Tuberculous Pleurisy Detected by Lung Ultrasound
Yuki Ohnishi, Yasuhiro Suyama, Kenichi Nakamura

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
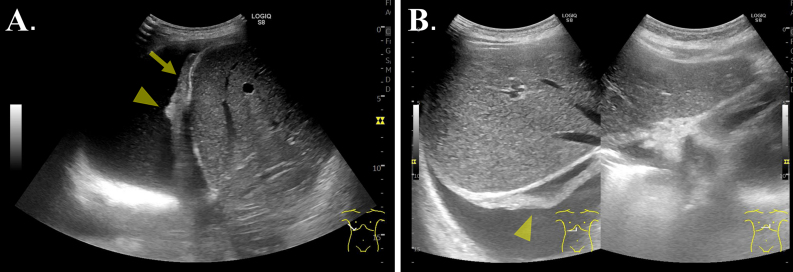 Figure 1
Figure 1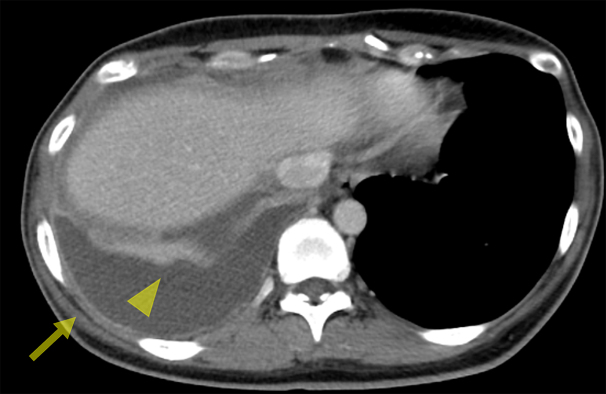 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUltrasound in Clinical Applications · Pleural and Pulmonary Diseases · Diagnosis and treatment of tuberculosis
A previously healthy 37-year-old Japanese woman presented with a 6-day history of right flank muscle cramps followed by 4 days of fever. She also reported dyspnea on exertion and occasional mild dry cough, both with unknown onsets. Physical examination was unremarkable, including absence of chest pain exacerbation with deep inspiration and no pleural friction rub appreciated. Lung ultrasound was performed (Figure 1A and 1B). Thoracentesis revealed an exudative pleural effusion with lymphocytic predominance and an adenosine deaminase level of 81 U/L. An enhanced chest computed tomography was obtained (Figure 2). T-SPOT was negative. She was admitted upon presentation. Sputum culture obtained on the day of admission confirmed Mycobacterium tuberculosis complex after 15 days of incubation. We diagnosed tuberculous pleurisy. The patient was referred to a tuberculosis treatment center for further management, where combination therapy with isoniazid, rifampin, ethambutol, and pyrazinamide led to resolution of symptoms. Later, she disclosed that her father, who died when she was 10 years old, had been treated for tuberculosis.
Tuberculous pleurisy is not always easy to diagnose and may occur in the absence of pulmonary lesions. Inflammation of the peripheral diaphragmatic pleura, innervated by lower intercostal nerves, can cause referred pain in the lower chest or upper abdomen ^(1)^. While a definitive diagnosis of tuberculous pleurisy relies on pleural biopsy tissue samples, biopsy cultures, and pleural effusion cultures ^(2)^, lung ultrasound provides an accessible and noninvasive modality to support the diagnosis. Pleural thickness of approximately 3 mm is a frequently observed ultrasonographic finding in pleural tuberculosis ^(3)^. In adult tuberculous pleurisy, subpleural nodules are among the lung ultrasound findings with the highest sensitivities, ranging from 72.5% to 100% ^(4)^. The evaluation of the pleura should be incorporated into the workup of lateral abdominal pain, and lung ultrasound is a potentially valuable diagnostic tool.
Article Information
Author Contributions
According to the definition provided by the International Committee of Medical Journal Editors, the following individuals meet the criteria for authorship based on their substantial contributions to the intellectual content of the manuscript: Yuki Ohnishi: conceptualization, investigation, writing - original draft; Yasuhiro Suyama: investigation, writing - review and editing; Kenichi Nakamura: writing - review and editing. All authors have read and approved the final manuscript.
Conflicts of Interest
None
Ethical Approval and Consent to Participate
The authors obtained consent from the patients for the publication of this report, including images.
Acknowledgment
The authors would like to express our gratitude to the support and feedback provided by Dr. Lance Bacon in the process of revising the manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Valdés L, Alvarez D, San José E, et al. Tuberculous pleurisy: a study of 254 patients. Arch Intern Med. 1998;158(18):2017-21.9778201 10.1001/archinte.158.18.2017 · doi ↗ · pubmed ↗
- 2Wang T, Du G, Fang L, et al. Value of ultrasonography in determining the nature of pleural effusion: analysis of 582 cases. Medicine (Baltimore). 2022;101(33):e 30119.35984158 10.1097/MD.0000000000030119 PMC 9388019 · doi ↗ · pubmed ↗
- 3Bigio J, Kohli M, Klinton JS, et al. Diagnostic accuracy of point-of-care ultrasound for pulmonary tuberculosis: a systematic review. P Lo S One. 2021;16(5):e 0251236.33961639 10.1371/journal.pone.0251236 PMC 8104425 · doi ↗ · pubmed ↗