Predictive Factors and Onset Timing of Delirium in Hospitalized Patients with Heart Failure
Noriko Kawazoe, Yoshiaki Kubota, Takuya Nishino, Miwako Ogane, Yoshiki Iwade, Daisuke Hayashi, Yukihiro Watanabe, Katsuhito Kato, Shuhei Tara, Kuniya Asai

TL;DR
This study identifies factors linked to early and late-onset delirium in heart failure patients, emphasizing the role of anticholinergic load and malnutrition.
Contribution
The study distinguishes predictive factors for early versus late-onset delirium in heart failure patients, highlighting anticholinergic load and malnutrition as key contributors.
Findings
Early-onset delirium is associated with higher anticholinergic load and C-reactive protein levels.
Late-onset delirium correlates with malnutrition and body mass index.
Hyperactive delirium is more common in early-onset cases, while hypoactive or mixed subtypes are prevalent in late-onset cases.
Abstract
This study aimed to examine the predictive factors and timing of delirium onset in hospitalized patients with heart failure, focusing on the impact of total anticholinergic load and other contributing variables. The single-site retrospective cohort study included 694 patients hospitalized for heart failure and receiving treatment for hyperpolypharmacy between January 2015 and March 2023. The patients were categorized into delirium and non-delirium groups, with the delirium group further subdivided into early-onset (within 6 days) and late-onset (day 7 or later) subgroups. Logistic regression analyses were performed to identify significant factors associated with delirium onset. Compared with the non-delirium group, the delirium group (n = 54) showed a higher total anticholinergic load, malnutrition prevalence, and elevated N-terminal pro-brain natriuretic peptide levels. Early-onset…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
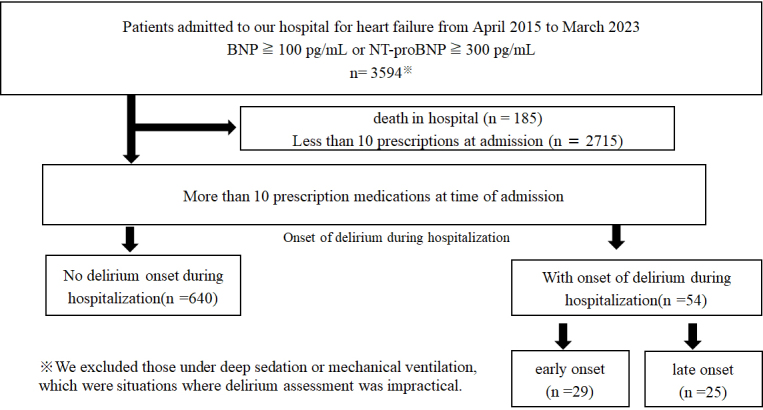 Figure 1
Figure 1| Variable | Non-delirium group | Delirium group | p Value | Early-onset | Late-onset | p Value |
|---|---|---|---|---|---|---|
| N | 640 | 54 | 29 | 25 | ||
| Age (years) | 78 (70-84) | 80 (69-85) | 0.234 | 83 (73-85) | 80 (68-85) | 0.761 |
| Men, n (%) | 416 (65.0) | 29 (53.7) | 0.130 | 14 (48.3) | 15 (60.0) | 0.557 |
| BMI ≥25 kg/m2, n (%) | 193 (31.1) | 20 (37.0) | 0.457 | 10 (34.5) | 10 (40.0) | 0.988 |
| LVEF (%) | 57 (39-66) | 54.50 (35-67) | 0.494 | 54 (35-64) | 58 (33-68) | 0.979 |
| Length of stay (days) | 14 (9-22) | 26 (16-40) | <0.001 | 18 (15-29) | 30 (21-60) | 0.008 |
| Alb (g/dL) | 3.7 (3.3-4.0) | 3.5 (3.0-3.8) | <0.001 | 3.7 (3.1-3.9) | 3.4 (2.9-3.6) | 0.106 |
| Alb <3.5 g/dL, n (%) | 202 (31.5) | 26 (48.1) | 0.023 | 13 (44.8) | 13 (52.0) | 0.607 |
| CRP (mg/dL) | 0.49 (0.16-2.02) | 0.88 (0.30-5.18) | 0.013 | 0.81 (0.29-5.38) | 0.96 (0.34-4.58) | 0.896 |
| Infection, n (%) | 130 (20.3) | 20 (37.0) | 0.017 | 11 (37.9) | 9 (36.0) | 0.886 |
| eGFR (mL/min/1.73 m2) | 46 (29-60) | 45 (23-59) | 0.365 | 46 (27-62) | 44 (23-52) | 0.278 |
