Physician Characteristics Associated with Prioritizing Treatment Burden in Outpatient Care for Older Adults with Multimorbidity
Takuma Kimura, Ken Shinmura, Shinji Matsumura, Masayoshi Hashimoto

TL;DR
This study explores which physician traits are linked to prioritizing treatment burden in older patients with multiple health issues.
Contribution
The study introduces a new scale to assess treatment burden prioritization and identifies sex as a key factor influencing it.
Findings
A new six-item scale for assessing treatment burden prioritization showed good validity and consistency.
Female physicians were more likely to prioritize treatment burden compared to male physicians.
Years of experience and practice setting had no significant impact on prioritizing treatment burden.
Abstract
Older adults with multimorbidity often experience substantial treatment burden, which can compromise their quality of life and adherence to medical treatment. Accordingly, physicians need to prioritize treatment burden. However, physician characteristics associated with prioritization of treatment burden among older adults with multimorbidity in outpatient care remain unclear. This study aimed to: (1) develop a brief, clinician-oriented scale to assess prioritization of treatment burden in outpatient settings and evaluate its reliability and exploratory validity; and (2) examine associations between prioritizing treatment burden and physician attributes in Japan. We conducted an anonymous postal survey in June and July 2022 targeting 3,300 physicians affiliated with the Japan Geriatrics Society or the Japan Primary Care Association. Physicians’ prioritization of treatment burden was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
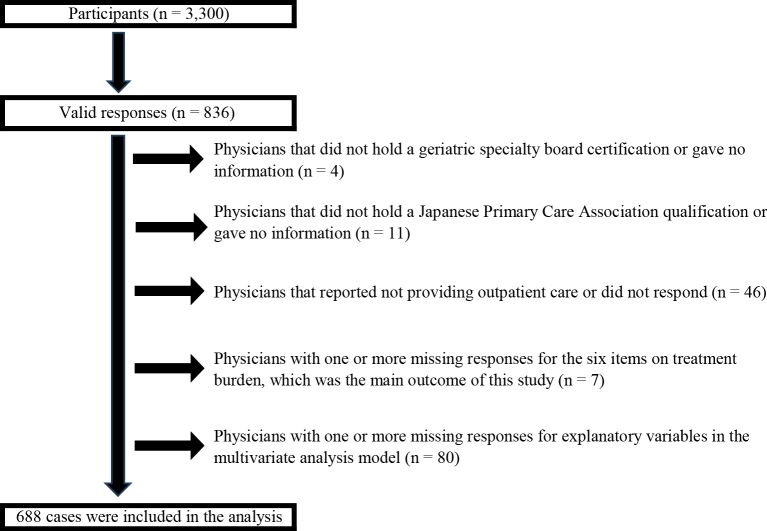 Figure 1
Figure 1| Component 1 | Component 2 | |
|---|---|---|
| Dietary therapy reduces QOL | 0.876 | 0.104 |
| Exercise therapy reduces QOL | 0.832 | 0.073 |
| Pharmacotherapy reduces QOL | 0.734 | 0.280 |
| Waiting time is burdensome | 0.126 | 0.860 |
| Visiting outpatient clinics is burdensome | 0.160 | 0.856 |
| Overall treatment burden exists | 0.460 | 0.394 |
| Not prioritized at all | Minimally prioritized | Moderately prioritized | Highly prioritized | |||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| Dietary therapy reduces QOL | 7 | 1.0% | 121 | 17.6% | 445 | 64.7% | 115 | 16.7% |
| Exercise therapy reduces QOL | 14 | 2.0% | 175 | 25.4% | 427 | 62.1% | 72 | 10.5% |
| Pharmacotherapy reduces QOL | 1 | 0.1% | 66 | 9.6% | 435 | 63.2% | 186 | 27.0% |
| Waiting time is burdensome | 6 | 0.9% | 146 | 21.2% | 452 | 65.7% | 84 | 12.2% |
| Visiting outpatient clinics is burdensome | 1 | 0.1% | 45 | 6.5% | 465 | 67.6% | 177 | 25.7% |
| Overall treatment burden exists | 2 | 0.3% | 22 | 3.2% | 341 | 49.6% | 323 | 46.9% |
| Total | High prioritization group | Low prioritization group | p-Value | ||||
|---|---|---|---|---|---|---|---|
| n or mean | % or SD | n or mean | % or SD | n or mean | % or SD | ||
| Sex | 0.002 | ||||||
| Male | 564 | 82.0% | 392 | 79.2% | 172 | 89.1% | |
| Female | 124 | 18.0% | 103 | 20.8% | 21 | 10.9% | |
| Age (years) | 53.4 | 11.9 | 53.3 | 11.9 | 53.4 | 11.9 | 0.908 |
| Experience as a physician (years) | 27.7 | 11.6 | 27.7 | 11.5 | 27.7 | 11.7 | 0.929 |
| Type of facility | 0.755 | ||||||
| Clinic | 220 | 32.0% | 160 | 32.3% | 60 | 31.1% | |
| Hospital | 468 | 68.0% | 335 | 67.7% | 133 | 68.9% | |
| Type of facility | 0.935 | ||||||
| Non-bedded clinic | 199 | 28.9% | 53 | 27.5% | 146 | 29.5% | |
| Bedded clinic | 21 | 3.1% | 7 | 3.6% | 14 | 7.0% | |
