Ruptured Hepatic Artery Aneurysms Revealing Systemic Lupus Erythematosus
Saori Inoue, Mari Tatsumi, Yu Tanaka, Aya Ide

TL;DR
A rare case of ruptured hepatic artery aneurysms revealed systemic lupus erythematosus, highlighting the importance of timely diagnosis and treatment.
Contribution
This case report adds a unique presentation of SLE revealed by ruptured hepatic artery aneurysms and emphasizes the role of immunosuppressive therapy in vasculitis.
Findings
Ruptured hepatic artery aneurysms revealed SLE with antiphospholipid antibody syndrome in a 74-year-old woman.
Endovascular embolization and immunosuppressive therapy led to rapid aneurysm regression and improved outcomes.
The case supports an inflammatory vasculitic mechanism in SLE-associated hepatic artery aneurysms.
Abstract
Hepatic artery aneurysms are rare vascular lesions, most often caused by infection, but occasionally linked to connective tissue diseases such as systemic lupus erythematosus (SLE). We report a case of multiple hepatic artery aneurysms revealing SLE with antiphospholipid antibody syndrome. A 74-year-old woman, having previously undergone splenectomy for pancytopenia of unknown cause, was admitted for postoperative maxillary cyst infection. On day 10, she developed acute abdominal pain; computed tomography showed multiple hepatic artery aneurysms with rupture. Emergency transcatheter arterial embolization of the A5 branch achieved hemostasis. Serology was positive for antinuclear antibody, anti-double-stranded DNA antibody, lupus anticoagulant, and anti-β2-glycoprotein I antibody. She had pericardial effusion, hypocomplementemia, proteinuria, hemolytic anemia, and erythema, leading to a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
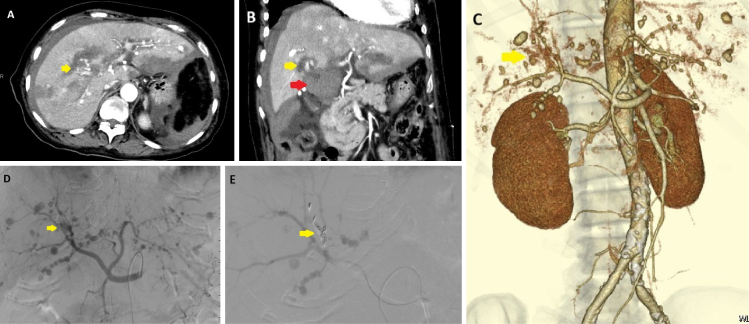 Figure 1
Figure 1| Parameter | Reference range | After rupture (Day 10) | 6 months follow-up |
|---|---|---|---|
| White blood cell count (/μL) | 3,300-8,600 | 10,520 | 6,510 |
| Hemoglobin (g/dL) | 11.6-14.8 | 8.0 | 10.0 |
| Platelet count (/μL) | 158,000-348,000 | 292,000 | 398,000 |
| Lactate dehydrogenase (U/L) | 124-222 | 151 | 195 |
| Haptoglobin (mg/dL) | 20-200 | <1 | 127 |
| Direct Coombs test | Negative | Positive | NA |
| Serum creatinine (mg/dL) | 0.6-1.1 | 0.75 | 0.45 |
| Estimated glomerular filtration rate (mL/min/1.73 m2) | >60 | 57.1 | 99.5 |
| Proteinuria (g/g creatinine) | <0.15 | 0.79 | 0.31 |
| Aspartate aminotransferase (U/L) | 13-30 | 46 | 11 |
| Alanine aminotransferase (U/L) | 7-23 | 26 | 4 |
| Alkaline phosphatase (U/L) | 38-113 | 122 | 62 |
| Gamma-glutamyl transpeptidase (U/L) | 9-32 | 82 | 29 |
| Total bilirubin (mg/dL) | 0.4-1.5 | 0.34 | 0.32 |
| Complement component 3 (mg/dL) | 86-160 | 67 | 126 |
| Complement component 4 (mg/dL) | 17-45 | 10 | 17 |
| Total hemolytic complement activity (CH50/mL) | 25-48 | 13.1 | 22.9 |
| Anti-double-stranded DNA antibody | Negative | Positive | Negative |
| Lupus anticoagulant | Negative | Positive | NA |
| Anti-cardiolipin β2 glycoprotein I antibody | Negative | Positive | NA |
| Proteinase 3-anti-neutrophil cytoplasmic antibody (U/mL) | <3.4 | <1 | NA |
| Myeloperoxidase-anti-neutrophil cytoplasmic antibody (U/mL) | <3.5 | <1 | NA |
| Antinuclear antibody, Homogeneous pattern (titer) | <1:40 | 80 | NA |
| Antinuclear antibody, Speckled pattern (titer) | <1:40 | 80 | NA |
| Antinuclear antibody, Nucleolar pattern (titer) | <1:40 | 80 | NA |
| C-reactive protein (mg/dL) | <0.14 | 5.01 | 1.48 |
| Author & Year | Age / Sex | Chief Complaint / Presentation | Aneurysm Location | Treatment Method | Outcome | Reference |
|---|---|---|---|---|---|---|
| C Liu, 2011 | 31-year-old male | Epigastric pain and jaundice for 2 months | Two hepatic artery aneurysms in the left lateral lobe | TAE, later left lateral lobectomy and ligation of the proximal hepatic artery | Good recovery | 7 |