| Hb (g/dL) | 12.2 (10.5-13.8) | 11.7 (10.8-13.2) | 0.384 | 11.7 (10.9-12.9) | 11.7 (10-13) | 0.487 |
| K (meq/L) | 4.2 (3.8-4.6) | 4.1 (3.9-4.6) | 0.853 | 4.1 (3.9-4.4) | 4.3 (3.9-4.6) | 0.244 |
| Na (meq/L) | 139 (137-142) | 138.50 (135-142) | 0.421 | 138 (136-143) | 139 (135-141) | 0.375 |
| NT-proBNP (pg/mL) | 2,256 (874-5,345) | 3,747 (2,388-8,437) | 0.002 | 3,435 (2,590-5,887) | 4,903 (1,959-8,849) | 0.249 |
| Number of medications | 11 (10-13) | 12 (11-13) | 0.245 | 12 (11-13) | 12 (10-13) | 0.698 |
| TAL | 1 (0-3) | 2 (1-6) | <0.001 | 4 (2-8) | 1 (0-2) | 0.001 |
| New-onset atrial arrhythmias, n (%) | 24 (3.8) | 3 (5.6) | 0.460 | 2 (6.9) | 1 (4.0) | 1.000 |
| Variable | Univariate analysis | Multivariate analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | CI_Lower | CI_Upper | p Value | OR | CI_Lower | CI_Upper | p Value | |
| Early-onset subgroup | ||||||||
| TAL | 1.254 | 1.159 | 1.360 | <0.001 | 1.255 | 1.160 | 1.363 | <0.001 |
| Age | 1.013 | 0.980 | 1.051 | 0.470 | ||||
| Men | 0.503 | 0.236 | 1.065 | 0.071 | ||||
| BMI ≥25 kg/m2 | 1.164 | 0.400 | 1.380 | 0.704 | ||||
| HFrEF | 1.813 | 0.813 | 3.874 | 0.131 | ||||
| NT-proBNP | 1.000 | 1.000 | 1.000 | 0.950 | ||||
| Alb | 0.577 | 0.294 | 1.141 | 0.111 | ||||
| CRP | 1.054 | 0.996 | 1.106 | 0.043 | 1.064 | 1.000 | 1.121 | 0.029 |
| Hb | 0.986 | 0.837 | 1.162 | 0.867 | ||||
| K | 0.755 | 0.416 | 1.290 | 0.335 | ||||
| Na | 0.999 | 0.919 | 1.094 | 0.989 | ||||
| eGFR | 0.999 | 0.983 | 1.014 | 0.875 | ||||
| ACE-I or ARB | 0.875 | 0.412 | 1.943 | 0.733 | ||||
| Beta blocker | 0.799 | 0.378 | 1.719 | 0.558 | ||||
| MRA | 1.503 | 0.676 | 3.201 | 0.299 | ||||
| SGLT2-i | 0.519 | 0.083 | 1.775 | 0.376 | ||||
| Loop diuretic | 1.285 | 0.564 | 2.759 | 0.531 | ||||
| Late-onset subgroup | ||||||||
| TAL | 0.946 | 0.772 | 1.100 | 0.531 | ||||
| Age | 1.012 | 0.976 | 1.054 | 0.531 | ||||
| Men | 0.808 | 0.361 | 1.885 | 0.608 | ||||
| BMI ≥25 kg/m2 | 1.475 | 0.417 | 1.931 | 0.352 | ||||
| HFrEF | 1.669 | 0.693 | 3.782 | 0.231 | ||||
| NT-proBNP | 1.000 | 1.000 | 1.000 | 0.583 | ||||
| Alb | 0.266 | 0.127 | 0.547 | <0.001 | 0.222 | 0.101 | 0.473 | <0.001 |
| CRP | 1.051 | 0.988 | 1.106 | 0.073 | ||||
| Hb | 0.928 | 0.779 | 1.104 | 0.398 | ||||
| K | 1.325 | 0.785 | 2.086 | 0.257 | ||||
| Na | 0.930 | 0.856 | 1.015 | 0.091 | ||||
| eGFR | 0.986 | 0.969 | 1.003 | 0.126 | ||||
| ACE-I or ARB | 0.494 | 0.219 | 1.106 | 0.084 | ||||
| Beta blocker | 1.380 | 0.604 | 3.427 | 0.460 | ||||
| MRA | 0.777 | 0.279 | 1.87 | 0.596 | ||||
| SGLT2-i | 0.955 | 0.222 | 2.835 | 0.941 | ||||
| Loop diuretic | 1.627 | 0.696 | 3.649 | 0.243 | ||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntensive Care Unit Cognitive Disorders · Electrolyte and hormonal disorders · Sepsis Diagnosis and Treatment
Introduction