| Hospital with <200 beds | 170 | 24.7% | 46 | 23.8% | 124 | 25.1% | |
| Hospital with ≥200 beds | 212 | 30.8% | 61 | 31.6% | 151 | 30.5% | |
| University hospital | 86 | 12.5% | 26 | 13.5% | 60 | 12.1% | |
| Clinical setting | |||||||
| Ward | 0.386 | ||||||
| Provided | 374 | 54.4% | 264 | 53.3% | 110 | 57.0% | |
| Not provided | 314 | 45.6% | 231 | 46.7% | 83 | 43.0% | |
| Home medical care | 0.269 | ||||||
| Provided | 265 | 38.5% | 197 | 39.8% | 68 | 35.2% | |
| Not provided | 423 | 51.5% | 298 | 60.2% | 125 | 64.8% | |
| Long-term care facility | 0.144 | ||||||
| Provided | 184 | 26.7% | 140 | 28.3% | 44 | 22.8% | |
| Not provided | 504 | 73.3% | 355 | 71.7% | 149 | 77.2% | |
| Municipality population size | 0.628 | ||||||
| Under 100,000 | 187 | 27.2% | 132 | 26.7% | 55 | 28.5% | |
| Over 100,000 | 501 | 72.8% | 363 | 73.3% | 138 | 71.5% | |
| Frequency of treating patients aged 65-75 years | 0.484 | ||||||
| Low | 2 | 0.3% | 1 | 0.2% | 1 | 0.5% | |
| High | 684 | 99.7% | 492 | 99.8% | 192 | 99.5% | |
| Frequency of treating patients aged 75-89 years | 0.192 | ||||||
| Low | 3 | 0.4% | 1 | 0.2% | 2 | 1.0% | |
| High | 684 | 99.6% | 493 | 99.8% | 191 | 99.0% | |
| Frequency of treating patients aged ≥90 years | 0.324 | ||||||
| Low | 37 | 5.4% | 24 | 4.8% | 13 | 6.7% | |
| High | 651 | 94.6% | 471 | 95.2% | 180 | 93.3% | |
| Model 1 | Model 2 | |||||||
|---|---|---|---|---|---|---|---|---|
| Prevalence ratio | 95% confidence interval | p-Value | Prevalence ratio | 95% confidence interval | p-Value | |||
| Lower | Higher | Lower | Higher | |||||
| Experience as a physician (years) | 1.002 | 0.997 | 1.006 | 0.461 | 1.002 | 0.997 | 1.006 | 0.461 |
| Sex | ||||||||
| Female | 1.204 | 1.084 | 1.336 | <0.001 | 1.202 | 1.082 | 1.335 | <0.001 |
| Male | REF | REF | - | - | ||||
| Municipality population size | ||||||||
| Under 100,000 | 0.987 | 0.887 | 1.098 | 0.808 | 0.978 | 0.878 | 1.089 | 0.679 |
| Over 100,000 | REF | - | - | REF | - | - | ||
| Frequency of treating patients aged ≥90 years | ||||||||
| High | 1.111 | 0.866 | 1.425 | 0.408 | 1.094 | 0.852 | 1.404 | 0.481 |
| Low | REF | - | - | REF | - | - | ||
| Type of facility | ||||||||
| Clinic | 1.011 | 0.916 | 1.116 | 0.828 | - | - | - | |
| Hospital | REF | - | - | - | - | - | ||
| Clinical setting | ||||||||
| Ward | ||||||||
| Provided | - | - | - | 0.969 | 0.880 | 1.066 | 0.518 | |
| Not provided | - | - | - | REF | - | - | ||
| Home medical care | ||||||||
| Provided | - | - | - | 1.019 | 0.906 | 1.146 | 0.754 | |
| Not provided | - | - | - | REF | - | - | ||
| Long-term care facility | ||||||||
| Provided | - | - | - | 1.067 | 0.947 | 1.201 | 0.286 | |
| Not provided | - | - | - | REF | - | - | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Disease Management Strategies · Primary Care and Health Outcomes · Healthcare Policy and Management
Introduction
Japan is the most rapidly aging country in the world, and the proportion of older adults with multimorbidity is expected to increase. In such patients, the cumulative demands of medication management, clinic visits, self-care, and lifestyle modifications constitute a substantial treatment burden, which can lead to poor medical treatment adherence, treatment discontinuation, and ultimately impaired disease control and adverse health outcomes ^(1), (2), (3)^. Older adults are particularly vulnerable to treatment burden because of cognitive decline, impaired activities of daily living, and limited social support, which may compromise both their quality of life (QOL) and the quality of care they receive ^(4), (5), (6), (7)^.
