC-producing organisms (blue) compared to number of cases due to all carbapenemase-producing organisms (CPO, black) in British Columbia, Canada. The double vertical line indicates a gap in surveillance data between 2019–2021. The figure was created using surveillance data collected from the Provincial Infection Control Network of British Columbia (8).
In Canada, most clinical microbiology laboratories routinely use matrix-assisted laser desorption/ionization time-of-flight (MALDI-ToF), a mass spectrometry-based method, to rapidly identify organisms with high sensitivity and specificity. Recent studies have demonstrated that in addition to identification, MALDI-ToF can be leveraged to detect antibiotic resistance genes, including carbapenemases like KPC (9–11). This approach has the potential to significantly shorten time to KPC detection, as current investigations, such as the NG-Test CARBA 5 (Hardy Diagnostics, Santa Maria, CA) or CPE PCR, are only initiated after the bacteria have been identified, and the susceptibility pattern has been confirmed (Fig. 2). The MALDI Biotyper (MBT) Subtyping Module (MBT Module, Bruker Daltonics) uses a characteristic spectral peak at ~11,109 m/z to identify KPC among Citrobacter freundii, Enterobacter aerogenes, Enterobacter asburiae, Enterobacter cloacae, Enterobacter kobei, Enterobacter ludwigii, Escherichia coli, Klebsiella aerogenes, Klebsiella oxytoca, Klebsiella pneumoniae, Klebsiella variicola, and Serratia marcescens (12). This peak corresponds to a protein encoded by the p019 gene located adjacent to blaKPC, which is associated with 39% of KPC-2 isolates and 4% of KPC-3 isolates (13). As such, studies indicate that KPC detection by MALDI-ToF has high specificity (99%) but low sensitivity (42–85%) (14, 15).
Comparison between the current workflow and the MBT Module for KPC detection. Following subculture, bacterial species are identified via MALDI-ToF. In the current workflow (A), KPC detection and clinical notification occur only after susceptibility testing and specific carbapenemase testing with CARBA 5 and/or CPE PCR. The MBT Module (B) enables earlier detection of KPC at the time of bacterial identification, allowing for timely clinical notification (about a day earlier than the current pathway).
It is crucial that clinical microbiology laboratories quickly and accurately detect KPC-producing Enterobacterales so that physicians can initiate appropriate broad-spectrum empiric antibiotics, such as meropenem-vaborbactam, ceftazidime-avibactam, imipenem-cilastatin-relebactam, or cefiderocol, which is necessary for patient survival (16, 17). Moreover, early detection of KPC enables implementation of appropriate infection prevention and control (IPAC) precautions, which is key for controlling the spread of KPC in hospital or long-term care facilities (18). Currently, few publications have used the MBT Module to detect KPC beyond Klebsiella species (9–11, 13–15, 19, 20). Moreover, none of the publications in this field have involved Canadian clinical isolates. This study involved validating the MBT Module for KPC detection in a Canadian hospital laboratory using a variety of Enterobacterales isolates from clinical samples and the Antimicrobial Resistance Isolate Bank (AR Bank) (21).
MATERIALS AND METHODS
Preparation of isolates for testing
A data set of Enterobacterales isolates was selected to reflect the historic trends of KPC in the hospital clinical laboratory and was based on prior phenotypic and molecular results that demonstrated either the presence or absence of KPC (Table 1). This frozen data set included 70 clinical isolates (both patient specimen and surveillance samples) from a hospital laboratory. Clinical isolates were limited to one per patient and were selected between May 2022 and August 2024. The remainder of the data set included 23 isolates from the AR Bank (gram-negative carbapenemase detection [CarbaNP] and Enterobacterales carbapenemase diversity [CRE] panels). Isolates were subcultured twice on 5% sheep blood agar prior to testing.
MALDI-ToF MS testing
Culture plates with 24 ± 8 h of growth were accepted for MALDI-ToF MS testing. MALDI-ToF MS was performed as per the manufacturer’s instructions. All isolates were tested on both the MALDI Biotyper Sirius and Smart System (Bruker Daltonics, Billerica, MA). The mass spectral readouts were obtained using MBT HT Client (Version 5.1.410.9032). The detailed report was reviewed to confirm isolates that were identified as KPC-positive. As per the manufacturer’s guidelines, KPC subtyping was not completed on isolates with low identification scores. Therefore, any isolate with an ID score < 2.0 were re-spotted and re-tested the same day.
KPC PCR
This multiplex real-time colony PCR was used as the gold standard to confirm the presence or absence of KPC in the tested isolates. This PCR was developed by the British Columbia Center for Disease Control Public Health Laboratory (22). Primers and a fluorescent probe (outlined in Table 2) were obtained from Integrated DNA Technologies (Coralville, IA).