Congestive heart failure (HF) is a cardiovascular disease with a high global prevalence and mortality rate, posing significant social and economic burdens in both developed and developing countries ^(1), (2)^. With the aging population and continuous advancements in healthcare, the number of patients with HF is expected to increase further, leading to a global decline in the quality of life ^(3)^.
Delirium, characterized by abrupt changes in attention, cognition, and awareness, is often triggered by underlying conditions such as HF that cannot be explained by pre-existing neurocognitive disorders ^(4)^. Moreover, HF has been identified as an independent risk factor for delirium ^(5)^. The presence of delirium in patients with HF complicates communication with healthcare providers, increasing the challenges faced by the medical staff ^(6)^. Multiple studies have demonstrated associations between delirium and adverse outcomes in patients with HF, including higher mortality rates, prolonged hospital stays, and increased healthcare costs ^(4), (7), (8), (9), (10), (11), (12)^. Additionally, patients with HF are often subject to polypharmacy ^(3)^, which can escalate into hyperpolypharmacy (HPP), a condition also reported in this population ^(13)^. Among various medications, the total anticholinergic load (TAL) has been identified as a significant risk factor for delirium ^(14)^. However, the diagnosis of delirium in patients with HF is often delayed, and current healthcare practices fail to adequately address the needs of these patients ^(4)^. Although delirium frequently occurs in older adults and patients with chronic illnesses, potential differences in the contributing factors based on the timing of delirium onset remain unclear. Additionally, the associated risks have not been fully elucidated. We hypothesized that risk factors differ across subgroups, depending on the timing of the onset of delirium. Therefore, this study examined the impact of TAL and other factors on the timing of delirium onset in patients with HF and HPP.
Materials and Methods
Design
This study followed a quantitative research design.
Population and sample
The inclusion criteria were urgent admission to our hospital for HF and treatment for HPP. Patients with urgent hospitalization included those requiring immediate HF management but excluded those under deep sedation or mechanical ventilation, which were situations where delirium assessment was impractical. HPP was defined as taking at least 10 medications at the time of admission. First, we categorized patients into two groups based on the presence or absence of delirium. The delirium group was further subdivided into two categories based on onset timing: an early-onset group (onset within 6 days of admission) and a late-onset group (onset on or after day 7 of admission). Supplementary Figure 1 presents a histogram of the delirium onset times. Early-onset delirium was defined as delirium with onset within a median of 6 days after admission. We analyzed differences in the patient backgrounds and examined factors influencing the occurrence and timing of delirium onset.