Japan’s healthcare system is characterized by a strong reliance on outpatient services, and has one of the highest rates of outpatient visits among Organisation for Economic Co-operation and Development (OECD) countries ^(8)^. Consequently, clinic visits often become a significant component of treatment burden ^(3)^. The highly specialized nature of Japanese healthcare also means many older adults with multimorbidity must attend multiple departments, which further compounds treatment burden. Therefore, outpatient care for older adults with multimorbidity in Japan is structurally prone to generating treatment burden.
Previous studies showed that physicians tended to underestimate patients’ treatment burden, leading to a mismatch between physicians’ perceptions and patients’ subjective experiences of daily challenges, medication management, and clinic visits ^(9), (10)^. This gap may contribute to reduced treatment adherence and fragmented care. Treatment burden should be evaluated from the patient’s perspective, but cognitive decline may make self-assessment difficult among older adults ^(5), (7)^. Therefore, in addition to caregiver input, physicians require a framework that enables them to recognize and actively respond to treatment burden in clinical practice, particularly in time-constrained outpatient settings. However, no simple scale currently exists for physicians to directly assess treatment burden. We hypothesized that physicians may find it more intuitive to understand treatment burden when framed in terms of QOL decrements caused by treatment itself.
In Western countries, general practitioners and geriatricians are increasingly recognized as playing central roles in alleviating treatment burden in outpatient care for older adults with multimorbidity ^(11), (12), (13)^. A similar role is expected in Japan. However, little is known about the extent to which physicians in Japan prioritize treatment burden, or how this prioritization relates to physician attributes such as sex, years of clinical experience, and practice setting. Identifying these characteristics may be crucial for designing educational programs and policy interventions to improve the quality of care for older adults with multimorbidity.
This study had two aims. First, we developed a brief, clinician-oriented scale to enable physicians to conceptualize treatment burden in relation to QOL and evaluated its reliability and exploratory validity. Second, we examined how physicians providing outpatient care in Japan perceived treatment burden in older adults with multimorbidity and explored associations between prioritization of treatment burden and physician attributes, including sex, clinical experience, and practice environment.
Materials and Methods
Study population
We conducted an anonymous, mail-based questionnaire survey in June and July 2022. To specifically target physicians who are extensively involved in the outpatient care of older adults with multimorbidity, we included all 1,650 certified geriatricians registered with the Japan Geriatrics Society as of April 2022. In addition, to capture physicians providing outpatient care for older adults with multimorbidity in community settings who were not organ- or disease-specific specialists, we randomly selected 1,650 physicians from among the 6,526 eligible members of the Japan Primary Care Association (JPCA). Eligible JPCA members comprised 1,091 board-certified family medicine specialists and 5,435 board-certified primary care physicians. In total, 3,300 physicians were included in our study sample.
Questionnaire
The questionnaire comprised 15 items, including the primary outcome measure (i.e., prioritization of treatment burden in the outpatient care of older adults with multimorbidity), participant characteristics, and items used for other research purposes ^(14), (15)^.