Approximately one to three bacterial colonies from each culture plate were inoculated into tubes with sterile water (turbidity approximately 0.5 McFarland standard). The tubes were then heated at 100°C for 8 minto promote bacterial lysis.
As per the manufacturer’s instructions, each PCR reaction contained TaqMan Fast Advanced Master Mix (Life Technologies, Burlington, ON), RNase-free water, primers and probe, and sample lysate. Real-time PCR was conducted on the ABI 7500 platform (ThermoFisher, Waltham, MA) with the recommended fast thermal cycling conditions (35 cycles total). The PCR reaction was considered valid if the positive control cycle threshold (Ct) value was between 20 and 30, and all the negative controls were negative for KPC. An isolate was considered positive for KPC if the Ct value was between 10 and 30.
Analysis and preparation of figures
Performance was evaluated by comparing the MBT Module against a real-time PCR assay as the reference standard. Sensitivity was calculated as the percentage of the isolates detected as KPC-positive by the MBT Module among those positive by KPC PCR. Specificity was calculated as the percentage of the isolates detected as KPC-negative by the MBT Module among those negative by KPC PCR. Positive predictive value (PPV) was determined by calculating the proportion of isolates truly carrying KPC (true positives) by the KPC-positive isolates detected via the MBT Module (total positive tests). Negative predictive value (NPV) was determined by calculating the proportion of isolates lacking KPC (true negatives) by the total number of negative tests (true and false negatives). The figure was created in BioRender (2024).
RESULTS
In total, 93 isolates (clinical and AR Bank) were tested, of which 58 (62.4%) were confirmed to carry a gene for KPC via PCR (Table 3). Of those PCR-positive isolates, nine (seven clinical, two AR Bank) were identified as KPC-positive via the MBT Module. There were no discordant results between the Sirius and Smart systems. Overall sensitivity was 15.5% (9/58), and specificity was 100%. There were no instances where the MBT Module result was positive, but PCR was negative. As such, the PPV of the MBT module was 100%. The NPV of the MBT module was 41.7% (35 isolates were true negatives; 49 isolates were false negatives).
KPC types were only available for the AR Bank isolates of which five were KPC-2 and 14 were KPC-3. The MBT Module identified two AR Bank isolates as KPC positive, both of which were KPC-2. As such, the frequency of positive KPC identification was 40% in the KPC-2 group and 0% in the KPC-3 group.
DISCUSSION
In this study, the MBT Module had a low sensitivity (15.5%) but high specificity (100%) and PPV (100%) for the detection of KPC-producing Enterobacterales. These results support similar findings (42% sensitivity, 100% specificity) published by Cuello et al. (13) who tested more than 700 clinical Klebsiella isolates from the United States and South America (13). This study expanded upon the work of Cuello et al. (13) by contributing geographic representation from Canada and by analyzing the performance of the MBT Module for KPC detection among Klebsiella and non-Klebsiella bacterial isolates.
In addition to the methods used in this study, there are other automated approaches for rapid KPC detection in Enterobacterales. A study by Centonze et al. (19) similarly targeted the ~11,109 m/z peak but used the MALDI-ToF Vitek MS system from BioMérieux (19). In their sample of 176 KPC-positive clinical isolates, they reported high sensitivity (99.4%) and specificity (100%) for KPC detection using the MALDI-ToF Vitek MS System (19). The authors noted, however, that the high sensitivity and specificity may be a result of testing isolates derived from the same clone (19). Other groups have also improved the sensitivity of detection by targeting the mature KPC protein (~28,643–28,731 Da) rather than the biomarker (~11,109 Da). For example, Costa et al. (14) reported a sensitivity and specificity of 100% for the detection of the mature KPC protein in their data set of clinical blood cultures, short-term cultures, and colonies, but sensitivity dropped to 63% when the biomarker was targeted (14). Similarly, Moreira et al. (20) reported a sensitivity and specificity of 98.1 and 97.9%, respectively, when they targeted the mature KPC protein in their sample of clinical Enterobacterales isolates (20). Comparing detection of the mature protein with the p019 biomarker was not part of this study; meanwhile, it could represent a future research direction. As such, different approaches can be taken for KPC detection depending on the availability of equipment in the clinical laboratory.