Delirium is defined in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) based on the following five key features ^(15)^:
-
Disturbance in attention and awareness.
-
Development over a short period, with fluctuations in severity throughout the day.
-
Additional disturbance in cognition.
-
These disturbances are not better explained by a pre-existing neurocognitive disorder.
-
There is evidence that the disturbance is a direct consequence of another medical condition.
Delirium was retrospectively diagnosed through a review of clinical records, including psychiatric consultations, or calculated for inpatient psychotherapy.
TAL was calculated based on the anticholinergic cognitive burden (ACB) scale developed by Boustani et al. ^(14)^. Each prescribed medication was assigned a score from 1 to 3 according to its anticholinergic potency, and the total ACB score was calculated as the sum of these individual scores. Supplementary Table 1 shows a detailed list of medications contributing to TAL. Malnutrition was defined according to a serum albumin level of <3.5 g/dL at the time of admission. New-onset atrial fibrillation was defined as atrial arrhythmias (including atrial fibrillation, atrial flutter, and atrial tachycardia) occurring prior to delirium onset.
Exclusion criteria
The exclusion criteria were in-hospital death and use of fewer than 10 drugs at admission.
Data sources
This single-site cohort study was based on information collected from the Diagnosis Procedure Combination (DPC) database of Nippon Medical School Hospital. The following data were extracted: patient age and sex, primary diagnoses and comorbidities, medications, and discharge status. The diagnoses followed the guidelines of the International Classification of Diseases, 10^th^ revision. Laboratory data and electrocardiograms were collected electronically from the medical records.
Data analysis
The primary endpoints of this study were the differences in the patient backgrounds, factors influencing the occurrence of delirium, and the timing of its onset.
Categorical variables were expressed as numbers and percentages and compared among the groups using the chi-squared test. Continuous variables were expressed as means and standard deviations or medians and interquartile ranges. Logistic regression analysis was performed to identify the factors associated with delirium occurrence. Variables included in multivariable logistic regression analysis were selected according to their clinical relevance and statistical significance in univariate analyses (p < 0.05). Two-sided p values <0.05 were considered to indicate statistical significance. The statistical analyses were performed using SPSS version 28 (IBM Corp., Armonk, NY, USA) and R software (version 4.2.1; R Foundation for Statistical Computing, Vienna, Austria).
Ethical considerations
The data were anonymized, and their use precluded the identification of individuals. Consequently, the requirement for patient consent was waived. The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Nippon Medical School Hospital (B-2021-433).
Results
Participants
Between April 2015 and March 2023, this study included 694 patients with HPP (taking ≥10 medications at the time of admission) who were hospitalized at our institution for HF (Figure 1). The mean age of the cohort was 76.0 ± 11.1 years, and 64.1% were men.
Flow chart showing the process of patient selection.Between April 2015 and March 2023, this study enrolled 694 patients with hyperpolypharmacy (taking 10 or more medications at admission) who were hospitalized at our institution for heart failure.
The participants were divided into the delirium (n = 54) and non-delirium (n = 640) groups. Compared with the non-delirium group, the delirium group exhibited a higher total anticholinergic burden, malnutrition, incidence of infections, and elevated levels of the N-terminal pro-brain natriuretic peptide (Table 1). The total number of medications did not differ significantly between the groups. Supplementary Table 2 shows the HF-related medication profiles across the four patient groups.
Comparison between the early-onset and late-onset delirium groups
The delirium group was further subdivided based on the timing of onset into the early-onset (within 6 days of admission, n = 29) and late-onset (7 days or later, n = 25) subgroups. There were no significant differences in age, sex, or presence of anemia between the subgroups. However, TAL was significantly higher in the early-onset subgroup, whereas the hospital stays were longer in the late-onset subgroup.
Logistic regression analysis was performed to identify factors associated with delirium onset in each subgroup. In the early-onset subgroup, both univariate and multivariate analyses identified high TAL scores and elevated C-reactive protein (CRP) levels as significant contributing factors. In the late-onset subgroup, both univariate and multivariate analyses identified malnutrition as a significant contributing factor (Table 2).