Analytical model
Our literature review revealed no prior studies examining the relationship between physician attributes and their awareness of treatment burden. Based on previous literature, we hypothesized that attributes associated with higher prioritization of treatment burden would be: (1) more years of experience, (2) female sex (women were previously shown to be more patient-centered), (3) practicing in smaller municipalities, (4) frequently caring for patients aged ≥90 years, and (5) working in clinics, home visit settings, or long-term care facilities ^(4), (5), (6), (7), (9), (16), (17), (18)^. We restricted our analysis to physicians engaged in outpatient practice because outpatient care is a key setting for managing older adults with multimorbidity and delivering care in resource- and time-constrained environments.
Questions on prioritization of treatment burden
We developed a six-item scale to assess the extent to which physicians prioritized treatment burden based on prior patient-reported burden scales ^(19), (20), (21)^ and internal discussions. We reframed the concept of treatment burden using QOL as a lens to enhance physician understanding and included both disease management and logistical aspects of care. The final items were: “Dietary therapy reduces QOL,” “Exercise therapy reduces QOL,” “Pharmacotherapy reduces QOL,” “Waiting time is burdensome,” “Visiting outpatient clinics is burdensome,” and “Overall treatment burden exists.” Each item was scored on a 4-point Likert scale from 1 (not prioritized at all) to 4 (highly prioritized).
The reliability and validity of the scale was evaluated. We assessed construct validity by calculating Pearson’s correlation coefficients for convergent validity between our scale and two theoretically relevant items: “Assessing patient burden” and “Revising treatment plans.” To evaluate the discriminant validity, we used two items expected to be weakly correlated with treatment burden prioritization: “difficulty addressing social issues” and “difficulty treating patients with severe comorbidities.”
We conducted exploratory factor analysis (EFA) to examine latent factor structures. Principal component analysis was used for extraction and varimax rotation and Kaiser normalization was applied. Factor retention was based on eigenvalues >1.0 (Kaiser criterion) and visual inspection of the scree plot. Cronbach’s alpha was calculated to assess internal consistency.
Physician characteristics
Participants were asked to report their sex, age, and clinical experience (years and months). Practice setting was recorded as clinic without beds, clinic with beds, hospital with <200 beds, hospital with ≥200 beds, tertiary care hospital, or long-term care/older adult care facility. Participants also reported their practice type (outpatient, home visits, long-term care, inpatient) and municipality population size (<50,000, 50,000-100,000, 100,000-300,000, 300,000-500,000, >500,000). Frequency of care by patient age group (65-74 years, 75-89 years, ≥90 years) was assessed using four categories: “never,” “rarely,” “sometimes,” and “frequently.”
Data analysis
Treatment burden prioritization
Items were scored from 1 to 4 points, and these scores were summed to calculate a total score from 6 to 24. Higher scores reflected greater prioritization of treatment burden. Participants were classified into two groups based on the median score: those scoring above the median were assigned to the “high prioritization” group; those scoring below the median to the “low prioritization” group.
Background characteristics
Municipality size was dichotomized as <100,000 (non-urban) and ≥100,000 (urban) based on previous studies. Frequency of treating patients in each age group was categorized as “low” (never or rarely) or “high” (sometimes or frequently). We compared participants’ background characteristics across prioritization groups using chi-square tests, Fisher’s exact tests, or Mann-Whitney U-tests, as appropriate.
Factors associated with prioritization
We used modified Poisson regression to calculate prevalence ratios (PRs) and 95% confidence intervals (CIs), with high prioritization ^(1)^ versus low prioritization (0) as the outcome ^(22)^. Covariates included years of experience (continuous), sex (male/female), municipality population size (<100,000/≥100,000), and frequency of caring for patients aged ≥90 years (high/low). Model 1 included these covariates plus facility type (clinic/hospital). Model 2 further included inpatient care, home visits, and facility-based care. We assessed multicollinearity using variance inflation factors (VIFs) with a threshold of <10. All analyses were two-tailed, with the significance level set at p < 0.05. Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 29.0.1 (IBM Corp., Armonk, NY, USA).
Ethical approval
This study was approved by the Ethics Committee of the Maruki Memorial Medical and Social Welfare Center (Approval Number 37). Consent was obtained through the voluntary return of completed questionnaires, which included a cover sheet describing the study’s aims, data protection procedures, and researcher contact information.