This validation examined the ability of the MBT Module to detect KPC among a variety of Enterobacterales. The distribution of Enterobacterales species was selected to reflect the isolates previously observed in the hospital’s clinical laboratory between 2022 and 2023, whereby among 42 KPC-producing Enterobacterales, 19 were K. pneumoniae (45 and 39% in the present study), and six were C. freundii complex (14 and 19% in the present study). In the literature, the presence of p019 is more commonly detected in Klebsiella species compared to Citrobacter species, although a far fewer number of Citrobacter isolates have been studied (10, 23, 24). Similar to previous publications, the MBT Module detected KPC in some of the K. oxytoca, C. freundii, and K. pneumoniae isolates. As such, the composition of Enterobacterales species used in this study may have contributed to the low MBT Module sensitivity. Furthermore, unlike Centonze et al. (19) who detected 92.3% (12/13) of KPC-producing E. coli in their data set, the MBT Module in this study did not detect any KPC-producing E. coli isolates (19). It is possible that the KPC-producing E. coli isolates in this study differ significantly in their carriage of p019 due to geographic variation. In a study of KPC-positive K. pneumoniae isolates across Europe, Gato et al. (25) observed wide geographic variation of p019 detection from 100% in France and Ireland to 0% in Portugal and Poland (25). As p019 is part of a mobile genetic element, it is feasible that through selective pressure, many of this study’s isolates maintained the resistance gene (blaKPC) but lost p019 (25). Consequently, the low MBT Module sensitivity seen here may indirectly reflect a local plasmid reservoir that lacks p019. Otherwise, the MBT Module did not detect KPC in E. bugandensis and K. ozaenae, but blaKPC is not automatically detected in these bacteria as noted in the Bruker manual. While the sample size was sufficient for validation in the clinical laboratory, the small number of isolates was a limitation that meant that some bacterial species were rarely tested. As such, these findings require external evaluation for confirmation.
Future studies are needed to better understand the characteristics of KPC detection by the MBT Module. In the laboratory, it remains unclear if there are other factors, besides the presence/absence of p019, influencing KPC detection among the various Enterobacterales species. Furthermore, additional work is needed to evaluate how KPC detection by the MBT Module impacts quality indicators in the microbiology laboratory and patient care. While this study combined surveillance and patient specimens, it would be interesting to tease apart these sample types when evaluating impact given the different IPAC implications. Finally, this work with KPC invites the opportunity to explore more targets for the MBT Module, including other carbapenemases like NDM and OXA-48 (26, 27).
In conclusion, despite a low sensitivity, the automated MBT Module had high specificity and PPV for the detection of KPC-producing Enterobacterales, making it a potentially useful adjunctive "rule-in" tool at the time of MALDI-ToF identification, prior to the availability of conventional susceptibility testing (10, 28, 29). Many clinical laboratories already use MALDI-ToF for bacterial identification; therefore, detection of KPC by the MBT Module would not significantly change the current workflow and would not require the purchase of an additional instrument. It is important to note that due to the low sensitivity, all negative MBT Module results would still require routine testing to evaluate for KPC, as would positive results to evaluate for the presence of additional CPE genes like NDM or OXA-48. Nevertheless, KPC detection at the time of bacterial identification has the potential to critically impact patient care by facilitating an earlier switch to more appropriate antibiotics and ensuring suitable IPAC precautions.
Supplementary Material
Reviewer comments
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organisation. 2024. WHO Bacterial Priority Pathogens List, 2024: bacterial pathogens of public health importance to guide research, development and strategies to prevent and control antimicrobial resistance.
- 2Caliskan-Aydogan O, Alocilja EC. 2023. A review of carbapenem resistance in Enterobacterales and its detection techniques. Microorganisms 11:1491. doi:10.3390/microorganisms 1106149137374993 PMC 10305383 · doi ↗ · pubmed ↗
- 3Canadian Nosocomial Infection Surveillance Program. 2023. Healthcare-associated infections and antimicrobial resistance in Canadian acute care hospitals, 2017–2021. Can Commun Dis Rep 49:235–252. doi:10.14745/ccdr.v 49i 05a 0938425696 PMC 10903608 · doi ↗ · pubmed ↗
- 4Li J, Walkty A, Lagacé-Wiens P, Karlowsky J, Zhanel G. 2025. The state of antimicrobial resistance of Gram-negative bacilli in Canada. Tropical Med 10:115. doi:10.3390/tropicalmed 10040115 · doi ↗
- 5Jamal AJ, Tijet N, Mc Geer A, Baqi M, Borgia S, Ciccotelli W, Farshait N, Katz K, Mehta M, Goneau L, Mertz D, Small LN, Melano R. 2023. 2468. The genomic epidemiology of carbapenemase-producing Enterobacterales (CPE) in Ontario, Canada, 2016. Open Forum Infect Dis 10:2086. doi:10.1093/ofid/ofad 500.2086 · doi ↗
- 6Antimicrobial Resistance. 2024. Canadian antimicrobial resistance surveillance system 2024. Available from: https://health-infobase.canada.ca/carss/amr/results.html?ind=09#further Reading. Retrieved 14 May 2025.
- 7Provincial Infection Control Network of British Columbia (PIC Net). 2019. Annual surveillance report of healthcare-associated infections in BC health care facilities: fiscal year 2018/2019.
- 8Provincial Infection Control Network of British Columbia (PIC Net). 2025. Quarterly surveillance reports. https://picnet.ca/surveillance/surveillance-reports/quarterly-reports.