Subtypes of delirium
The prevalence of delirium subtypes in the early- and late-onset subgroups was determined through a chart review. Subtype classification was based on the DSM-5 criteria.
In the early-onset subgroup, the distribution was as follows: hyperactive subtype, 25/29 (86.2%) patients; mixed subtype, 3/29 (10.3%); and hypoactive subtype, 1/29 (3.5%). In the late-onset subgroup, the hypoactive and mixed subtypes were observed in 5/25 (20%) patients. Although the initial presentation in the late-onset subgroup was predominantly hyperactive delirium, 7/25 (28%) patients transitioned to the mixed subtype over time, with a tendency for prolonged recovery from delirium (Supplementary Table 3).
Discussion
This study identified high TAL, infection, and malnutrition as factors associated with delirium onset. Further analysis based on the timing of delirium onset revealed that early-onset delirium was directly influenced by an elevated TAL and infection, whereas late-onset delirium was primarily associated with malnutrition. These results underscore the need to adapt nursing care strategies according to the timing of hospitalization.
Specifically, for early-onset delirium, prehospital factors, such as TAL and the presence of infection, necessitate careful adjustment of medications to reduce the anticholinergic load and establishment of stringent measures to control medical conditions. In contrast, prevention of late-onset delirium requires targeted interventions, including rehabilitation and nutritional support, to address malnutrition.
Factors associated with early-onset delirium
High TAL and elevated CRP levels were identified as factors associated with early-onset delirium. These factors independently affected the onset of delirium, making it a particularly challenging condition. The fact that the occurrence was noted early, after hospital admission, suggests that approaches initiated after admission may not be sufficient to prevent onset. Collaboration with pharmacists to reduce TAL in daily practice may help prevent delirium. Additionally, assessing patients’ self-care capabilities, supporting behaviors that reduce infection risk, and coordinating social resources for patients with diminished functional abilities could contribute to prevention.
Recent studies have highlighted the detrimental effects of polypharmacy on patients with cardiovascular diseases. Kanai et al. ^(16)^ reported that HPP, particularly that involving non-cardiovascular medications, was associated with increased mortality and rehospitalization rates among older patients following acute decompensated HF (CURE-HF registry). Similarly, Yamamoto et al. ^(17)^ demonstrated that polypharmacy contributed to a higher risk of major bleeding after percutaneous coronary intervention, independent of antithrombotic therapy. Although polypharmacy itself is a known risk factor for adverse outcomes, our recent study reported that the focus should be on the quality, not the quantity, of drugs ^(18)^. These findings underscore the importance of optimizing medications in the management of patients vulnerable to delirium.
Factors associated with late-onset delirium
Low nutritional status was identified as factors associated with late-onset delirium. Although these are the predisposing factors for developing delirium, they are less likely to cause the condition independently. HF has been established as an independent risk factor for delirium ^(8), (19)^. Smith et al. reported that patients with delirium had longer hospital stays than did those without ^(19)^. Early identification of delirium risk is particularly important from a prognostic perspective ^(8)^. Patients presenting with the factors identified in this study should be classified as having a high risk for delirium, warranting systematic nursing care and multidisciplinary interventions involving dietitians, physical therapists, and other healthcare professionals. Delirium has been observed in both young and older patients and is associated with adverse outcomes within 30 days ^(20)^. These findings highlight the critical importance of evaluating and managing delirium in patients with acute HF regardless of age.