Results
In total, 836 responses were received (response rate 25.3%). Of these, 15 physicians were excluded: four from the geriatrics group who were not certified geriatricians and 11 from the primary care group who had neither family medicine nor primary care certification. An additional 46 physicians were excluded because they did not provide outpatient care, and seven were excluded because of incomplete responses on any of the six primary outcome items. Finally, 80 physicians were excluded because of missing data on explanatory variables. The final analytic sample comprised 688 physicians (Figure 1).
Population flow diagram of study participants.
Participants’ mean age was 53.41 ± 11.89 years, and their mean clinical experience was 27.68 ± 11.63 years. The majority (n = 564, 82.0%) of participants were male and 124 (18.0%) were female.
- Reliability and Validity of the Treatment Burden Prioritization Scale
Evaluation of convergent validity showed the Treatment Burden Prioritization Scale score was moderately correlated with “assessing patient burden” (r = 0.455) and “revising treatment plans” (r = 0.396), which was consistent with theoretical assumptions. Evaluation of discriminant validity showed that correlations with “difficulty addressing social issues” (r = 0.061) and “difficulty treating patients with severe comorbidities” (r = 0.029) were low, as expected. These results supported the convergent and discriminant validity of our scale.
EFA of the Treatment Burden Prioritization Scale indicated a two-factor structure based on eigenvalues and scree plot examination (Table 1). Items related to diet, exercise, and medication loaded on Factor 1 (“QOL impact”), and waiting time and transportation burden loaded on Factor 2 (“Outpatient visit burden”). The item “There is treatment burden” showed high cross-loading on both factors, suggesting a general factor nature. The Kaiser-Meyer-Olkin measure was 0.735 and Bartlett’s test of sphericity was significant (p < 0.001), indicating the scale had adequate factorability. The Cronbach’s alpha was 0.790 for Factor 1 (three items), 0.728 for Factor 2 (two items), 0.757 for five items combined, and 0.771 for all six items.
These results indicated the scale was a valid tool for assessing physician prioritization of treatment burden in the care of older adults with multimorbidity, with a clear conceptual structure and theoretical consistency.
- Treatment Burden in the Management of Older Adults with Multimorbidity (Table 2)
Overall “moderately prioritized” was the most common response for all six items. On an item level, the most common response for “Pharmacotherapy reduces QOL,” “Visiting outpatient clinics is burdensome,” and “Overall treatment burden exists” was “highly prioritized” followed by “moderately prioritized.” For “Dietary therapy reduces QOL,” “Exercise therapy reduces QOL,” and “Waiting time is burdensome,” the most common response was “minimally prioritized” followed by “moderately prioritized.” The overall mean score for the prioritization scale was 18.47 ± 2.43 (out of 24). The median score was 19, and 193 physicians (28.1%) were classified as the low prioritization group and 495 (71.9%) as the high prioritization group.
- Basic Characteristics and Treatment Burden Prioritization (Table 3)
Female physicians were significantly more likely to be in the high prioritization group than male physicians (p < 0.001). No significant differences were observed between treatment burden prioritization and age or years of clinical experience. There were no statistically significant differences between prioritization groups for types of clinical service (e.g., home visits, long-term care facility care, inpatient care), municipality population size, or frequency of treating patients by age group (65-74 years, 75-89 years, ≥90 years).
- Factors Associated with the Prioritization of Treatment Burden in Outpatient Care for Older Patients (Table 4)
In both model 1 (PR 1.204, 95% CI: 1.084-1.336) and model 2 (PR 1.202, 95% CI: 1.082-1.335), being female was significantly associated with higher prioritization of treatment burden compared with being male. Kendall correlation coefficients among independent variables showed no multicollinearity (τ < 0.70, maximum was 0.207 in model 1 and 0.393 in model 2). The VIFs were ≤1.078 in model 1 and ≤1.499 in model 2.
Discussion
This study focused on physicians’ prioritization of treatment burden in the provision of outpatient care of older adults with multimorbidity. First, we demonstrated that the newly developed six-item scale for assessing treatment burden prioritization showed reliability and exploratory validity. We then clarified the associations between prioritization of treatment burden and physician characteristics and practice environments in the context of outpatient care. To our knowledge, few previous studies evaluated physicians’ attitudes toward treatment burden from this perspective, meaning our study is a pioneering attempt in this field.