| EN Pollono, 2009 | 56-year-old female | Gastrointestinal bleeding without identifiable lesions | Multiple hepatic artery aneurysms | TAE | Good recovery | 4 |
| J Trambert, 1989 | 49-year-old male | Caused by ruptured aneurysms of a branch of the left hepatic artery | Branch of the left hepatic artery | TAE | Good recovery | 8 |
| Present case, 2022 | 74-year-old female | Abdominal pain, intraperitoneal bleeding | Multiple intrahepatic aneurysms | TAE | Good recovery |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal vascular conditions and treatments · Liver Diseases and Immunity · IgG4-Related and Inflammatory Diseases
Introduction
Hepatic artery aneurysms are most commonly caused by infection but are occasionally associated with connective tissue diseases such as systemic lupus erythematosus (SLE) ^(1), (2)^. We report a case of multiple hepatic artery aneurysms that led to the diagnosis of SLE, accompanied by a literature review.
Case Report
A 74-year-old woman had undergone splenectomy 3 years earlier for unexplained pancytopenia and splenomegaly, at which time antinuclear antibody positivity was noted. She also had a history of chronic maxillary sinusitis (bilateral radical surgery in her teens). She presented with low-grade fever and headache, and was admitted on day 1 with a diagnosis of infection of a postoperative left maxillary cyst. On day 2, incision and drainage of the cyst were performed. Blood cultures were negative, and echocardiography revealed pericardial effusion without vegetations.
On day 10, she developed abdominal pain. Contrast-enhanced computed tomography (CT) demonstrated multiple hepatic artery aneurysms with contrast extravasation around the perihilar region, suggesting intraperitoneal hemorrhage (Figure 1A-C). Emergency transcatheter arterial embolization (TAE) of the segment 5 branch achieved hemostasis with coil placement (Figure 1D and E).
Contrast-enhanced CT and angiography at symptom onset.Contrast-enhanced CT obtained immediately after the onset of abdominal pain shows multiple hepatic artery aneurysms.(A) Axial arterial-phase image and (B) coronal arterial-phase image demonstrate several aneurysms. Intraperitoneal hemorrhage originating from the A5 branch is suspected (yellow arrow), and a hematoma is present in the hepatic hilum (red arrow). No arterial aneurysms were identified in locations other than the liver.(C) Three-dimensional reconstructed CT highlights the extravasation at the A5 branch (yellow arrow).(D) Angiography confirms contrast extravasation from the same site (yellow arrow).(E) Coil embolization was performed at the A5 branch (yellow arrow), clearly showing coil deployment at the bleeding site.CT: computed tomography.
Serologic testing was positive for antinuclear antibodies, anti-double-stranded DNA antibodies, lupus anticoagulant, and anti-cardiolipin β2 glycoprotein I antibodies. Additional findings included pericardial effusion, hypocomplementemia, proteinuria, hemolytic anemia (low haptoglobin, positive direct Coombs test) (Table 1), and erythema of the right upper arm, right palm, and anterior chest. No pulmonary or gastrointestinal lesions were observed. She was diagnosed with SLE. Treatment with glucocorticoids and cyclophosphamide was initiated, leading to rapid radiological improvement of the hepatic artery aneurysms; regression was noted on day 14 of treatment, and follow-up CT at 6 months showed near-complete resolution but also to significant clinical and laboratory improvement. Anti-double-stranded DNA antibody levels decreased, proteinuria was reduced, pericardial effusion disappeared, and anemia and hemolytic findings were ameliorated.