Strengths and limitations
The study was conducted on delirium that developed in patients with HF admitted to an advanced medical center after preventive measures were taken. This study has some limitations. First, the single-center DPC database design may have introduced a selection bias. Specifically, there was a possibility of immortal time bias, because patients discharged before the development of delirium could have been misclassified as non-delirious. Similarly, the exclusion of in-hospital deaths may have biased the results. Second, delirium was diagnosed by individual psychiatrists based on the DSM-5 criteria. Third, there is a lack of standardization in the methods for delirium assessment across studies, making it challenging to quantify potential relationships between delirium severity and outcomes in patients with HF. Several validated tools, including the Confusion Assessment Method, Memorial Delirium Assessment Scale, and Delirium Rating Scale R-98, exist to assess delirium severity ^(21), (22)^. However, the use of these tools was not explored in this study. Fourth, the study did not assess the most common causes of delirium, specifically, duration of bed rest, indwelling urinary catheterization, continuous intravenous infusion, fasting, and oxygenation. Fifth, there is no standardized assessment tool for delirium, and it is possible that delirium is underestimated for patients. Sixth, malnutrition was defined on the basis of serum albumin levels of <3.5 g/dL at admission. However, we acknowledge that albumin is influenced by inflammation and may not fully represent the nutritional status, and that no validated nutritional assessment tool was used.
Conclusions
This study identified high TAL and malnutrition as factors associated with delirium onset. In the early-onset group, specific triggers―a high TAL and infections―were identified as the primary risk factors, whereas malnutrition was associated with late-onset delirium. These findings highlight the importance of implementing preventive care strategies tailored to the timing of delirium onset. To enhance the generalizability and robustness of our results, future studies conducted across multiple centers with larger sample sizes and harmonized assessment protocols are recommended.
Article Information
Acknowledgments
The authors extend their sincere thanks to all the professionals involved in patient care, including the emergency staff, technicians, medical engineers, nurses, pharmacists, physicians, and surgeons at the Nippon Medical School Hospital. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author Contributions
NK conceived the study, and YK designed the study. NK and TN performed data collection, and TN conducted statistical analyses. MO, YI, DH, and YK drafted the original manuscript. All authors contributed to the final version of the manuscript for submission.
Conflicts of Interest
None
This study was conducted after obtaining permission from the Ethics Committee of the Nippon Medical School Hospital (B-2021-433).
Supplement
Supplementary Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alberto RM, Domingo R, Aitor A, et al. Long-term prognostic value of functional status and delirium in emergency patients with decompensated heart failure. Eur Geriatr Med. 2018;9(4):515-22.34674495 10.1007/s 41999-018-0072-0 · doi ↗ · pubmed ↗
- 2Ayatollahi Y, Liu X, Namazi A, et al. Early readmission risk identification for hospitalized older adults with decompensated heart failure. Res Gerontol Nurs. 2018;11(4):190-7.29634848 10.3928/19404921-20180322-01 · doi ↗ · pubmed ↗
- 3Battle DE. Diagnostic and Statistical Manual of Mental Disorders (DSM). Co DAS. 2013;25(2):191-2.24413388 10.1590/s 2317-17822013000200017 · doi ↗ · pubmed ↗
- 4Beezer J, Al Hatrushi M, Husband A, et al. Polypharmacy definition and prevalence in heart failure: a systematic review. Heart Fail Rev. 2022;27(2):465-92.34213753 10.1007/s 10741-021-10135-4PMC 8250543 · doi ↗ · pubmed ↗
- 5Correale M, Altamura M, Carnevale R, et al. Delirium in heart failure. Heart Fail Rev. 2020;25(5):713-23.31377979 10.1007/s 10741-019-09842-w · doi ↗ · pubmed ↗
- 6Han JH, Mc Naughton CD, Stubblefield WB, et al. Delirium and its association with short-term outcomes in younger and older patients with acute heart failure. PLOS One. 2022;17(7):e 0270889.35881580 10.1371/journal.pone.0270889 PMC 9321444 · doi ↗ · pubmed ↗
- 7Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. 2022;145(18):e 876-94.35363500 10.1161/CIR.0000000000001062 · doi ↗ · pubmed ↗
- 8Hutt E, Frederickson E, Ecord M, et al. Associations among processes and outcomes of care for Medicare nursing home residents with acute heart failure. J Am Med Dir Assoc. 2003;4(4):195-9.12837140 10.1097/01.JAM.0000073964.19754.C 0 · doi ↗ · pubmed ↗