The six-item scale developed in this study was structured around two conceptual domains: “impact of treatment on QOL” and “burden of outpatient visits.” This framework allowed for a brief, practical assessment across multiple domains, including treatment modalities, lifestyle modifications, and access to care. Previous research showed that discrepancies often exist between patients’ self-perceived treatment burden and physicians’ understanding thereof, with physicians tending to focus predominantly on medical factors ^(9), (10), (23)^. Our scale may help bridge this perceptual gap in geriatric and primary care settings when used alongside existing patient-reported measures, thereby serving as a useful tool for shared decision-making, including treatment adjustment and deprescribing ^(24)^. From a practical perspective, our scale can be readily integrated into outpatient workflows because it can be quickly completed by physicians before or after patient encounters. Scores above a certain threshold may serve as a cue to reconsider treatment strategies, but the scale may be particularly useful when scores fall below a set threshold. As all patients with multimorbidity experience some degree of treatment burden, low scores could function as a reminder for physicians to heighten their awareness of this issue ^(1), (3), (4)^. For example, based on the scale items, such reminders may prompt physicians to reconsider specific clinical actions, including deprescribing, modifying lifestyle recommendations, or adjusting follow-up intervals. Furthermore, when discrepancies arise between physicians’ scores and patient-reported measures, comparison of these results may stimulate dialogue, uncover hidden patient concerns, and ultimately contribute to more individualized and patient-centered care.
A key finding of this study was that sex was significantly associated with physicians’ prioritization of treatment burden. Female physicians were more likely to prioritize treatment burden than male physicians. This suggested that female physicians may be more sensitive to the impact of treatment on patients’ daily lives and the logistical burdens of outpatient visits. This result was consistent with previous studies that reported female physicians were more likely to adopt patient-centered approaches than male physicians ^(16), (17), (18)^. Female physicians are also known to engage in empathetic communication, employ holistic perspectives, spend more time per consultation, and devote attention to psychosocial contexts ^(17), (18)^. These factors may contribute to their heightened awareness of treatment burden. The sex difference observed in this study may reflect social and cultural gender roles in addition to biological sex differences ^(17), (25)^.
In contrast, clinical experience, engagement in home or facility-based care, and frequency of caring for different age groups of older adults were not significantly associated with prioritization of treatment burden. Several interpretations for these findings are possible. First, extensive clinical experience does not necessarily translate into a deeper recognition of treatment burden. Without structured education or opportunities for continuing learning, it may be difficult for physicians to acquire awareness of treatment burden through experience alone. Second, even when physicians regularly care for the oldest old or practice in long-term care settings, a predominant focus on medical management may limit recognition of patients’ subjective burdens and psychosocial needs. Previous studies suggested that clinics may provide higher-quality care for older adults with multimorbidity compared with hospitals ^(26)^. However, our study found no significant association between practice setting and prioritization of treatment burden. This suggested physicians’ individual attitudes and values may play a greater role than practice environment in shaping their recognition of treatment burden. Educational interventions therefore hold potential to effect meaningful change. Although recent educational initiatives in Japan have begun to address outpatient care for patients with multimorbidity, training specifically focused on treatment burden remains lacking ^(27)^. Developing educational programs that explicitly integrate treatment burden into outpatient care for older adults is essential.
This study had several limitations. First, although the scale we developed demonstrated construct validity and internal consistency, its content validity remains exploratory. Further research should assess our scale’s agreement with patients’ self-reported treatment burden, compare it with existing patient-reported measures, and examine concordance or discordance with caregiver-reported burden, particularly among older patients with cognitive impairment. Reproducibility across multiple sites should also be evaluated ^(24)^. Second, this study targeted geriatricians and certified physicians from the JPCA, who represent physicians providing outpatient care for older adults with multimorbidity but not organ- or disease-specific specialists. Although this sampling strategy provided a degree of representativeness, participation was voluntary, which raises the possibility of selection bias if physicians with stronger interest in treatment burden were most likely to respond. Third, the survey relied on self-reported data, which may not fully reflect actual clinical behaviors. Fourth, physician sex was analyzed as a binary variable (male/female). The observed sex differences may partly reflect broader gender roles. Further studies should examine how sex and gender perspectives influence recognition and management of treatment burden in greater detail ^(17), (28)^.