Discussion
Etiologies of hepatic artery aneurysms include infection, atherosclerosis, fibromuscular dysplasia, vasculitis, polyarteritis nodosa, and SLE ^(3), (4)^. In autoimmune diseases, aneurysm formation is thought to result from vasculitis-induced medial layer destruction and immune cell infiltration ^(5)^. In this case, the pancytopenia 3 years earlier suggests that undiagnosed SLE had been present. The absence of positive blood cultures and of vegetations indicating infective endocarditis reduced the likelihood of an infectious aneurysm. Furthermore, regression of the aneurysms after immunosuppressive therapy supported an inflammatory etiology.
Endovascular treatment, such as TAE or coil embolization, is minimally invasive and offers benefits including shorter hospitalization and fewer postoperative complications. Open surgery, although more invasive, may provide definitive and durable treatment in cases of complex or large aneurysms ^(6)^. Hepatic artery aneurysms carry a clear rupture risk (approximately 14%), and rupture is associated with high mortality ^(3)^. Therefore, prompt diagnosis and appropriate therapeutic intervention are essential for improving prognosis. In this patient, rupture occurred during hospitalization, but timely endovascular intervention successfully achieved hemostasis and a favorable outcome.
While prior cases presented mainly with gastrointestinal bleeding or hemobilia, our patient developed acute abdominal pain from aneurysmal rupture during hospitalization ^(4), (7), (8)^. Endovascular embolization was the initial treatment in most cases, including ours, and all patients had favorable outcomes with timely intervention (Table 2).
This case highlights that rapid diagnosis, prompt hemostatic intervention, and early initiation of immunosuppressive therapy are critical for achieving favorable outcomes in SLE-associated hepatic artery aneurysms.
Article Information
Author Contributions
Saori Inoue: patient care, manuscript drafting. Mari Tatsumi, Yu Tanaka: clinical data interpretation, and literature review. Aya Ide: image preparation and editing.
Conflicts of Interest
None.
Ethics Approval and Consent to Participate
This case report did not require approval by the institutional review board, in accordance with the policy of Meitetsu hospital. Written informed consent for publication was obtained from the patient .
Acknowledgements
None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tamura H, Ozono Y, Uchida K, et al. Multiple intrahepatic artery aneurysms during the treatment for Ig G 4-related sclerosing cholangitis: a case report. World J Hepatol. 2024;16(12):1505-14.39744203 10.4254/wjh.v 16.i 12.1505 PMC 11686534 · doi ↗ · pubmed ↗
- 2Boukobza M, Ilic-Habensus E, Arregle F, et al. Hepatic artery aneurysms in infective endocarditis: report of 10 cases and literature review. Ann Vasc Surg. 2024;105:252-64.38574810 10.1016/j.avsg.2024.01.013 · doi ↗ · pubmed ↗
- 3Abbas MA, Fowl RJ, Stone WM, et al. Hepatic artery aneurysm: factors that predict complications. J Vasc Surg. 2003;38(1):41-5.12844087 10.1016/s 0741-5214(03)00090-9 · doi ↗ · pubmed ↗
- 4Pollono EN, Madoff DC, Spence SC, et al. Multiple hepatic artery aneurysms in a patient with systemic lupus erythematosus. Lupus. 2010;19(1):93-5.19884215 10.1177/0961203309345721 · doi ↗ · pubmed ↗
- 5Corominas H, Tsokos M, Quezado M, et al. Aneurysm of the ascending aorta in systemic lupus erythematosus: case report and review of the literature. Eur J Rheumatol. 2017;4(2):133-5.28638687 10.5152/eurjrheum.2017.17066 PMC 5473449 · doi ↗ · pubmed ↗
- 6Song C, Dong J, Yu G, et al. Comparison of open surgery and endovascular procedures as a therapeutic choice for visceral artery aneurysms. Vascular. 2018;26(4):387-92.29228875 10.1177/1708538117744102 · doi ↗ · pubmed ↗
- 7Liu C, Tang QB, Zeng H, et al. Clinical and pathological analysis of hepatic artery aneurysm in a patient with systemic lupus erythematosus: report of a case. Surg Today. 2011;41(11):1571-4.21969165 10.1007/s 00595-010-4470-2 · doi ↗ · pubmed ↗
- 8Trambert J, Reinitz E, Buchbinder S. Ruptured hepatic artery aneurysms in a patient with systemic lupus erythematosus: case report. Cardiovasc Intervent Radiol. 1989;12(1):32-4.2496925 10.1007/BF 02577123 · doi ↗ · pubmed ↗