The complexity of multiple coexisting conditions renders additive treatment approaches based solely on single-disease guidelines insufficient for older adults with multimorbidity ^(12), (13)^. Because additive approaches may exacerbate treatment burden, clinicians must not only decide “what to treat,” but also determine “which treatments burden patients most,” prioritize accordingly, and consider discontinuing therapies when appropriate. Raising physicians’ awareness of treatment burden is clinically and policy-relevant. Alleviating treatment burden may improve patients’ QOL and treatment adherence, and reduce avoidable hospitalizations and healthcare costs. Therefore, widespread use of the six-item Treatment Burden Prioritization Scale in daily practice could foster more patient-centered multimorbidity care in Japan.
Our findings suggest that physicians’ sex has a greater influence on attitudes toward treatment burden than clinical experience or practice environment. This implies that awareness of treatment burden may not be naturally acquired through experience alone. Rather, structured educational interventions are needed to enhance physicians’ recognition of treatment burden. Developing training programs focused on treatment burden―including its assessment, shared decision-making, and deprescribing―may improve the quality of care for older adults with multimorbidity. Incorporating such modules into residency training, continuing professional development, and board certification for geriatric and primary care specialists could help shift physician attitudes and contribute to overall improvement in care quality.
Article Information
Acknowledgments
We express our deep appreciation to Dr. Masahiro Akishita, former President of the JGS, geriatric specialists; Dr. Tetsushu Kusaba, President of the JPCA, family medicine specialists; and primary care certified physicians for their cooperation with this survey.
Author Contributions
Takuma Kimura and Ken Shinmura conceived the research questions. Takuma Kimura and Ken Shinmura contributed to the design of the research protocol and the development of the questionnaire. Takuma Kimura and Shinji Matsumura conducted the statistical analysis. Takuma Kimura drafted the initial manuscript in collaboration with Ken Shinmura, Shinji Matsumura, and Masayoshi Hashimoto. All authors revised and approved the final manuscript.
Conflicts of Interest
First author reports receiving research grants from CUC (Change Until Change) Inc. and Kyouseikai Medical Corporation, Japan. The other authors declare that there are no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mair FS, May CR. Thinking about the burden of treatment. BMJ. 2014;349:g 6680.25385748 10.1136/bmj.g 6680 · doi ↗ · pubmed ↗
- 2Eton DT, Ridgeway JL, Egginton JS, et al. Finalizing a measurement framework for the burden of treatment in complex patients with chronic conditions. Patient Relat Outcome Meas. 2015;6:117-26.25848328 10.2147/PROM.S 78955 PMC 4383147 · doi ↗ · pubmed ↗
- 3Lee JE, Lee J, Shin R, et al. Treatment burden in multimorbidity: an integrative review. BMC Prim Care. 2024;25(1):352.39342121 10.1186/s 12875-024-02586-z PMC 11438421 · doi ↗ · pubmed ↗
- 4Morris JE, Roderick PJ, Harris S, et al. Treatment burden for patients with multimorbidity: cross-sectional study with exploration of a single-item measure. Br J Gen Pract. 2021;71(706):e 381-90.33875419 10.3399/BJGP.2020.0883 PMC 8074644 · doi ↗ · pubmed ↗
- 5Zhang J, Xu X, Zhang X, et al. Self-perceived care needs and quality of life in people with cognitive impairment during routine care at home: cross-sectional results of the interventional study. BMC Geriatr. 2023;23(1):185.36991348 10.1186/s 12877-023-03846-w PMC 10061730 · doi ↗ · pubmed ↗
- 6Gebreyohannes EA, Gebresillassie BM, Mulugeta F, et al. Treatment burden and health-related quality of life of patients with multimorbidity: a cross-sectional study. Qual Life Res. 2023;32(11):3269-77.37405663 10.1007/s 11136-023-03473-3PMC 10522511 · doi ↗ · pubmed ↗
- 7Sheehan OC, Leff B, Ritchie CS, et al. A systematic literature review of the assessment of treatment burden experienced by patients and their caregivers. BMC Geriatr. 2019;19(1):262.31604424 10.1186/s 12877-019-1222-z PMC 6788093 · doi ↗ · pubmed ↗
- 8OECD. 2025, July. OECD health statistics 2025. Definitions, sources and methods. Healthcare utilisation – 1_Consultations: 1_1 Total doctors consultations (including teleconsultations). OECD Publishing. https://stats.oecd.org/wbos/fileview 2.aspx?ID File=839106 ea-625f-4ff 4-87a 8-1201 a 8647 af 5 [accessed 11 September 2025].